National Clandestine Laboratory Seizure Report
National Clandestine Laboratory Seizure Report
EPIC 143 CLS Automated Form Guide
National Clandestine Laboratory Seizure Report
OMB: 1117-0042
Automated CLS Form EPIC 143
EPIC 143
National Clandestine
Laboratory Seizure Report
Automated Form
I. Introduction
The National Clandestine Laboratory Seizure (CLS) Form EPIC 143 that EPIC has been using is now available in an automated FDF format. The form is a FDF and can be submitted electronically via e-mail to EPIC. The form can then be printed or saved as a PDF for use locally or by state agencies.
II. Purpose
The purpose of this document is to explain the use of the Form EPIC 143, how to fill it out, and then how to send the seizure information to EPIC.
III. The Form EPIC 143 Clan Lab Automated Edition
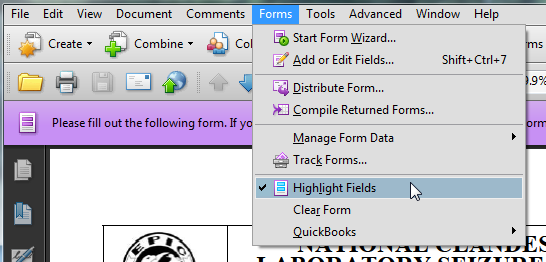
Fields marked by a red box around them are the required fields on the Form EPIC 143. To turn on the highlighted fields to see what is required go to the forms menu in adobe and select Highlight Fields.
When you select a box in a “check one” section, the unselected choices will stay highlighted as a reminder that the field is mandatory. For instance, the TYPE OF REPORT section has Lab Seizure checked and the other 2 choices still have the red box indicating a required field in that section. In Section II, the Seizure Location section, the Family Dwelling is checked and all the other fields still have the red outline.
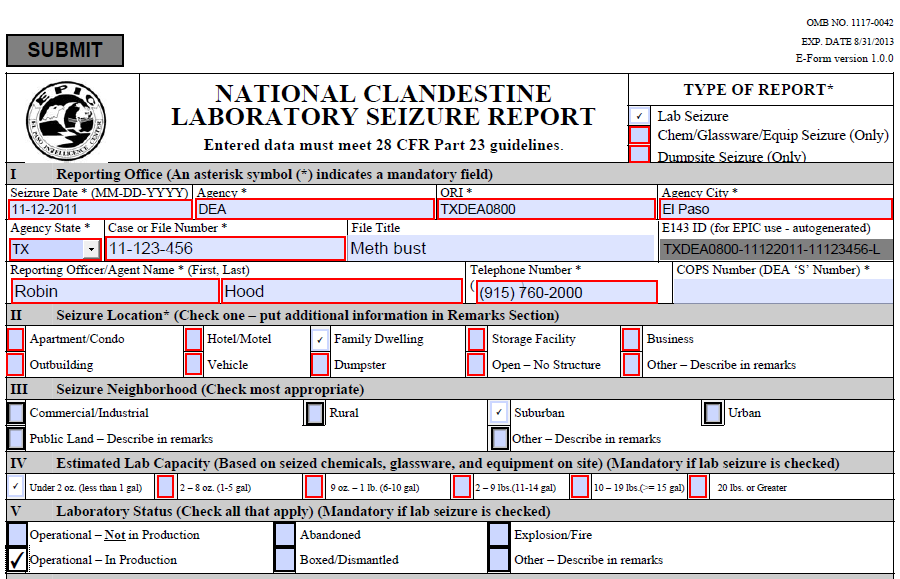
Section I Reporting Office
Seizure Date (required) is the actual date of the seizure, not the date of reporting the seizure.
Agency (required) is the full agency name of the office reporting the seizure.
ORI (required) is the Originating Reporting Identifier. This 9 digit identifier starts with a 2 character state identifier, followed by a 2 or 3 character type designation (SP- State Police, DEA- Drug Enforcement Administration); the rest of the code is numbers to designate the exact location of the agency.
Agency City (required) location of the reporting agency. Also to be entered as city for the seizing agency in the NSS.
Agency State (required) location of the reporting agency. Also to be entered as state for the seizing agency in the NSS.
Case or File Number (required) the case or file number of the incident.
File Title (not required) used for case or file title is applicable.
Unique ID (system generated) is a combination of the ORI, the seizure date, and the case number. This number is used to track individual submissions of the form; in the event of issues arising with a submission, this number can be used to determine the submission that had issues.
Reporting Officer/Agent Name, First & Last (required) First then Last name of person reporting the incident.
Telephone Number (required) call back number for the person reporting the incident.
COPS Number (not required) DEA generated number when using DEA for clean-up of incident. The format of this is XX-YY-SZZZ where XX is the state code, YY is 2 numbers, and ZZZ is 3 numbers.
Section II Seizure Location
Select one (required) from the list of incident locations. If Other is selected, be sure to describe the location in the remarks section.
Section III Seizure Neighborhood
Select one (not required) from the list of neighborhoods that best describes the incident area.
Section IV Estimated Lab Capacity
Select one (required if Lab Seizure is the type of report) from the list that best describes the quantity of drugs that can be manufactured in a single batch with the equipment and chemicals at the incident location.
Section V Laboratory Status
Select all that apply (required if Lab Seizure is the type of report) from the list that describe the status of the lab when it was discovered during the incident. If Other is selected then the description must be entered in the remarks section.
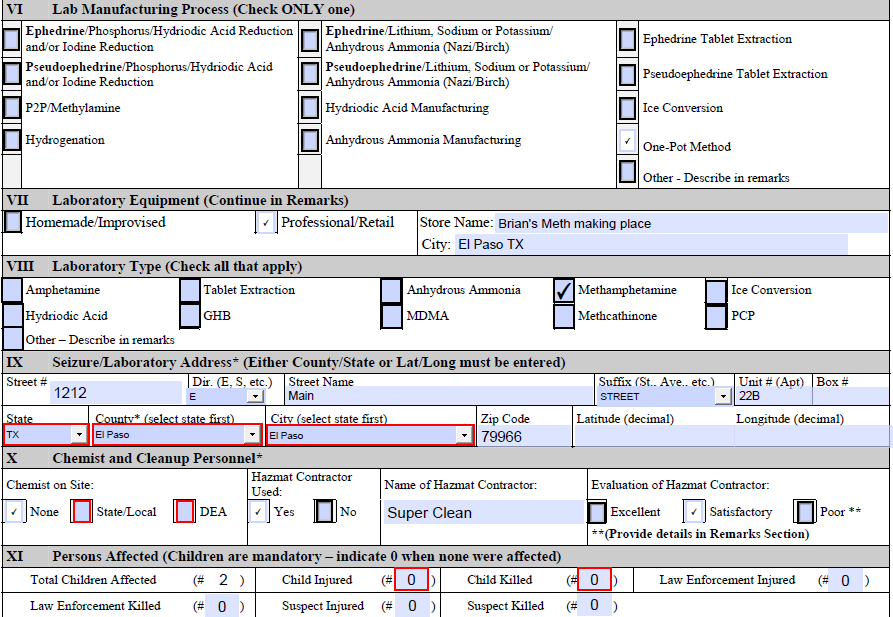
Section VI Lab Manufacturing Process
Select only one (not required) of the listed processes of manufacturing contraband. If Other is selected, then the description must be entered in the remarks section.
Section VII Laboratory Equipment
Select one (not required) Homemade or Professional. Include the store name for professional. Use the remarks section if more information is available.
Section VIII Laboratory Type
Select all that apply (not required) of the laboratory types listed. If Other is selected then the description must be entered in the remarks section.
Section IX Seizure/Laboratory Address
Either state, county and city OR the lat/long is required for the incident. The full address can be entered for the incident, but must include the state, county and city. If the Lat/Long is used it must be entered in decimal format and the rest of the address in unnecessary.
Section X Chemist and Cleanup Personnel
Chemist on Site (required) select one. Hazmat Contractor used (not required) select one. Name of Hazmat Contractor (fill in if used) and Evaluation of Hazmat Contractor. If the Evaluation is poor then provide details in the remarks section.
Section XI Persons Affected
Children are required. All entries in this section default to 0. Change the quantities as needed and describe how people were injured or killed. Enter a description of how people were injured or killed in the remarks section at the end of the form.
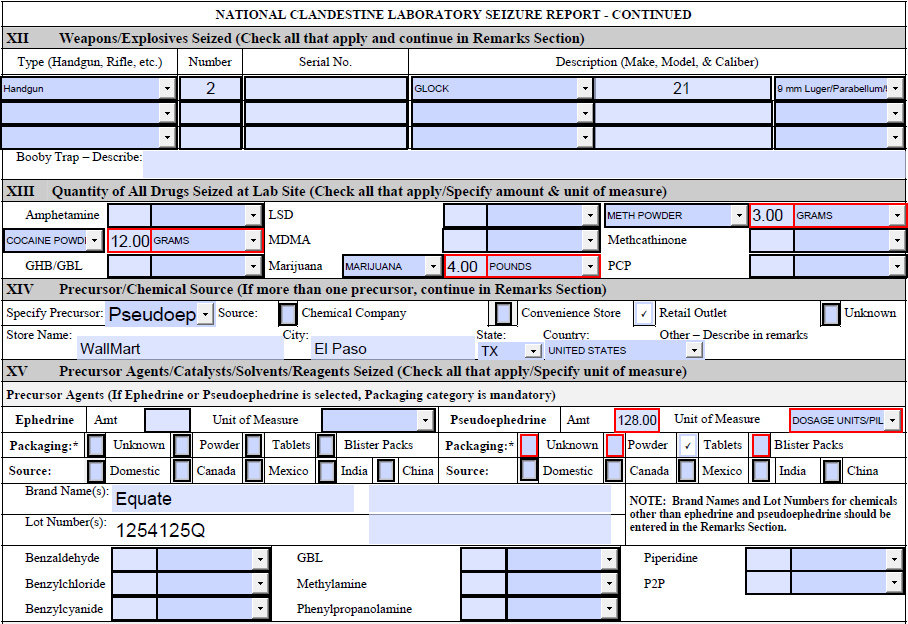
Section XII Weapons/Explosives Seized
Section not required. Enter the Type, Number of weapons, the Serial Number, Make, Model and Caliber of the weapon. At the bottom of the section, a description of any booby traps can be entered.
Section XIII Quantity of All Drugs Seized at Lab Site
Section not required. Enter all the drugs found at the seized location. Enter the quantity and the unit of measure for each drug found at the site.
Section XIV Precursor/Chemical Source
Section not required. If entering precursor source data use the Specify precursor drop-down menu.
Section XV Agents/Catalysts/Solvents/Reagents Seized
Agents
If Ephedrine or Pseudoephedrine is selected, then the packaging is required. Enter the amount and the unit of measure, the packaging (required) and the source. Enter the brand name and lot number from the Ephedrine and Pseudoephedrine. Enter the quantity and unit of measure for all other agents.
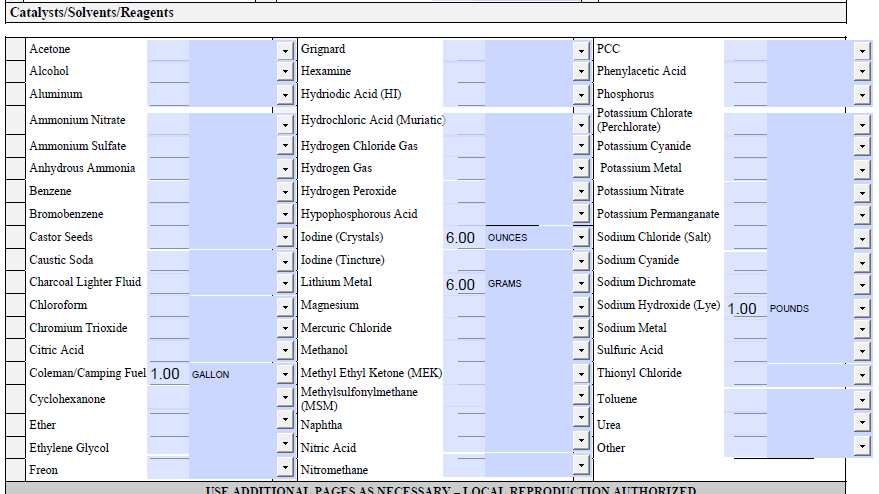
Catalysts/Solvents/Reagents
Enter the quantity and the unit of measure for all of the other chemicals found at the incident location. Batteries are not each, they should be listed as 1 gram per battery found at incident location. If Other is used, then enter details in the remarks section.
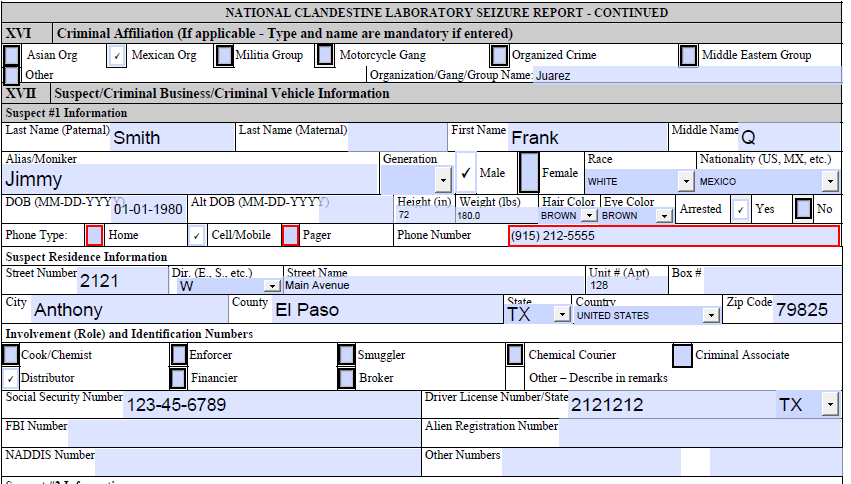
Section XVI Criminal Affiliation
Select one (not required) of the affiliations listed and then enter the name of the affiliation. If Other is used then enter details in the remarks section.
Section XVII Suspect/Criminal Business/Criminal Vehicle Information
Suspect 1 Information
Enter the name information including the alias, then the sex, race and nationality of the subject.
Enter the DOB and identifiers for the subject. Per the EPIC Director, EPIC policy is not to collect and store data on juveniles. If Juvenile DOB is entered the Form will be rejected when Submitted.
If a phone number is entered, the phone type is required.
Suspect Residence Information is next, followed by the involvement of the subject. Check all that apply for the involvement.
Enter all the Identification numbers that can be found for the subject.
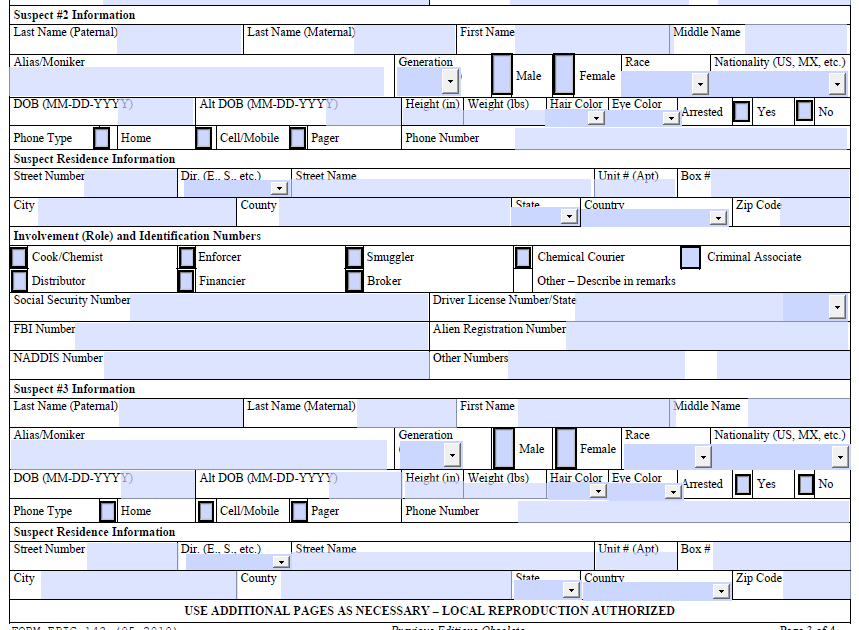
Repeat Suspect information for each of the subjects involved in the incident. Three subjects can be entered into the form. If more subjects are involved then enter the information in the remarks section.
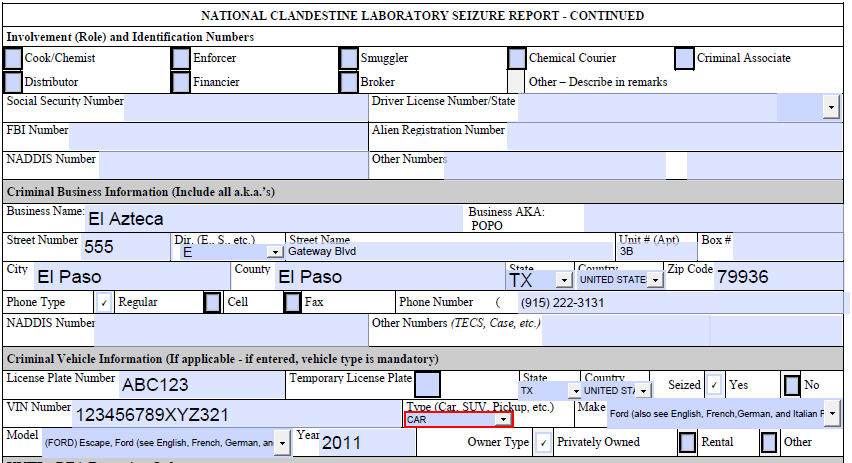
2) Criminal Business Information
Enter the name, AKA, full address and phone number of the business. Include the NADDIS number and the TECS number if available.
3) Criminal Vehicle Information
Enter the license plate, state, country, VIN, Type (required), Make, Model and Year of the vehicle involved in the incident.
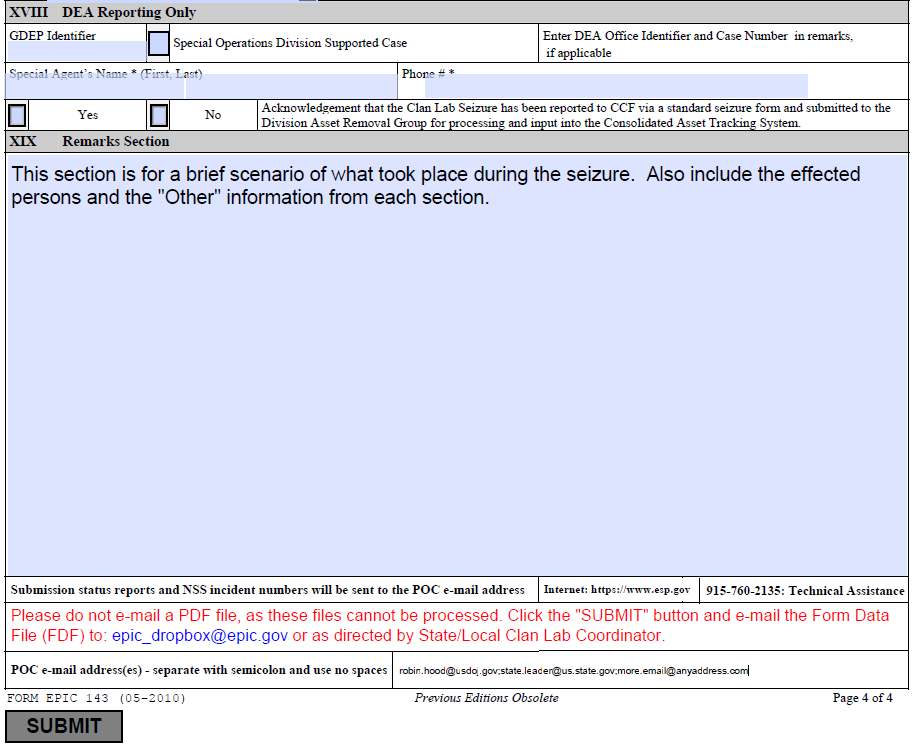
Section XVIII DEA Reporting Only
This section is used by DEA only.
Section XIX Remarks Section
This section is used to write up the general information on the incident. It should include what happened leading up to the incident and the outcome of the incident. Also included in the remarks section the description of how people were injured or killed plus any of the sections where Other was used as a choice should be detailed here.
When the remarks are finished enter the E-mail address of the POC for the report. The POC should be the state agency coordinator, or your area’s designee, to verify the submission of the report. The submission status report will be sent to this address. The submission status report will detail the NSS incident number if successful or the error codes if the report is unsuccessful. A unsuccessful report can be fixed and then resubmitted.
IV. Submitting the form
It is recommended that you save a copy of the form as a PDF before submitting in case you need to refer to the form later. Once all required fields have been filled out, click the “Submit” button; this will prompt you to either use your mail client or Internet mail to submit the form. Please note that the submit button creates an FDF file that contains all the data from the form; this FDF file is what must be mailed to epic_dropbox@epic.gov. EPIC cannot and will not process PDF files.
V. Support
If users have any questions completing the National Clandestine Laboratory Seizure (CLS) Form EPIC 143 please contact the Clan Lab Collections Team at 1-888-873-3742 option 2. If users experience any technical difficulties, account problems, or have suggested improvements, contact the EPIC Help Desk at 1-915-760-2135 or email at the address Helpdesk@esp.gov .
| File Type | application/msword |
| Author | res00737 |
| Last Modified By | res01201 |
| File Modified | 2012-03-30 |
| File Created | 2012-03-30 |
© 2026 OMB.report | Privacy Policy