Individuals and Households Respondents
Study of Nutrition and Activity in Child Care Settings II (SNACS-II)
H3_Parent Interview for In-Care Day
Individuals and Households Respondents
OMB: 0584-0669
H3. Parent Interview for In-Care Day
This page has been left blank for double-sided copying.
OMB
Number: 0584-XXXX
Expiration
Date: XX/XX/20XX

Study of Nutrition and Activity in Child Care Settings II (SNACS-II)
Parent Interview for In-Care Day
The Food and Nutrition Service (FNS) is collecting this information to understand the nutritional quality of CACFP meals and snacks, the cost to produce them, and dietary intakes and activity levels of CACFP participants. This is a voluntary collection and FNS will use the information to examine CACFP operations. The collection does request personally identifiable information under the Privacy Act of 1974. Responses will be kept private to the extent provided by law and FNS regulations. According to the Paperwork Reduction Act of 1995, an agency may not conduct or sponsor, and a person is not required to respond to, a collection of information unless it displays a valid OMB control number. The valid OMB control number for this information collection is 0584-xxxx. The time required to complete this information collection is estimated to average 0.75 hours (45 minutes) per response, including the time for reviewing instructions, searching existing data sources, gathering and maintaining the data needed, and completing and reviewing the collection of information. Send comments regarding this burden estimate or any other aspect of this collection of information, including suggestions for reducing this burden, to: U.S. Department of Agriculture, Food and Nutrition Service, Office of Policy Support, 1320 Braddock Place, 5th Floor, Alexandria, VA 22314. ATTN: PRA (0584-xxxx). Do not return the completed form to this address. |
INTRODUCTION
VOICEMAIL SCRIPT: Hello, this message is for [CONSENTED PARENT NAME]. This is [INTERVIEWER NAME] from the second Study of Nutrition and Activity in Child Care Settings, or SNACS-II.
IF INTERVIEW NOT STARTED: We were calling to ask you about the foods and drinks [CHILDNAME] had [yesterday/ on ##DAY] and their activities. Please call our toll-free number, [insert #], today to schedule the interview appointment. The interview will take no more than 45 minutes. After you complete the interview, we will send you a $20 gift card. We look forward to speaking with you today.
IF INTERVIEW STARTED BUT NOT COMPLETE (BREAKOFF OR DATA RETRIEVAL): We had scheduled an interview with you today. Please call our toll-free number, [insert #], to reschedule your interview. After you complete the interview, we will send you a $20 gift card. We look forward to speaking with you.
INTRO: Hello, my name is [INTERVIEWER NAME] from Westat. I am calling about the second Study of Nutrition and Activity in Child Care Settings. May I please speak to [CONSENTED PARENT NAME]?
RESPONDENT ON PHONE GO TO CONSENT
NEW RESPONDENT COMES TO PHONE [REPEAT INTRO]
RESPONDENT NOT AVAILABLE [SCHEDULE CALLBACK]
WRONG NUMBER [DISPO AS WRONG NUMBER – PERSON]
GATEKEEPER REFUSAL [SOFT REFUSAL]
DO NOT WISH TO PARTICIPATE I’m sorry to hear that you do not wish to participate. The information you would have provided is very valuable to improving the program. Can you tell me the reason for choosing not to participate? ADDRESS ISSUES/CONCERNS GO TO REFUSAL CONVERSION]1
CONSENT: IF FIRST INTERVIEW: Thank you for taking part in the second Study of Nutrition and Activity in Child Care Settings. USDA is interested in learning about nutrition and activity habits of children. I understand that your child went to [Center/Provider/Afterschool Program] [yesterday/(DAY)]. I would like to ask you some questions about your child’s food and activity [yesterday/(DAY)] and some questions about your household. Your answers will help us improve services and better meet the needs of parents who send their children to child care programs.
The interview will take no more than 45 minutes and you will receive a $20 gift card to thank you for your participation.
This interview is voluntary. That means you can skip any question and you can stop at any time. Taking part in this study will not affect your benefits in any way – either now or in the future. Your information will be kept private and used only for research purposes according to state and federal law. We will not include information that identifies you or your family members in any report. The responses of all parents taking part in the study will be combined for reporting purposes. GO TO Q1.
IF DATA RETRIEVAL INTERVIEW FOR ASA24 ONLY: I would like to get the details about the foods and drinks your child had [DAY] that you were unable to report during our call [earlier/yesterday/(DAY)]. GO TO Q4
IF DATA RETRIEVAL FOR ASA24 AND ADMINISTERING SECTIONS B-F: I would like to get the details about the foods and drinks [CHILDNAME] had [DAY] that you were unable to report during our call [yesterday/(DAY)], and then ask you about [CHILDNAME]’s physical activity and some general information about your household. GO TO Q4.
IF ADMINISTERING SECTIONS B-F ONLY: I would like to ask about [CHILDNAME]’s physical activity and complete the interview about your household. GO TO SECTION B.
Do you agree to participate?
Yes
No I’m sorry to hear that you do not wish to participate. The information you would have provided is very valuable to improving the program. Can you tell me the reason for choosing not to participate? ADDRESS ISSUES/CONCERNS GO TO REFUSAL CONVERSION
IF CHILD GENDER MISSING, CONTINUE; ELSE GO TO INSTRUCTIONS FOR Q3.
Is [CHILDNAME] a boy or girl?
Boy
Girl
REFUSED
IF CHILD DATE OF BIRTH MISSING, CONTINUE; ELSE GO TO Q4.
What is [CHILDNAME]’s current age?
___ ___ years
DON’T KNOW
REFUSED
I would like to start by asking about foods and drinks [CHILDNAME] had [yesterday/(DAY)]. [IF CHILD ATTENDS AR/OSHCC: You may wish to have [CHILDNAME] be present for the first part of the interview with you, so [she/he] can provide details about the foods and drinks [she/he] had [yesterday/(DAY)]. After getting this information, we can continue with the rest of the interview with you. [CHILDNAME] does not have to be on the phone for these questions.] Did you write down what [CHILDNAME] had to eat and drink [yesterday/(DAY)] when not in child care in your Child Food Diary?
Yes GO TO Q4.1
No IF CHILD ATTENDS AR/OSHCC: GO TO Q4.2; ELSE GO TO Q4.3
And do you have your Child Food Diary with you? I will wait while you get it.
Yes GO TO Q5
No IF CHILD ATTENDS AR/OSHCC: GO TO Q4.2; ELSE GO TO Q4.3
Is [CHILDNAME] available now to assist with the interview?
Yes GO TO Q5
No GO TO Q4.3
Are you able to tell me about foods and drinks [CHILDNAME] had [yesterday/(DAY)] when not in child care?
Yes GO TO Q5
No Because you don’t have the information about foods and drinks [CHILDNAME] had [yesterday/(DAY)] when not in child care [IF CHILD ATTENDS AR/OSHCC: and [CHILDNAME] is not available to help with the interview], we can reschedule that part of the interview for later. We can complete the other questions I have for you now. This should take about 15 minutes.
Do you have any questions about the interview before I begin?
Yes ADDRESS QUESTIONS/CONCERNS ABOUT STUDY, THEN PROCEED.
No
IF PARENT ANSWERED ‘NO’ TO Q4.3, GO TO SECTION B.
SECTION A: ASA24
I would like to ask about what [CHILDNAME] had to eat and drink [yesterday/(DAY)] from midnight to midnight.
Since we observed the foods and beverages [CHILDNAME] had while at [Center/Provider/Afterschool Program], you do not need to report anything that [Center/Provider/Afterschool Program] provided. But, if [CHILDNAME] brought any foods or drinks from home to [Center/Provider/Afterschool Program], please be sure to tell me about them. Please include all foods eaten at home, [[IF CHILD ATTENDS AR/OSHCC: while at school – including foods brought from home to school, as well as any foods] shared by friends, purchased at the store, a fast food place, or restaurant.
To help you report the amounts of foods and beverages that [CHILDNAME] had [yesterday/on (DAY)]], I may ask you to look at the pictures in the Food Model Booklet, or you can use your own measuring cups and spoons. Do you have the Food Model Booklet ready to help with the interview?
Yes
No Do you have your own measuring cups and spoons available to help with the interview?
Yes I will wait a few minutes while you get them.
No That is fine, we can still do the interview now.
LAUNCH ASA24
Exhibit A: Meal-based Quick List Screenshot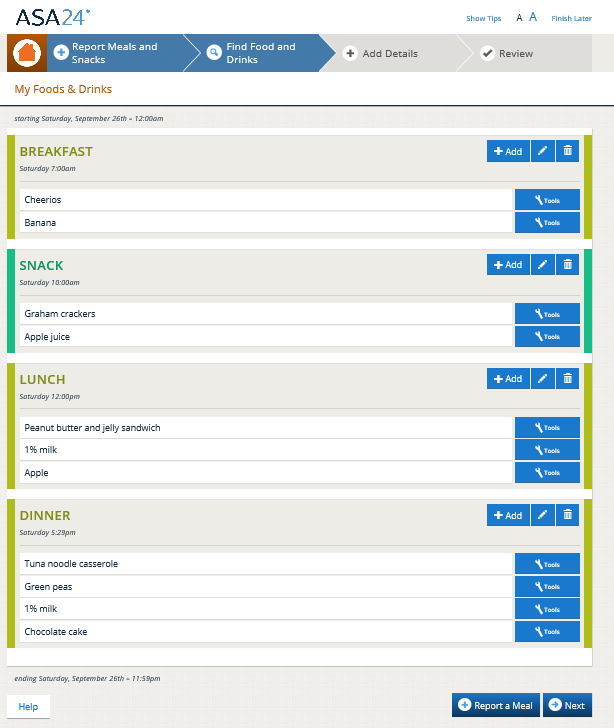
Exhibit B. Detail Screenshot (Example question)

Exhibit C. Review Screenshot

Exhibit D. Forgotten Foods List Screenshot (Example question)
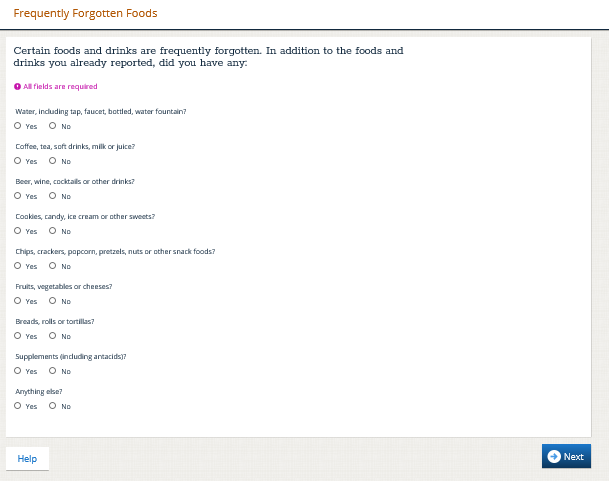
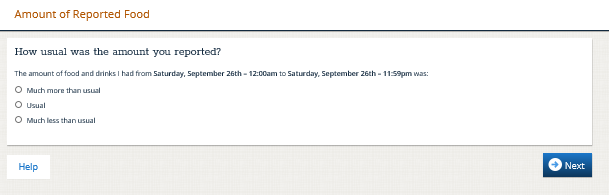
Exhibit E. Usual Amount Screenshot
INTERVIEWER: NEEDS DATA RETRIEVAL:
No
Yes
INTERVIEWER: RECORD WHO COMPLETED THE ASA24:
Parent only
Child and parent together
Child only
IF SECTIONS B-F COMPLETED FIRST (PARENT ANSWERED ‘NO’ TO Q4.3 AND CONTINUED WITH INTERVIEW BEFORE RETURNING TO ASA24 IN SECTION A), GO TO CONCLUSION.
SECTION B: FOODS AND BEVERAGES IN CHILD CARE
IF CHILD PRESENT FOR ASA24: Thank you, [CHILDNAME], for talking with me. Now I would like to talk with [CONSENTED PARENT NAME], and you don’t have to be on the call anymore.
Now I am going to ask you some questions about [CHILDNAME]’s schedule and the meals and snacks [she/he] eats at [Center/Provider/Afterschool Program].
IF PARENT CANNOT CONTINUE (BREAKOFF): GO TO CONCLUSION
Thinking about a typical week, does [CHILDNAME] go to [Center/Provider/Afterschool Program] on…
PROGRAMMER: DISPLAY Q6.1 OR DISPLAY Q6.2 AND Q6.3, BASED ON PROVIDER SAMPLE.
Goes to [Center/ Provider/Afterschool Program] on: |
Q6.1. If Q6=YES AND CHILD ATTENDS ECC/FDCH: At what time do you usually drop off and pick up [CHILDNAME] from [Center/Provider/]? |
Q6.2. IF Q6=YES AND CHILD ATTENDS AR/OSHCC: Did [CHILDNAME] attend child care before school? And how many hours did [she/he] spend at Center/ Provider/Afterschool Program] before school? |
Q6.3. IF Q6=YES AND CHILD ATTENDS AR/OSHCC: Did [CHILDNAME] attend child care after school? And how many hours did [CHILDNAME] spend at [Center/ Provider/Afterschool Program] after school? |
||||||
INTERVIEWER: MARK DAYS ATTENDED AND ENTER HOURS FOR THOSE DAYS. |
|||||||||
|
DK |
No |
Yes |
Drop-off time |
Pick-up time |
Before school care |
# hours before school |
After school care |
# hours after school |
Monday? |
|
|
|
|
|
□ |
|
□ |
|
Tuesday? |
|
|
|
|
|
□ |
|
□ |
|
Wednesday? |
|
|
|
|
|
□ |
|
□ |
|
Thursday? |
|
|
|
|
|
□ |
|
□ |
|
Friday? |
|
|
|
|
|
□ |
|
□ |
|
Saturday? |
|
|
|
|
|
□ |
|
□ |
|
Sunday? |
|
|
|
|
|
□ |
|
□ |
|
Q6.4 [IF CHILDNAME ATTENDS AR/OHSCC:] [Yesterday/On (DAY)], did your child attend [Center/Provider/Afterschool program] either before or after school?
Before school only
After school only
Both before and after school
DON’T KNOW
REFUSED
And do you usually send [CHILDNAME] to [Center/Provider/Afterschool Program] with a meal or snack from home, such as a brown bag lunch or snack?
INSTRUCTIONS: For children ≤3 years old only: This includes formula or breast milk.
Yes GO TO Q7.2
No GO TO Q7.1
Is this because the program does not allow food from home?
Yes GO TO SECTION C
No GO TO SECTION C
And on how many days each week do you usually send a meal or snack from home?
DAYS PER WEEK [Range 1-7]: ______
DON’T KNOW GO TO Q8
REFUSED GO TO Q8
What meals and snacks do you usually send from home? [CHECK ALL THAT APPLY]
INTERVIEWER: Mark all that apply.
Breakfast
Lunch
Dinner
Morning Snack
Afternoon Snack
Evening Snack
Which of the following reasons describe why you send food from home?
Reason for sending food from home |
CODE ONE PER ROW |
|||
YES |
NO |
DON’T KNOW |
REFUSED |
|
|
□ |
□ |
□ |
□ |
|
□ |
□ |
□ |
□ |
|
□ |
□ |
□ |
□ |
|
□ |
□ |
□ |
□ |
|
□ |
□ |
□ |
□ |
|
□ |
□ |
□ |
□ |
|
□ |
□ |
□ |
□ |
PROGRAMMER: DISPLAY ONLY IF CHILD IS ≤3 YEARS OLD |
||||
|
□ |
□ |
□ |
□ |
PROGRAMMER: DISPLAY ONLY IF CHILD IS ≤3 YEARS OLD |
||||
|
□ |
□ |
□ |
□ |
PROGRAMMER: DISPLAY FOR ALL AGES: |
||||
______________________ |
□ |
□ |
□ |
□ |
SECTION C: CHILD’S PHYSICAL ACTIVITY
Now I am going to ask you about [CHILDNAME]’s activities.
How active do you consider [CHILDNAME] to be?2
Very active
Active
Somewhat active
Not at all active
Don’t know
Refused
During the past week, on how many weekdays did [CHILDNAME] watch TV or videos when [she/he] was not in child care or school? 3 Do not include weekend days—Saturday or Sunday.
ENTER NUMBER OF DAYS BETWEEN 0 and 5 |__| IF 0 DAYS, GO TO Q12
DON’T KNOW
REFUSED
And on those days, about how much time did [CHILDNAME] usually spend watching TV or videos?4 Please include only times when the primary activity was watching TV or videos.
Less than one hour per day
1 hour per day
2 hours per day
3 hours per day
4 hours per day
5 hours or more per day
DON’T KNOW
REFUSED
Now I am going to ask you about the time [CHILDNAME] spends playing video or computer games, or using an electronic device for something that was not school work. For these questions, do not include time when [she/he] is at child care or school or weekend days—Saturday or Sunday—or using the computer for school work.
During the past week, on how many weekdays did [CHILDNAME] play video or computer games or use an electronic device such as IPad, computer, smart phone for something that was not school work? 5
ENTER NUMBER OF DAYS BETWEEN 0 and 5 |__| IF 0 DAYS, GO TO Q14
DON’T KNOW
REFUSED
And on those days, how much time did [CHILDNAME] usually spend playing video or computer games or using an electronic device for something that was not school work?6 Please include only times when the primary activity was playing video or computer games or using an electronic device for something that was not school work.
Less than one hour per day
1 hour per day
2 hours per day
3 hours per day
4 hours per day
5 hours or more per day
DON’T KNOW
REFUSED
The next few questions are about sitting time, excluding time spent watching TV or on the computer.
During the past week on weekdays, about how much time did [CHILDNAME] spend sitting in a vehicle to get to and from places, including school and child care? Do include weekend days—Saturday or Sunday.7
ENTER NUMBER (OF MINUTES OR HOURS) |__||__||__|.|__|
Minutes
Hours
DON’T KNOW
REFUSED
During the past week, on weekdays, about how much time did [CHILDNAME] usually spend sitting, doing things such as homework, reading, or playing cards or board games? Please do not include time spent on the computer. Do not include weekend days – Saturday or Sunday.8
0 hours per day
Less than one hour per day
1 hour per day
2 hours per day
3 hours per day
4 hours per day
5 hours or more per day
DON’T KNOW
REFUSED
The next few questions are about activities that increase heart rate and make the child breathe hard. Some examples of these activities include biking; brisk walking; swimming; dancing; competitive sports; or playing active video games such as Nintendo, Xbox, PlayStation, Wii, Oculus or other virtual reality systems.9
During the past week when [CHILDNAME] was not at child care or school, on how many weekdays did [she/he] do activities that increased [his/her] heart rate and made [him/her] breathe hard? Do include weekend days—Saturday or Sunday.10
ENTER NUMBER OF DAYS BETWEEN 0 and 5 |__| IF 0 DAYS, GO TO Q18
DON’T KNOW
REFUSED
And on those days, about how much time did [CHILDNAME] usually spend doing these activities?11
Less than one hour per day
1 hour per day
2 hours per day
3 hours per day
4 hours per day
5 or more hours per day
DON’T KNOW
REFUSED
During the past week when [CHILDNAME] was not at child care or school, on how many weekdays did [she/he] play outdoors? Do not include weekend days—Saturday or Sunday.
ENTER NUMBER OF DAYS BETWEEN 0 and 5 |__| IF 0 DAYS, GO TO Q20
DON’T KNOW
REFUSED
And on those days, about how much time did [CHILDNAME] usually spend playing outdoors?12
Less than one hour per day
1 hour per day
2 hours per day
3 hours per day
4 hours per day
5 hours per day
DON’T KNOW
REFUSED
SECTION D: HOUSEHOLD MEMBERS
Including yourself and [CHILDNAME], how many people live in your household? Don’t forget to include non‑relatives who live here and, of course, babies, small children and foster children. Also include persons who usually live here but are temporarily away for reasons such as: vacation, traveling for work, or in the hospital. Do not include children living away at school.
NUMBER OF PEOPLE [RANGE 2-20]: ________
DON’T KNOW
REFUSED
Of the number of people in your household, how many are children currently 5 to 18 years of age?
NUMBER OF CHILDREN AGED 5 to 18: ______________
Of the number of people in your household, how many are children currently less than 5 years old?
NUMBER OF CHILDREN LESS THAN 5 YEARS OLD: ______________
DISPLAY Q23 IF (1) THE SUM OF Q21 + Q22>1 OR (2) THE SUM OF Q21 + Q22 = 1 AND AGE OF [CHILDNAME] IS MISSING.
What is the age of the [IF Q21 + Q22>1: oldest] child in your household? |__|__| YEARS
Do you consider [CHILDNAME] to be Hispanic or [Latino/Latina]? [IF NECESSARY: A person of Cuban, Mexican, Puerto Rican, South or Central American, or other Spanish culture or origin, regardless of race.]
Hispanic or [Latino/Latina]
Not Hispanic or [Latino/Latina]
REFUSED
What race do you consider [CHILDNAME] to be? Please choose one or more of the following.
American Indian or Alaska Native
Asian
Black or African American
Native Hawaiian or Other Pacific Islander
White
REFUSED
SECTION E: FOOD SECURITY
These next questions are about the food eaten in your household in the last month and whether you were able to afford the food you need.
THROUGHOUT THIS SECTION, ENTER APPROPRIATE FILLS DEPENDING ON NUMBER OF ADULTS AND NUMBER OF CHILDREN IN THE HOUSEHOLD.
Which of these statements best describes the food eaten in your household in the last month: —enough of the kinds of food [I/we] want to eat; —enough, but not always the kinds of food [I/we] want; —sometimes not enough to eat; or, —often not enough to eat?
Enough of the kinds of food we want to eat
Enough but not always the kinds of food we want
Sometimes not enough to eat
Often not enough to eat
DON’T KNOW
REFUSED
Now I’m going to read you several statements that people have made about their food situation. For these statements, please tell me whether the statement was often true, sometimes true, or never true for [you/your household] in the last month.
The first statement is “[I/We] worried whether [my/our] food would run out before [I/we] got money to buy more.” Was that often true, sometimes true, or never true for [you/your household] in the last month?
Often true
Sometimes true
Never true
DON’T KNOW
REFUSED
“The food that [I/we] bought just didn’t last, and [I/we] didn’t have money to get more.” Was that often, sometimes, or never true for [you/your household] in the last month?
Often true
Sometimes true
Never true
DON’T KNOW
REFUSED
“[I/we] couldn’t afford to eat balanced meals.” Was that often, sometimes, or never true for [you/your household] in the last month?
Often true
Sometimes true
Never true
DON’T KNOW
REFUSED
IF "OFTEN TRUE" OR "SOMETIMES TRUE" TO ONE OR MORE OF Q27-Q29 OR, RESPONSE “SOMETIMES…” OR “OFTEN…” TO QUESTION Q26, CONTINUE TO Q30; OTHERWISE, GO TO INTRODUCTION TO Q35.
In the last month, did [you/you or other adults in your household] ever cut the size of your meals or skip meals because there wasn't enough money for food?
Yes GO TO Q30.1
No GO TO Q31
DON’T KNOW GO TO Q31
REFUSED GO TO Q31
[IF YES ABOVE, ASK] In the last 30 days, how many days did this happen?
|__|__| Days
DON’T KNOW
In the last month, did you ever eat less than you felt you should because there wasn't enough money for food?
Yes
No
DON’T KNOW
REFUSED
In the last month, were you ever hungry but didn't eat because there wasn't enough money for food?
Yes
No
DON’T KNOW
REFUSED
In the last month, did you lose weight because there wasn't enough money for food?
Yes
No
DON’T KNOW
REFUSED
IF AFFIRMATIVE RESPONSE TO ONE OR MORE OF QUESTIONS Q30-Q33, THEN CONTINUE TO Q34; OTHERWISE, GO TO INTRODUCTION TO Q35.
In the last month, did [you/you or other adults in your household] ever not eat for a whole day because there wasn't enough money for food?
Yes GO TO Q34.1
No GO TO INTRODUCTION TO Q35
DON’T KNOW GO TO INTRODUCTION TO Q35
REFUSED GO TO INTRODUCTION TO Q35
[IF YES ABOVE, ASK] In the last 30 days, how many days did this happen?
|__|__| Days
DON’T KNOW
INTRODUCTION TO Q35: Now I'm going to read you several statements that people have made about the food situation of their children. For these statements, please tell me whether the statement was often true, sometimes true, or never true in the last month for [your child/children living in the household who are under 18 years old].
“[I/we] relied on only a few kinds of low-cost food to feed [my/our] child/the children] because [I was/we were] running out of money to buy food.” Was that often, sometimes, or never true for [you/your household] in the last month?
Often true
Sometimes true
Never true
DON’T KNOW
REFUSED
“[I/We] couldn’t feed [my/our] child/the children] a balanced meal, because [I/we] couldn’t afford that.” Was that often, sometimes, or never true for [you/your household] in the last month?
Often true
Sometimes true
Never true
DON’T KNOW
REFUSED
"[My/Our child was/The children were] not eating enough because [I/we] just couldn't afford enough food." Was that often, sometimes, or never true for [you/your household] in the last month?
Often true
Sometimes true
Never true
DON’T KNOW
REFUSED
IF AFFIRMATIVE RESPONSE (I.E., "OFTEN TRUE" OR "SOMETIMES TRUE") TO ONE OR MORE OF QUESTIONS Q35-Q37, THEN CONTINUE TO Q38; OTHERWISE GO TO SECTION F.
In the last month, did you ever cut the size of [your child's/any of the children's] meals because there wasn't enough money for food?
Yes
No
DON’T KNOW
REFUSED
In the last month, did [CHILD’S NAME/any of the children] ever skip meals because there wasn't enough money for food?
Yes GO TO Q39.1
No GO TO Q40
DON’T KNOW GO TO Q40
REFUSED GO TO Q40
[IF YES ABOVE ASK] In the last 30 days, how many days did this happen?
|__|__| Days
DON’T KNOW
In the last month, [was your child/were the children] ever hungry but you just couldn't afford more food?
Yes
No
DON’T KNOW
REFUSED
In the last month, did [your child/any of the children] ever not eat for a whole day because there wasn't enough money for food?
Yes
No
DON’T KNOW
REFUSED
SECTION F: CHILD DEMOGRAPHICS & HOUSEHOLD PROGRAM PARTICIPATION
The final set of questions are about you and your household.
I’m going to read the names of some programs that provide food or meals to individuals or households.
Please tell me if you or anyone in your household has received benefits from these programs in the last 30 days.
SNAP [OR INSERT STATE SNAP PROGRAM NAME],13 also known as food stamps
WIC program, or the Special Supplemental Nutrition Program for Women, Infants and Children
[For households receiving WIC] [IF WIC=1: DISPLAY] Infant formula from WIC
[[IF CHILD ATTENDS AR/OSHCC: DISPLAY] Free meals at school
[IF ‘Free meals at school’=1: SKIP; IF CHILD ATTENDS AR/OSHCC: DISPLAY] Reduced-price meals at school
Food pantries, food banks, local soup kitchens, or emergency kitchens
[IF PROGRAM IS ON AN INDIAN RESERVATION OR CHILD CARE SITE IS IN OKLAHOMA: DISPLAY] Food Distribution Program on Indian Reservations, also called FDPIR
None of the above
DON’T KNOW
REFUSED
Does anyone in your household participate in Medicaid?
Yes
No
DON’T KNOW
REFUSED
Does anyone in your household receive income from the [INSERT STATE TANF NAME]? [IF NECESSARY: Temporary Assistance for Needy Families, or TANF, is a program that provides cash assistance and supportive services to assist families with children under age 18.]
Yes
No
DON’T KNOW
REFUSED
Is any child in the household currently covered by the [INSERT STATE CHIP NAME] or the Children’s Health Insurance Program?14 [IF NECESSARY: Children’s Health Insurance Program is free or low-cost health coverage for eligible children and other family members.]
Yes
No
DON’T KNOW
REFUSED
We would like your best estimate of your total annual household income before taxes in the year 2022. Please include all forms of income, including wages, salaries, interest, dividends, and other forms of income such as Social Security, SSI, or TANF for all household members.
INTERVIEWER: IF NON-SPECIFIC AMOUNT GIVEN, PROBE FOR SPECIFIC AMOUNT. AFTER PROBING, IF NON SPECIFIC AMOUNT STILL GIVEN, MARK ‘NON-SPECIFIC AMOUNT.’
$ |___|___|___| , |___|___|___| RECORD AMOUNT GO TO CONCLUSION
(0 – 999,999)
NON-SPECIFIC AMOUNT GO TO Q47
DON’T KNOW GO TO Q47
REFUSED GO TO Q47
Is your total household income less than or more than $50,000?
Less than $50,000 GO TO Q48
$50,000 or more GO TO Q49
DON’T KNOW GO TO CONCLUSION
REFUSED GO TO CONCLUSION
Now I am going to read you some income categories. Please tell me when I read the range that best represents your household’s income.
LESS THAN $5,000
$5,000 TO LESS THAN $10,000
$10,000 TO LESS THAN $15,000
$15,000 TO LESS THAN $20,000
$20,000 TO LESS THAN $25,000
$25,000 TO LESS THAN $30,000
$30,000 TO LESS THAN $40,000
$40,000 TO LESS THAN $50,000
DON’T KNOW
REFUSED
GO TO CONCLUSION
Now I am going to read you some income categories. Please tell me when I read the range that best represents your household’s income.
$50,000 TO LESS THAN $60,000
$60,000 TO LESS THAN $70,000
$70,000 TO LESS THAN $80,000
$80,000 TO LESS THAN $90,000
$90,000 TO LESS THAN $100,000
$100,000 OR MORE
DON’T KNOW
REFUSED
CONCLUSION
IF SECTION A (ASA24) NOT INITIATED/SKIPPED (PARENT ANSWERED ‘NO’ TO Q4.3):
IF CHILD ATTENDS ECC/FCCH GO TO C1
IF CHILD ATTENDS AR/OSHCC CONTINUE
I would like to check, is [CHILDNAME] available now to assist with the interview?
YES, available GO TO SECTION A (administer ASA24 interview)
NOT AVAILABLE GO TO C1
[NOTE TO REVIEWERS: For the 1st ICD, having sections B-F incomplete does not trigger another call – the conclusions depend on the ASA24. Sections B-F will be administered at every follow-up interview, as needed.]
IF NO USUAL INTAKE:
IF SECTION A (ASA24) COMPLETE: You have just given us valuable information for this study. We will mail you a $20 gift card for this interview. We would also like to schedule one more call to ask you about what [CHILDNAME] ate and drank on a day when [she/he] did not attend child care. [IF SECTIONS B-F NOT COMPLETE:] We can also complete the rest of today’s interview at that time.] The interview will take no more than 30 minutes and you will receive a $30 gift card after you complete the interview. GO TO C6
IF SECTION A (ASA24) NOT COMPLETE: You have just given us valuable information for this study. I would like to schedule two more calls with you. In the first call, we can finish talking about the foods and drinks your child had yesterday and then we can mail you the $20 gift card. In the second call, I will ask you about what your child had to eat and drink on a day [she/he] did not go to child care and we will mail you a $30 gift card after completing this call. GO TO C1
IF USUAL INTAKE: You have just given us valuable information for this study. Since food intake changes from day to day, I would like to schedule two more calls with you. The first call will be to ask about the foods and drinks [CHILDNAME] has on [DATE] when he/she will be in child care. In the second call, I will ask you about what your child had to eat and drink on a day [she/he] did not go to child care. We will mail you a $30 gift card after completing each interview. GO TO C2
May I call you later today or tomorrow? [IF CHILD ATTENDS AR/OSHCC: You may wish to have [CHILDNAME] participate in the interview with you, if [she/he] can provide details about what [she/he] had to eat and drink [yesterday/(DAY)]. [IF SECTIONS B-F NOT COMPLETE: We can also complete the rest of today’s interview at that time.].
YES
CALL BACK TODAY GO TO C5
CALL BACK TOMORROW (AUTO FILL DATE) GO TO C5
NO (PARENT NOT AVAILABLE FOR CALL BACK LATER TODAY OR TOMORROW) IF ASA24 NOT INITIATED GO TO SCHEDULE OUT OF CARE INTERVIEW; OTHERWISE: This interview will take no more than 10 minutes. When is the earliest we can call you to complete this interview?
DATE [WITHIN 3 DAYS OF INTERVIEW]: ______________ GO TO C5
IF DATE 3 DAYS AFTER INTERVIEW: In that case, I just need to schedule one more interview with you. GO TO SCHEDULE OUT OF CARE INTERVIEW
Will [CHILDNAME] attend child care on [SECOND MEAL OBSERVATION DAY]?
YES GO TO C3
NO IF ASA24 COMPLETE, GO TO SCHEDULE OUT OF CARE INTERVIEW; IF ASA24 NOT COMPLETE, GO TO C4
NOT SURE GO TO SCHEDULE OUT OF CARE DAY INTERVIEW.
REFUSED I’m sorry to hear that you no longer wish to participate. The information you would have provided is very valuable to improving the program. Can you tell me the reason for choosing not to participate? ADDRESS ISSUES/CONCERNS GO TO REFUSAL CONVERSION
May we call you on [DAY AFTER SECOND MEAL OBSERVATION DAY] to ask what [CHILDNAME] had to eat and drink on [DAY]? The interview will take no more than 30 minutes. [IF ASA24 NOT COMPLETE AND USUAL INTAKE: During this time, you can tell us the details about foods and drinks you were not able to provide for [yesterday/(DAY)]. [IF SECTIONS B-F NOT COMPLETE: and also complete the rest of today’s interview].
YES GO TO C5
NO In that case, may we call on [DATE] (2 DAYS AFTER OBSERVATION DAY)?
YES GO TO C5
NO IF ASA24 COMPLETE: In that case, I just need to schedule one more interview with you, GO TO SCHEDULE OUT OF CARE INTERVIEW; IF ASA24 NOT COMPLETE, GO TO C4
I would still like to get the details about yesterday’s foods and drinks. May I call you later today [or tomorrow IF THE CALL IS CLOSE TO END OF DAY] to get this information? [IF SECTIONS B-F NOT COMPLETE: We can also complete the rest of today’s interview at that time.]
YES
CALL BACK TODAY GO TO C5
CALL BACK TOMORROW (AUTOFILL DATE) GO TO C5
NO (PARENT NOT AVAILABLE FOR CALL BACK LATER TODAY OR TOMORROW) This interview will take no more than 10 minutes. When is the earliest we can call you to complete this interview?
DATE [WITHIN 3 DAYS OF INTERVIEW]: ______________ GO TO C5
IF DATE 3 DAYS AFTER INTERVIEW: In that case, I just need to schedule one more interview with you. GO TO SCHEDULE OUT OF CARE INTERVIEW
What time would you like us to call?
Time: ______________□ AM □ PM
SCHEDULE OUT OF CARE INTERVIEW
I would like to schedule one more call to ask you about what [CHILDNAME] ate and drank on a day when [she/he] did not attend child care. The interview will take no more than 30 minutes and you will receive a $30 gift card after you complete the interview.
Thinking about the next two weeks, when will your child not attend child care?
Day: ______________ Date: __________
Day: ______________ Date: __________
Day: ______________ Date: __________
Day: ______________ Date: __________
Day: ______________ Date: __________
Day: ______________ Date: __________
Day: ______________ Date: __________
Based on what you just told me, we would like to call you on: [ONE DAY AFTER FIRST AVAILABLE DAY AND DATE]
Does this work for you?
YES GO TO C8
NO GO TO ONE DAY AFTER NEXT AVAILABLE DAY AND IDENTIFY THE DAY THAT WORKS BEST.
Interview scheduled for: Date: ___ / ___ / ______ GO TO C8
REFUSED I’m sorry to hear that you no longer wish to participate. The information you would have provided is very valuable to improving the program. Can you tell me the reason for choosing not to participate? GO TO REFUSAL CONVERSION
What time should we call you?
Time: ______________□ AM □ PM
And is this [###-###-####] still the best number to reach you?
YES GO TO C10
NO What number should I call you at?
Telephone number: ___-___-____ GO TO C10
May we also send you a text message reminder at this telephone number?
YES GO TO CHILD FOOD DIARY REMINDER
NO Do you have a number we can use for a text message reminder?
YES Telephone number: ___-___-____. GO TO CHILD FOOD DIARY REMINDER
NO May we send you an email reminder at [EMAIL ADDRESS, IF EMAIL ADDRESS PROVIDED IN CONSENT]?
YES GO TO CHILD FOOD DIARY REMINDER
NO It looks like we are not able to send you a reminder. Please note that a member of the study team will be calling you on [DATE/TIME] GO TO CHILD FOOD DIARY REMINDER
CHILD FOOD DIARY REMINDER
IF DATA RETRIEVAL ONLY: Please remember to use your Child Food Diary to record the details you were not able to provide about the foods and drinks your child had on [DATE]. We look forward to talking with you soon. GO TO THANK YOU
IF DATA RETRIEVAL AND SECOND ICD SCHEDULED: Please remember to use your Child Food Diary to record the details about the foods and drinks your child had on [DATE] and also the foods and drinks your child has from midnight to midnight [tomorrow/(DAY)]. GO TO CHILD FOOD DIARY INSTRUCTIONS
IF NO DATA RETRIEVAL AND SECOND ICD SCHEDULED OR OCD SCHEDULED: Please use your Child Food Diary to record the details about all foods and drinks your child has from midnight to midnight [tomorrow/(DAY)]. GO TO CHILD FOOD DIARY INSTRUCTIONS
CHILD FOOD DIARY INSTRUCTIONS
As a reminder, you do not need to include any foods or drinks provided by [Center/Provider/Afterschool Program]. But, if [CHILDNAME] brought any foods or drinks from home to [Center/Provider/Afterschool Program], please be sure to write them down.]
Please write down all foods eaten at home, [IF CHILD ATTENDS AR/OSHCC: while at school – including foods brought from home to school, as well as foods] shared by friends, purchased at the store, fast food place, or restaurant.
If needed, talk with others who may have served foods and drinks to your child when your child was not in child care. [IF CHILD ATTENDS AR/OSHCC: You may wish to have [CHILDNAME] participate in the interview with you, if [she/he] can provide details about what [she/he] had to eat and drink [yesterday/(DAY)].
IF RESPONSE TO PARENT INTERVIEW Q4 AND Q4.1 = NO GO TO C11; OTHERWISE GO TO THANK YOU.
Do you still have the Child Food Diary we sent to you?
YES GO TO THANK YOU
NO Would you like me to send you the diary by email at [EMAIL ADDRESS]?
YES GO TO THANK YOU
NO
Send to a different email address: _______________________ GO TO THANK YOU
Not needed. To use your own paper, please be sure to record the time of day and/or the meal or snack at which your child had the food or drink, the name of the food or drink, and the amount your child had. GO TO THANK YOU
THANK YOU
Thank you very much for your participation in this interview.
IF DR REQUIRED AND INTERVIEW SCHEDULED: We look forward to talking with you soon. GO TO C12
IF DR REQUIRED AND INTERVIEW NOT SCHEDULED/PARENT REFUSED OR IF ASA24 COMPLETE: GO TO C12
I would like to confirm your name and mailing address so we can send you the $20 gift card. I have your name as [FIRST AND LAST NAME]. Is this correct?
YES
NO What is your name?
PROBE: Can you spell that for me?
FIRST NAME
LAST NAME
The address I have is [ADDRESS]. Is this correct?
YES
NO What is your current address?
PROBE: Is there an apartment number?
PROBE: This is where we will mail your gift card.
STREET 1: ___________________________________________________
STREET 2: ___________________________________________________
APT. #: ________________
CITY: ___________________________________________
STATE: ________________ (SELECT FROM DROP DOWN)
ZIP: ________________________
REFUSAL CONVERSION
I’m sorry to hear that you do not wish to participate. The information you would have provided is very valuable to improving the program. Can you tell me the reason for choosing not to participate?
IF: I don’t do surveys/don’t want my child to participate in a study.
ANSWER: I understand, but this study will help the U.S. Department of Agriculture understand the food and activities provided in child care settings. The results will help improve the program.
IF: I don’t know if you are who you say you are.
ANSWER: I can give you our 800 number to call and confirm the authenticity of the study.
IF: I don’t know how the results will be used.
ANSWER: The U.S. Department of Agriculture needs to periodically assess programs funded by the government. This study will help them understand the food and activities provided in child care settings, and this information may help improve child care programs.
IF: I don’t want the government to know about me/my child.
ANSWER: Researchers and program staff must follow all federal and state laws to protect your privacy. Study reports will combine your answers with those from others to summarize what we found. We will never report names or addresses. This way, no one can identify you, your child, or your child care provider.
IF: It's a bad time.
ANSWER: We can schedule a callback for a
time that would be good for you.
Date _____________ Time
_____________________
IF STILL HESITANT: [SAMPLED SITE NAME] is one of about 1,300 child care providers across the country that are helping USDA understand the food and activities provided in child care settings. We want to be sure that the study includes people like yourself, to ensure that the study findings are fair and accurate. We really want to include your household in the study. If now is a bad time, we can schedule the interview during the day or in the evening, any time that is better for you.
IF RESPONDENT AGREES TO PARTICIPATE, RESUME INTERVIEW
IF STILL REFUSES, THANK AND COMPLETE
Authority: This information is being collected under the authority of the Healthy, Hunger-Free Kids Act of 2010 (P. L. 111-296), Section 305.
Purpose: The Food and Nutrition Service (FNS) is collecting this information to evaluate the nutritional quality of Child and Adult Care Food Program (CACFP) meals and snacks, the cost to produce them, and dietary intakes and activity levels of CACFP participants.
Routine Use: The records in this system may be disclosed to private firms that have contracted with FNS to collect, aggregate, analyze, or otherwise refine records for the purpose of research and reporting to Congress and appropriate oversight agencies, and/or departmental and FNS officials.
Disclosure: Disclosing the information is voluntary, and there are no consequences to you as an individual participant in the CACFP for not providing the information.
The System of Records Notice for this information collection is USDA/FNS-8, FNS Studies and Reports, which can be located at https://www.govinfo.gov/content/pkg/FR-1991-04-25/pdf/FR-1991-04-25.pdf (p. 19078).
1 These are programming notes. On screen, this will take the interviewer to the correct screen.
2 Adamo KB, et al. Using path analysis to understand parent’s perceptions of their children’s weight, physical activity, and eating habits in the Champlain region of Ontario. Paediatrics & Child Health (2010);15(9):e33-e41. https://doi.org/10.1093/pch/15.9.e33
3 Question stem revised from Physical Activity Assessment Tool https://www.aafp.org/afp/2008/0415/afp20080415p1129-f1.pdf
4 Question stem revised from Physical Activity Assessment Tool https://www.aafp.org/afp/2008/0415/afp20080415p1129-f1.pdf and response categories from NHANES, NNYFS PAQ.710
5 Question wording from ISCOLE Diet and Lifestyle Questionnaire, Q2.
6 Question stem revised from Physical Activity Assessment Tool https://www.aafp.org/afp/2008/0415/afp20080415p1129-f1.pdf and response categories from NHANES, NNYFS PAQ.731
7 Time spent sitting and getting to and from places modeled after NHANES PAQ.680: https://wwwn.cdc.gov/nchs/data/nhanes/2019-2020/questionnaires/PAQ_K.pdf
8 Time spent sitting doing homework, reading, playing cards or board games modeled after: NHANES PAQ.680: https://wwwn.cdc.gov/nchs/data/nhanes/2019-2020/questionnaires/PAQ_K.pdf and response categories modeled after NHANES NYFS, PAQ.710: https://www.cdc.gov/nchs/data/nnyfs/PAQ.pdf
9 Introduction modeled after: NHANES PAQ.655: https://wwwn.cdc.gov/nchs/data/nhanes/2019-2020/questionnaires/PAQ_K.pdf
10 Question stem modeled after: Physical Activity Assessment Tool: https://www.aafp.org/afp/2008/0415/afp20080415p1129-f1.pdf
11 Time spent doing these activities modeled after: Physical Activity Assessment Tool: https://www.aafp.org/afp/2008/0415/afp20080415p1129-f1.pdf and response models modeled after NHANES NYFS, PAQ.710: https://www.cdc.gov/nchs/data/nnyfs/PAQ.pdf
12 Response options for time spent modeled after NHANES NYFS, PAQ.710: https://www.cdc.gov/nchs/data/nnyfs/PAQ.pdf
13 We will determine any State-specific names and make them available to the interviewer in a pop-up window during the interview.
14 We will determine any State-specific names and make them available to the interviewer in a pop-up window during the interview.
| File Type | application/vnd.openxmlformats-officedocument.wordprocessingml.document |
| File Title | Abt Single-Sided Body Template |
| Author | Patty Connor |
| File Modified | 0000-00-00 |
| File Created | 2022-05-03 |
© 2026 OMB.report | Privacy Policy