On-site Interview Questions
On-Site Installation Evaluations
20240222_OSIE_DP 6 Prevention Personnel
On-site Interview Questions
OMB: 0704-0610
DISCUSSION PROTOCOL 6
PREVENTION PERSONNEL DP6
Required
Materials:
OFR
POC Sheet
Resource
POC Sheet
Figures
1-4
Prevention
Survey (QR code, link, and/or paper versions)*
Pens
(if using paper surveys)
Audience: Integrated Prevention Teams; Resilience Teams; Behavioral Health Provider; Sexual Assault Prevention and Response; Victim Advocate; Chaplain; Suicide Prevention; Substance Abuse Prevention; Family Advocacy; and Equal Opportunity
Guidance to data collectors: Count the number of personnel in the room and tell the note-taker. Annotate the count in Question 1 response box.
Each question corresponds to specific data elements and specific sub-dimensions, which are listed in the boxes to the left. |
—START—
SCREENER
S1. Do you have any prevention responsibilities? For example, do you:
Run prevention programs of any kind?
Refer Service members that may be in need of mental or physical care?
Conduct education or awareness activities to educate Service members about available resources to deal with harmful behaviors?
Conduct evaluation of any prevention efforts?
Oversee prevention staff?
[Note: IF YES, proceed to Q1 below. IF NO, move over to PREVENTION SUPPORT DP7 protocol.]
DIMENSION 2: INTEGRATED PREVENTION – PRIORITY
Let’s start with some questions about primary prevention efforts here. Primary prevention focuses on stopping self-directed and other-directed harm BEFORE they occur. We’re especially interested in integrated prevention – which means simultaneously addressing multiple types of harm to self and others in a cohesive approach – for example, by addressing shared risk factors and avoiding duplication of efforts.

2.2.1
Does your leadership recognize or reward those who engage in prevention best practices, such as development of creative or interactive prevention activities, or conducting high-quality evaluations of prevention initiatives?IF YES: Please tell us about the rewards or recognitions presented and why.
IF NO: Why not?
Reminder, if needed: By your leadership, we mean your immediate supervisor and other leaders above in your chain of command.
2.4.1
Do you feel like your leadership has voiced support for or talked about the importance of primary prevention activities?
Reminder, if needed: By your leadership, we mean your immediate supervisor and other leaders above in your chain of command.

2.1.1
How do you keep track of whether planned prevention efforts are carried out?
DIMENSION 5: INTEGRATED PREVENTION – PREPARATION
Next, we would like to hear about the people working in prevention here and how they are supported by others here and beyond.
5.1.2
Since integrated prevention is an evolving field, how do you stay on top of the latest developments and learn from other installations or Services?
Do you go to any trainings? [If they go to training, confirm whether they have attended a training in the past year related to prevention and ask the following probes. If needed, ask for a brief description of the training topic and how it relates to prevention.]
Was the training interactive or just a presentation or PowerPoint?
How long was the training?
Who delivered the training? Does this group/organization have documented expertise in the training area?
How do you learn from other installations or Services? Or from others at your installation?

5.3.2
Do you think that there are enough people whose primary role is working to prevent Service members from dying by suicide; misusing alcohol; assaulting, harassing, discriminating against, or bullying others; and engaging in other forms of interpersonal violence here?
IF YES: How do you know?
IF NO: Which office(s) or prevention areas (e.g., alcohol prevention, harassment prevention) would you say are understaffed?
5.4.1
When there is turnover in people working to prevent the harmful behaviors we just discussed, is there sufficient overlap to allow the needed transition of duties? Or is there a gap in filling that role?
5.4.2
When there is turnover in prevention positions, has the quantity and quality of prevention work remained the same? Or have you noticed a decline? If so, why do you think that is happening?
DIMENSION 8: INTEGRATED PREVENTION – IMPLEMENTATION
Next, we’re going to ask some questions about the primary prevention efforts here. Primary prevention focuses on stopping self-directed and other-directed harm BEFORE they occur or, in other words, getting out in front of potential problems.
8.1.4
Using this handout and thinking about all the efforts here to prevent Service members from dying by suicide; misusing alcohol; assaulting, harassing, discriminating against, or bullying others; and engaging in other forms of interpersonal violence, which number on this scale best characterizes how prevention offices and staff work?
Can you explain why you selected that level of interaction?
IF NEEDED:
Can you share some examples of ways those prevention assets work together?
8.1.1
With multiple prevention efforts in place, how do you or others ensure that programming is not redundant?
8.1.3
To what extent do you feel that different prevention offices understand the roles and responsibilities of other prevention offices?
Finally, we would like to hear more about your specific prevention responsibilities. Earlier, you mentioned that your prevention responsibilities include [RESPONSE FROM SCREENER]. I would like to learn more about those responsibilities and how they fit into the overall prevention approach here.
8.2.1
8.1.2
First, let’s talk about the prevention activities that you’re responsible for [IF EVALUATION ONLY, proceed to Question 12]. [Use charts to facilitate these questions and have them point to those that are relevant to their prevention activity. Make sure to ask them how those factors are targeted to ensure they are not just picking random things that their work indirectly targets or is adjacent to.]
Looking at the risk factors and protective factors on the handout, which risk and protective factors are targeted by your prevention programming?
How are these factors chosen?
Are there any risk or protective factors you include in your programming that are not listed below?
F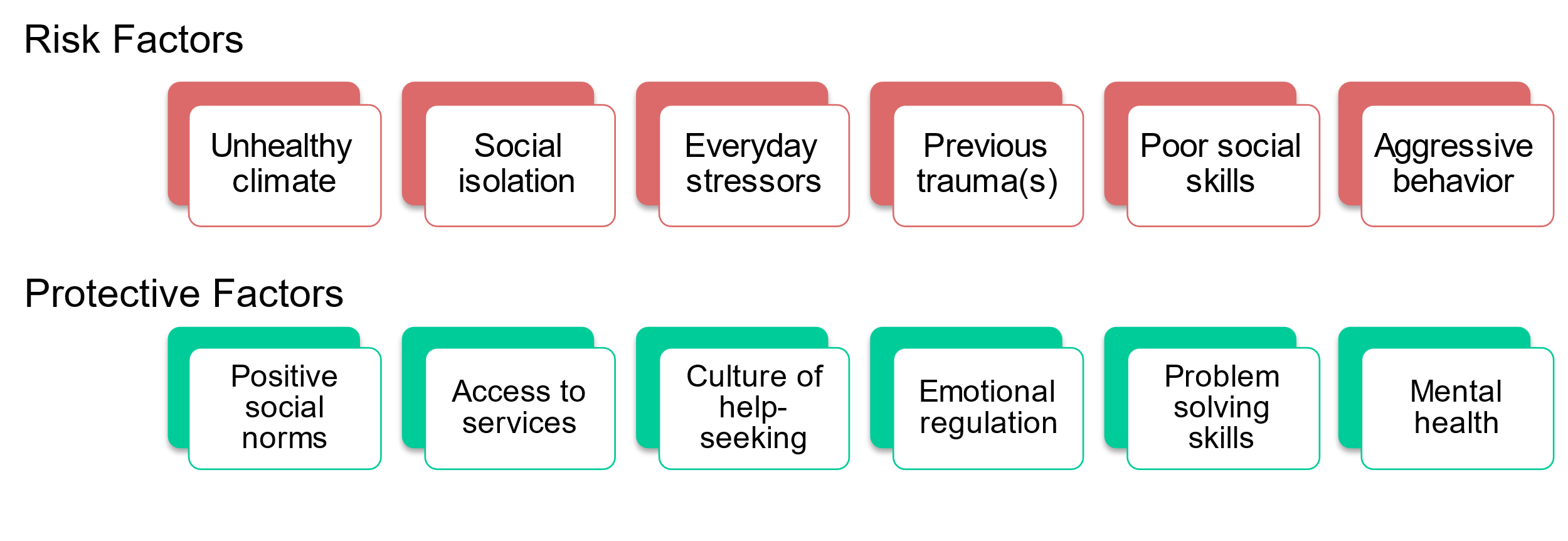
igure
2.
Risk and Protective Factors
8.2.2
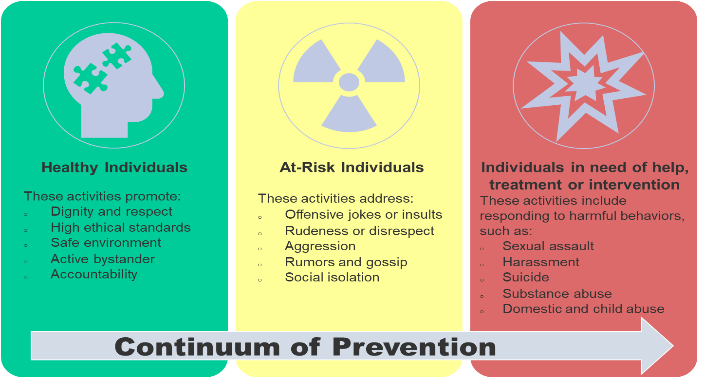
How do your prevention activities align with the continuum of prevention?
Continuum of prevention means that there are prevention activities for individuals who are healthy, those who are at-risk, and those who are in need of help or treatment, and that are tailored to each of these types of individuals.
Using this handout as a guide, please provide examples of your prevention activities that are targeted across the continuum of prevention.

Figure 3. Continuum of Prevention
Do your prevention activities address the entire continuum or is there an area of the continuum where you are more focused?
How do you tailor prevention activities for Service members in different stages of their careers?
-
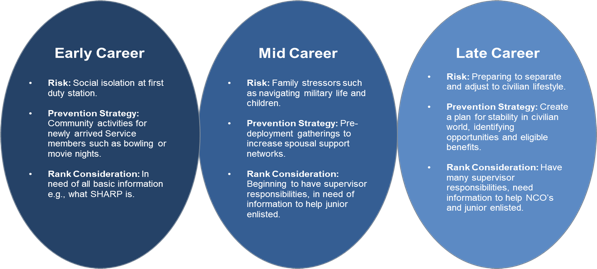
8.2.3
Prominent risk and protective factors vary throughout the career lifecycle, provide examples of targeted risk and protective factors for early career, mid-career, and late career. Based on each stage of one’s career there are different considerations of prevention information needed based on rank and supervisor responsibilities, provide examples of information provided to those in their early career, mid-career, and late career.
Figure
4.
Career Life Cycle
-
8.2.4
How do your prevention activities target different levels – specifically, individual Service members vs. units vs. the entire installation?

8.2
How do your prevention activities contribute to the overall prevention approach here?

8.3.1
Is there an ongoing evaluation of the prevention activities for which you are responsible?
IF NO, proceed to the next question.
IF YES:
What kinds of evaluation are used? For example, do you use surveys, focus groups, or interviews?
When does it occur (i.e., before an activity is getting started or after)?
Are evaluation efforts coordinated across offices responsible for prevention areas (e.g., alcohol, suicide, child abuse and neglect, domestic abuse, sexual assault, harassment)?
IF NO, proceed to the next question.
8.3.3
IF YES:
Are evaluation efforts ever rolled-up to provide an overarching picture of whether prevention is working across the installation or command?
IF YES: Could you give an example?

8.3.2
How do you communicate evaluation findings to your leadership and Service members here?

8.4.1
Do you use evaluation findings to improve prevention within the responsible offices and the overall prevention approach across the installation or command?
8.4.2
IF NO, proceed to the next question.
IF YES:
Can you provide an example of how this works?
What do you do if a prevention activity doesn’t seem to be working?
8.5.1
Do you monitor and address whether Service members are engaged and interested in prevention activities?
IF NO, proceed to the next question.
IF YES:
Is there data to support this? How do you assess engagement or resistance to prevention activities?

8.5.2
What do you do when Service members have become resistant or fatigued towards certain prevention activities?
How do Service members typically access support services related to harmful behaviors? Are there any issues or concerns that you have regarding access to support services?
Is there anything else important that you’d like us to be aware of or consider as it pertains to how harm to self or others is prevented or addressed within your unit or across your installation?
CONCLUSION/TRANSITION TO PREVENTION SURVEY
[DISPLAY QR CODE/SURVEY LINK TO PREVENTION SURVEY OR BEGIN PASSING OUT PAPER COPY AND PENS TO EACH PARTICIPANT.]
Before you leave, we would like to ask you to take about 5-8 minutes to complete a very short survey. The survey is anonymous. [IF COMPLETING ON PAPER: Please do not put your name on it.] We will NOT be looking at your individual responses. There are NO right or wrong answers to the survey, so please just respond based on your view. If you could please complete the survey before you leave today, that would be much appreciated. [IF COMPLETING ON PAPER: Please place your completed survey in this envelope.]
Thank you very much for spending time with us today and answering our questions. The information you provided is extremely valuable and useful to us.
Updated 2/22/2024
| File Type | application/vnd.openxmlformats-officedocument.wordprocessingml.document |
| Author | Flaspohler, Paul D. Dr. |
| File Modified | 0000-00-00 |
| File Created | 2025-02-28 |
© 2026 OMB.report | Privacy Policy