NOAA - "Let Spinners Sleep" Educational Products and Services Survey
Generic Clearance for the Collection of Qualitative Feedback on Agency Service Delivery
Let Spinners Sleep Teacher Survey.060414
NOAA - "Let Spinners Sleep" Educational Products and Services Survey
OMB: 0690-0030
Responsible Dolphin Viewing
Products and Services Evaluation
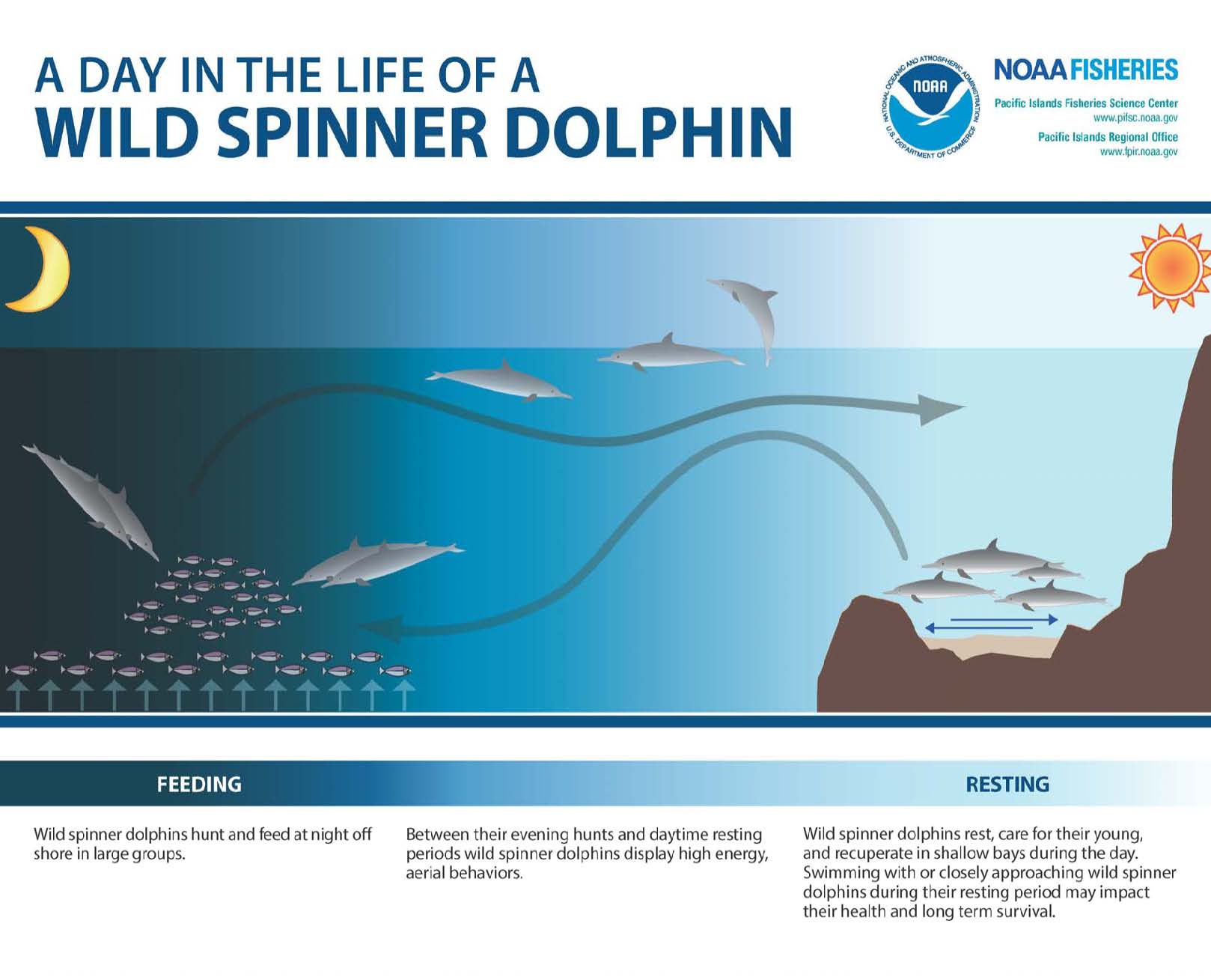
Figure 1. Day in the Life of a Spinner Dolphin graphic
Your participation in this survey is voluntary and responses are anonymous and confidential. Any material that might identify you will be destroyed at the end of the study. OMB Control No. 0690-0030
Expiration Date: 06/30/2017
This survey is being conducted to gather information about the “Let Spinners Sleep” Spinner Dolphin Presentations and Student Activity Guide. The results of the survey will help NOAA Fisheries and its partners evaluate the success of the program and how they may improve on this program for the future. The survey also offers an opportunity for you to provide suggestions for other spinner dolphin educational programming you would like to see developed. Thank you for your participation. Your feedback is valuable.
Estimated response time is 10 minutes. Send comments regarding this burden estimate or any other suggestions for reducing this burden to Laura McCue, NOAA National Marine Fisheries Service, IRC, 1845 Wasp Blvd, Bldg 176, Honolulu, HI 96818
Notwithstanding any other provisions of the law, no person is required to respond to, nor shall any person be subjected to a penalty for failure to comply with, a collection of information subject to the requirements of the Paperwork Reduction Act, unless that collection of information displays a currently valid OMB Control Number.
When you have completed the survey, please return it in the addressed postage paid envelope provided. Thank you!
Did your class receive a presentation about Spinner Dolphins and participate in a follow up student activity?
____Yes ____No
If yes, was the presentation effective in increasing your awareness about spinner dolphins and responsible viewing practices? ____Yes ____No
Which
activity did your students participate in? (CHECK ONE)
___ Spinner Shake Out ___Get the Message ___Mock Advisory Committee Meeting
Did you receive the “Let Spinners Sleep” Spinner Dolphin Student Activity Guide and materials?
____Yes ____No
If yes, how often have you
used the Activity Guide and materials in the last 6 months? (CHECK
ONE)
___ Once___ Twice ___ More than
twice Have not used it
Do you plan to use them in the
future?
____Yes ____No
One goal of the “Let Spinners Sleep” program was for teachers to share their knowledge and materials with other teachers at their respective schools who were unable to attend the presentation. If you attended a presentation and received a the “Let Spinners Sleep” Spinner Dolphin Student Activity Guide and materials, how many teachers have you been able to share them with?__________________________________________________________________
Do you plan to share the materials with teachers in the future?
____Yes ____No
What other school-based spinner dolphin education products / services would you like to see produced? ______________________________________________________________________________________________
What media or format would you like to see these products / services offered in? (CHECK ALL THAT APPLY)
-
Hand-outs/workbook
Citizen Science
Podcasts
Videos
Web-based activities
Other ________________
School field trips
Visiting scientist presentations
Would you be interested in receiving spinner dolphin related lesson plans and activities as they become available? (supplies will be dependent on availability)? ____Yes ____No
If yes, please provide a
mailing address where they can be sent (your name and address will
remain confidential)
Name or Organization:
_________________________________________
Street Address: _______________________________________________
______________________________
Zip Code: ________
Please return this survey in the addressed postage paid envelope provided – Thank you!
| File Type | application/msword |
| File Title | “Fishing Around Sea Turtles” Six-month Evaluation |
| Author | jennifer.metz |
| File Modified | 2014-06-04 |
| File Created | 2014-06-04 |
© 2026 OMB.report | Privacy Policy