10-10147 VHA OSI Primary Care Survey
Generic Clearance for the Collection of Qualitative Feedback on Agency Service Delivery (NCA, VBA, VHA)
VHA_OSI Conjoint_Primary Care_Survey_11-21-14 Final
Health Research Multilevel Engagement, SORCC Patient Survey,
OMB: 2900-0770
OMB No. 2900-0770
Estimated Burden: 7 Minutes
Expiration Date: XX/XX/XXXX

Voice of the Veteran Satisfaction Survey
OSI Conjoint Analysis
The Paperwork Reduction Act of 1995: This information is collected in accordance with section 3507 of the Paperwork Reduction Act of 1995. Accordingly, we may not conduct or sponsor and you are not required to respond to, a collection of information unless it displays a valid OMB number. We anticipate that the time expended by all individuals who complete this survey will average 7 minutes. This includes the time it will take to follow instructions, gather the necessary facts and respond to questions asked. Customer satisfaction is used to gauge customer perceptions of VA services as well as customer expectations and desires. The results of this telephone/mail survey will lead to improvements in the quality of service delivery by helping to achieve improved mental health services. Participation in this survey is voluntary and failure to respond will have no impact on benefits to which you may currently be receiving.
Veterans Health Adminsitration
J.D. Power and Associates
OSI Conjoint Survey – Primary Care
Draft 1
Section Name |
Section Title |
Level |
Order Group |
Order |
Introduction |
Introduction |
1 |
|
|
Choice Tasks |
Access to VHA Primary Care |
1 |
|
|
Follow-up Questions |
Misc Diagnostics |
1 |
|
|
Demographics |
Demographics |
1 |
|
|
INTRODUCTION
Welcome. J.D. Power and Associates has been asked by the Department of Veterans Affairs to conduct a study to better understand Veterans’ attitudes and opinions about Veterans’ access to Primary Care at VA facilities. This study is not regarding any care you may have received, or any care you might receive in the future, but your preferences, as a Veteran, with regards to Primary Care.
Your responses will be completely anonomyous and will not affect any benefits or services you may be receiving from the VA.
This survey will take approximately 10-12 minutes to complete. We thank you in advance for your participation.
Click here for our privacy and cookie notice.
S1 Are you currently a Veteran?
1 Yes
0 No [TERMINATE]
99 Don’t know [TERMINATE]
S2. Do you currently receive health care from the Department of Veterans Affairs?
Yes—my primary care provider is through the VA
Yes—but my primary care provider is not through the VA
0 No
S3. Do you currently receive health care from a provider other than the Department of Veterans Affairs?
Yes
0 No
-
[PROG: IF S2 = 0 and S3 = 0 then TERMINATE; ELSE IF S2 = 1 OR 2 THEN FILL VA HEALTHCARE QUOTA; IF S2 = 0 AND S3 = 1 THEN FILL NON-VA HEALTHCARE QUOTA]
S4. Are you currently being treated for a chronic condition with the Department of Veterans Affairs or another provider (e.g., diabetes, hypertension)?
Yes
0 No
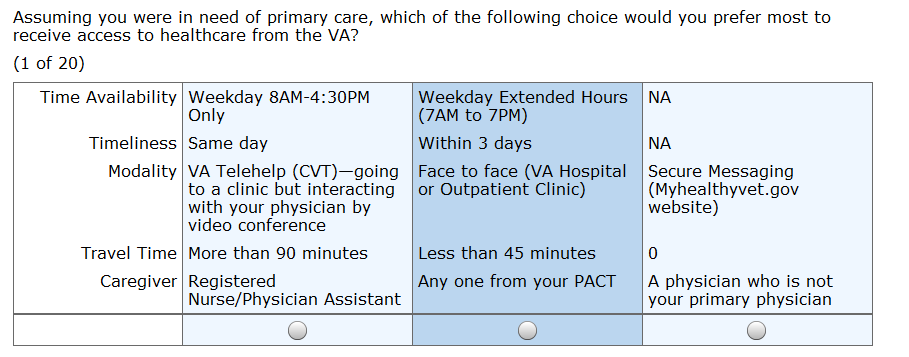
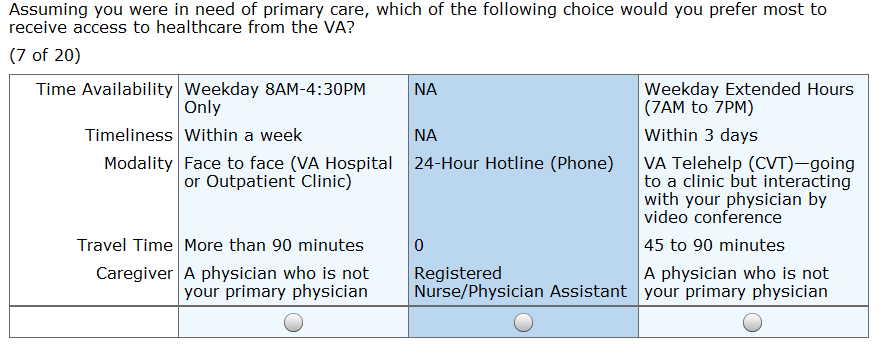
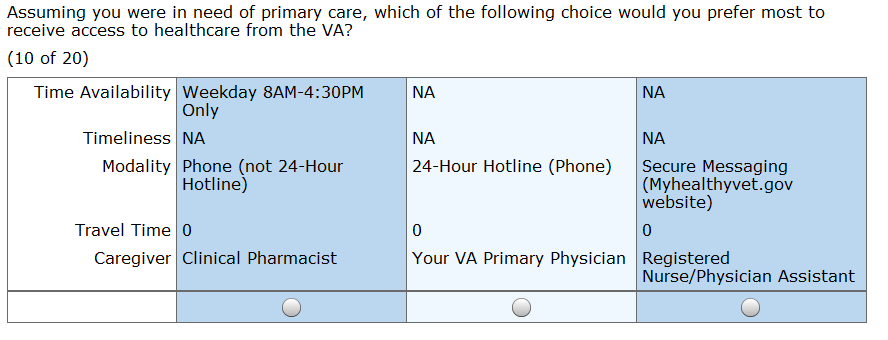
CHOICE TASKS
Thank you for your responses so far. We’d now like you to go through an exercise that will better help us understand your opinions about how you prefer to access VA healthcare for primary care.
In the following exercise, you will presented choices with different features that fall into 5 different categories as specified below. Your task is to select the choice you would prefer the most regarding how you would access VA healthcare. When making your selection, you can assume everything is the same except the differences shown for each choice. You will be asked to make selection for a total of 20 screens. Each screen may look very similar. However the choices are different so please be careful in making your selection.
Focus only on primary care which includes physicals/preventative care, illness or injury, follow-up visits or information with your primary care provider (not any type of Speciality Care).
Time Availability: The times you can access healthcare
Weekday 8AM-4:30PM Only
Weekday Extended Hours (7AM to 7PM)
Weekday Extended Hours (7AM to 7PM) and Weekend (8AM-4:30PM)
Timeliness: How long it takes to get an appointment from the time you first request to be seen
Same day
Within 3 days
Within a week
Within a month
[PROG NOTE: THIS FACTOR IS ONLY SHOWN WITH FACE TO FACE AND TELEHELP MODALITY BELOW]
Travel Time: The amount of transit time from your home to healthcare provider’s facility
Less than 45 minutes
45 to 90 minutes
More than 90 minutes
Modality: How you interact with the care provider
Face to face (VA Hospital or Outpatient Clinic)
Phone (not 24-Hour Hotline)
Secure Messaging (Myhealthyvet.gov website)
VA Telehelp (CVT)—going to a VA facility, but interacting with your physician by video conference
24-Hour Hotline (Phone)
Caregiver: The person providing the healthcare
Your VA Primary Physician
Registered Nurse/Physician Assistant
Clinical Pharmacist
Any one from your PACT
A physician who is not your primary physician
Note: PACT is your Patient Aligned Care Team and it includes your primary care physician, registered nurse, health technician, clerk and pharmacist
[PROG NOTE: SHOW 20 SCREENS (EXAMPLE BELOW), RANDOMLY MANIPULATING THE FEATURE SET WITHIN THE THREE CHOICES FOR EACH SCREEN]
FOLLOW-UP
F1. Which of the following methods would you prefer most to be reminded about an appointment you have with the VA?[PROG: SINGLE RESPONSE, FORCED]
Letter in the mail
Postcard in the mail
Text/SMS message
Phone call
Secure Messaging (Myhealthevet.gov website)
0 No preference
F2. If the VA had to cancel an appointment, which of the following methods would you prefer most to be notified?[PROG: SINGLE RESPONSE, FORCED]
Letter in the mail
Postcard in the mail
Text/SMS message
Phone call
Secure Messaging (Myhealthevet.gov website)
0 No preference
F3. Would you participate in a group appointment if one was offered? Group appointments are typically check-ups for veterans with the same condition. Private interaction with your primary care provider can be part of the appointment as well as group education and interaction.
Yes
No
2 Maybe
F4. While not currently offered by the VA, would you be willing to use an unsecured communication method (e.g. Skype, Facetime) to interact with your primary care provider or PACT Team member?
Yes
0 No
2 Maybe
DEMOGRAPHICS
These last few questions are for classification purposes only.
D1. In what year were you born?
Year of birth [PROG: DROPDOWN, FORCED, RANGE = 1914- 1996]
9998 Prefer not to answer [PROG: EXCLUSIVE]
D2. Are you…? [PROG: SINGLE RESPONSE, FORCED]
Male
0 Female
98 Prefer not to answer
D3. What was the last year of school you completed? [PROG: SINGLE RESPONSE, FORCED]
1 8th grade or less
2 Some high school
3 High school graduate
5 Some college
6 4-year college degree
9 More than 4 year degree
98 Prefer not to answer
D4. Is the area in which you live a/an…?
[PROG: SINGLE RESPONSE, FORCED]
1 Rural area
2 Suburban area
3 Urban area
99 Don't know
D5 Which of the following best describes your health status? [PROG: SINGLE RESPONSE, FORCED]
Excellent
Very Good
Good
Fair
Poor
98 Prefer not to answer
EXIT. That concludes our survey. J.D. Power thanks you for participating.
© 2014 J.D. Power and
Associates, McGraw-Hill Financial. All Rights Reserved. Page
| File Type | application/msword |
| Author | evej |
| Last Modified By | Manuel, Howard L. |
| File Modified | 2014-12-19 |
| File Created | 2014-12-19 |
© 2026 OMB.report | Privacy Policy