Impact Evaluation Instruments
Models of SNAP-Education (ED)and Evaluation Study
APPENDIX A. Data Collection Instruments for Impact Evaluation-SNAP-Ed I-English_Spanish
Impact Evaluation Instruments
OMB: 0584-0554
Appendix
A.
Data Collection Instruments
for Impact Evaluation
Impact Evaluation Instrument for CNNS
For the CNNS project, we will survey parents/caregivers of first through third grade students at pre- and post-intervention using a mail/telephone survey approach. We provide the following four versions of the instrument:
mail questionnaire (pre-survey - intervention and control groups),
mail questionnaire (post-survey - intervention group),
mail questionnaire (post-survey - control group), and
telephone questionnaire for nonrespondents to mail survey (pre- and post-surveys - intervention and control groups).
OMB No. 0584-NEW
Expiration date: XX/XXXX
See OMB statement on inside cover
What Does Your Child Eat?
|
|
Thank you for taking part in this important study!
Please fill out and return the survey in the enclosed envelope within the next week.
If you have any questions about the What Does Your Child Eat? study, please send an e-mail to xxxx@rti.org or call toll-free at 1-800-xxx-xxxx.
Public reporting burden for this collection of information is estimated to average 15 minutes per response, including the time for reviewing instructions, searching existing data sources, gathering and maintaining the data needed, and completing and reviewing the collection of information.
An agency may not conduct or sponsor, and a person is not required to respond to, a collection of information unless it displays a currently valid OMB control number.
Send comments regarding this burden estimate or any other aspect of this collection of information, including suggestions for reducing this burden, to: U.S. Department of Agriculture, Food and Nutrition Services, Office of Research and Analysis, Room 1014, Alexandria, VA 22302 ATTN: PRA (0584-xxxx*). Do not return the completed form to this address.
If you have questions regarding your rights as a research participant, you may contact RTI’s Office of Research Protection toll-free at 866-214-2043.
What
Does Your Child Eat?
Mail Questionnaire (Pre-survey,
Intervention and Control Groups)
Instrument for CNNS Impact Evaluation
This survey asks about what your child eats. This study is being sponsored by the U.S. Department of Agriculture’s Food & Nutrition Service and conducted by RTI International, a non-profit research organization. The survey will take about 15 to 20 minutes to complete. You will receive $10 for completing this survey and $15 for completing a second survey that we will mail you in about 2 months.
All of your answers to the survey will be kept private. We will not share your answers with anyone. You may skip any questions you do not want to answer. If you have any questions, please call XXX XXXX at RTI International at 1-800-xxx-xxxx.
Questions on Whether Certain Foods Are Available at Home
Were any of the following foods available in your home during the past week? Include fresh, frozen, canned, and dried foods. (Circle yes or no for each food.)
|
Yes |
No |
|
Yes |
No |
|
Yes |
No |
|
Yes |
No |
|
Yes |
No |
|
Yes |
No |
|
Yes |
No |
|
Yes |
No |
|
Yes |
No |
|
Yes |
No |
|
Yes |
No |
Questions on the Fruits and Vegetables Your Child Eats
For the next questions think about what your child ate during the past week, or the past 7 days. Do not include school or day care time.
How many days during the past week did your child eat more than one kind of fruit each day? Do not include fruit juice. (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
During the past week, how many cups of fruit did your child eat each day? Do not include fruit juice. (Circle one.)
1. None
2. 1/2 cup
3. 1 cup
4. 1 ½ cups
5. 2 cups
None
1 cup
2 cups
3 cups
6. 2 ½ cups
7. 3 cups or more
How many days during the past week did your child eat more than one kind of vegetable each day? Do not include vegetable juice. (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
During the past week, how many cups of vegetables did your child eat each day? Do not include vegetable juice. (Circle one.)
1. None

2. 1/2 cup
3. 1 cup
4. 1 ½ cups
5. 2 cups
None
1 cup
2 cups
3 cups
6. 2 ½ cups
7. 3 cups or more
During the past week, did your child eat any meals or snacks that were provided by his or her school or day care? (Circle all that apply.)
1. Yes, breakfast
2. Yes, lunch
3. Yes, snacks
4. No, did not eat breakfast, lunch, or snacks provided by school or day care
Is your child willing to try a new kind of fruit? (Circle one.)
1. No
2. Maybe
3. Yes
How many days during the past week did you give your child fruit as a snack? (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
How many days during the past week did your child ask or help himself or herself to fruit for a snack? (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
How many days during the past week did you give your child fruit at dinner? (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
Is your child willing to try a new kind of vegetable? (Circle one.)
1. No
2. Maybe
3. Yes
How many days during the past week did you give your child a vegetable as a snack? (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
How many days during the past week did your child ask or help himself or herself to vegetables for a snack? (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
How many days during the past week did you give your child a vegetable at dinner? (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
Questions on Your Child’s Eating Habits
How many days during the past week did your child help you make a snack or cook a meal? For example, did your child wash fruits or vegetables or crack an egg? (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
How much do you agree or disagree with the following statement? “If my child eats healthy, he or she will be healthier when he or she gets older.” (Circle one.)
1. Strongly agree
2. Agree
3. Disagree
4. Strongly disagree
How much do you agree or disagree with the following statement? “I am a good role model for my child by eating healthy foods.” (Circle one.)
1. Strongly agree
2. Agree
3. Disagree
4. Strongly disagree
How strongly do you agree or disagree with the following statement? “I can help my child eat a diet that is healthy.” (Circle one.)
1. Strongly agree
2. Agree
3. Disagree
4. Strongly disagree
Questions about You and Your Household
During the past year, how often did you run out of food before the end of the month? (Circle one.)
1. Did not run out of food
2. Seldom
3. Sometimes
4. Most of the time
5. Almost always
How many people under 18 years of age live in your household?
____
Including yourself, how many people 18 years of age or older live in your household?
____
Which of the following categories best describes your age? (Circle one.)
1. 18 to 24
2. 25 to 34
3. 35 to 44
4. 45 to 54
5. 55 to 64
6. 65 to 74
7. Over 74
What is your gender? (Circle one.)
1. Male
2. Female
Are you Hispanic or Latino? (Circle one.)
1. Yes
2. No
What is your race? (Circle all that apply.)
1. American Indian or Alaska Native
2. Asian
3. Black or African American
4. Native Hawaiian or other Pacific Islander
5. White
Thank
you for completing our survey.
Please return the survey in the
enclosed envelope.
OMB No. 0584-NEW
Expiration date: XX/XXXX
See OMB statement on inside cover
What Does Your Child Eat?
|
|
Thank you for taking part in this important study!
Please fill out and return the survey in the enclosed envelope within the next week.
If you have any questions about the What Does Your Child Eat? study, please send an e-mail to xxxx@rti.org or call toll-free at 1-800-xxx-xxxx.
Public reporting burden for this collection of information is estimated to average 15 minutes per response, including the time for reviewing instructions, searching existing data sources, gathering and maintaining the data needed, and completing and reviewing the collection of information.
An agency may not conduct or sponsor, and a person is not required to respond to, a collection of information unless it displays a currently valid OMB control number.
Send comments regarding this burden estimate or any other aspect of this collection of information, including suggestions for reducing this burden, to: U.S. Department of Agriculture, Food and Nutrition Services, Office of Research and Analysis, Room 1014, Alexandria, VA 22302 ATTN: PRA (0584-xxxx*). Do not return the completed form to this address.
If you have questions regarding your rights as a research participant, you may contact RTI’s Office of Research Protection toll-free at 866-214-2043.
What
Does Your Child Eat?
Mail Questionnaire (Post-survey,
Intervention Group)
Instrument for CNNS Impact Evaluation
This survey asks about what your child eats. This study is being sponsored by the U.S. Department of Agriculture’s Food & Nutrition Service and conducted by RTI International, a non-profit research organization. The survey will take about 15 to 20 minutes to complete. You will receive $15 for completing this survey.
All of your answers to the survey will be kept private. We will not share your answers with anyone. You may skip any questions you do not want to answer. If you have any questions, please call XXX XXXX at RTI International at 1-800-xxx-xxxx.
Questions on Whether Certain Foods Are Available at Home
Were any of the following foods available in your home during the past week? Include fresh, frozen, canned, and dried foods. (Circle yes or no for each food.)
|
Yes |
No |
|
Yes |
No |
|
Yes |
No |
|
Yes |
No |
|
Yes |
No |
|
Yes |
No |
|
Yes |
No |
|
Yes |
No |
|
Yes |
No |
|
Yes |
No |
|
Yes |
No |
Questions on the Fruits and Vegetables Your Child Eats
For the next questions think about what your child ate during the past week, or the past 7 days. Do not include school or day care time.
How many days during the past week did your child eat more than one kind of fruit each day? Do not include fruit juice. (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
During the past week, how many cups of fruit did your child eat each day? Do not include fruit juice. (Circle one.)
1. None
2. 1/2 cup
3. 1 cup
4. 1 ½ cups
5. 2 cups
None
1 cup
2 cups
3 cups
6. 2 ½ cups
7. 3 cups or more
During the past week, did your child eat more than one kind of vegetable each day? Do not include vegetable juice. (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
During the past week, how many cups of vegetables did your child eat each day? Do not include vegetable juice. (Circle one.)
1. None
2. 1/2 cup
3. 1 cup
4. 1 ½ cups
5. 2 cups
None
1 cup
2 cups
3 cups
6. 2 ½ cups
7. 3 cups or more
During the past week, did your child eat any meals or snacks that were provided by his or her school or day care? (Circle all that apply.)
1. Yes, breakfast
2. Yes, lunch
3. Yes, snacks
4. No, did not eat breakfast, lunch, or snacks provided by school or day care
Is your child willing to try a new kind of fruit? (Circle one.)
1. No
2. Maybe
3. Yes
How many days during the past week did you give your child fruit as a snack? (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
How many days during the past week did your child ask or help himself or herself to fruit for a snack? (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
How many days during the past week did you give your child fruit at dinner? (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
Is your child willing to try a new kind of vegetable? (Circle one.)
1. No
2. Maybe
3. Yes
How many days during the past week did you give your child a vegetable as a snack? (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
How many days during the past week did your child ask or help himself or herself to vegetables for a snack? (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
How many days during the past week did you give your child a vegetable at dinner? (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
Questions on Your Child’s Eating Habits
How many days during the past week did your child help you make a snack or cook a meal? For example, did your child wash fruits or vegetables or crack an egg? (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
How much do you agree or disagree with the following statement? “If my child eats healthy, he or she will be healthier when he or she gets older.” (Circle one.)
1. Strongly agree
2. Agree
3. Disagree
4. Strongly disagree
How much do you agree or disagree with the following statement? “I am a good role model for my child by eating healthy foods.” (Circle one.)
1. Strongly agree
2. Agree
3. Disagree
4. Strongly disagree
How strongly do you agree or disagree with the following statement? “I can help my child eat a diet that is healthy.” (Circle one.)
1. Strongly agree
2. Agree
3. Disagree
4. Strongly disagree
Questions on Materials Your Child Got at School
Your child got four picture books called, “The Eagle Books.” These books help children understand why it is important to eat healthy and get exercise. How many Eagle books did you or someone else in your household read to your child? (Circle one.)
1. None
2. One
3. Two
4. Three
5. Four
6. Did not get books
Your child’s teacher sent home recipes for healthy meals and snacks. How many recipes did you or someone else in your household use to make a snack or meal for your child? (Circle one.)
1. None
2. One
3. Two
4. Three
5. Four
6. Did not get recipes
Did your child help you or someone else in your household make snacks or meals using the recipes? (Circle one.)
1. Yes, all or most of them
2. Yes, some of them
3. No
4. Did not get recipes
Your child got a worksheet that asked about healthy and less healthy eating behaviors. Did you or someone else in your household help your child complete and return the worksheet to your child’s teacher? (Circle one.)
1. Yes
2. No
3. Did not get health homework
How easy was it to understand the Eagle books, recipes, worksheet, and other materials and activities sent home with your child? (Circle one.)
1. Very easy
2. Easy
3. Somewhat easy
4. Not very easy
5. Not at all easy
6. Did not read or use these materials and activities
How useful were the Eagle books, recipes, worksheet, and other materials and activities in helping you to get your child to eat healthier? (Circle one.)
1. Very useful
2. Useful
3. Somewhat useful
4. Not very useful
5. Not at all useful
6. Did not read or use these materials and activities
Please share any comments about the Eagle books, recipes, worksheet, and other materials and activities.
Thank you for completing
our survey.
Please return the survey in the enclosed envelope.
OMB No. 0584-NEW
Expiration date: XX/XXXX
See OMB statement on inside cover
What Does Your Child Eat?
|
|
Thank you for taking part in this important study!
Please fill out and return the survey in the enclosed envelope within the next week.
If you have any questions about the What Does Your Child Eat? study, please send an e-mail to xxxx@rti.org or call toll-free at 1-800-xxx-xxxx.
Public reporting burden for this collection of information is estimated to average 15 minutes per response, including the time for reviewing instructions, searching existing data sources, gathering and maintaining the data needed, and completing and reviewing the collection of information.
An agency may not conduct or sponsor, and a person is not required to respond to, a collection of information unless it displays a currently valid OMB control number.
Send comments regarding this burden estimate or any other aspect of this collection of information, including suggestions for reducing this burden, to: U.S. Department of Agriculture, Food and Nutrition Services, Office of Research and Analysis, Room 1014, Alexandria, VA 22302 ATTN: PRA (0584-xxxx*). Do not return the completed form to this address.
If you have questions regarding your rights as a research participant, you may contact RTI’s Office of Research Protection toll-free at 866-214-2043.
What
Does Your Child Eat?
Mail Questionnaire (Post-survey, Control
Group)
Instrument for CNNS Impact Evaluation
This survey asks about what your child eats. This study is being sponsored by the U.S. Department of Agriculture’s Food & Nutrition Service and conducted by RTI International, a non-profit research organization. The survey will take about 15 to 20 minutes to complete. You will receive $15 for completing this survey.
All of your answers to the survey will be kept private. We will not share your answers with anyone. You may skip any questions you do not want to answer. If you have any questions, please call XXX XXXX at RTI International at 1-800-xxx-xxxx.
Questions on Whether Certain Foods Are Available at Home
Were any of the following foods available in your home during the past week? Include fresh, frozen, canned, and dried foods. (Circle yes or no for each food.)
|
Yes |
No |
|
Yes |
No |
|
Yes |
No |
|
Yes |
No |
|
Yes |
No |
|
Yes |
No |
|
Yes |
No |
|
Yes |
No |
|
Yes |
No |
|
Yes |
No |
|
Yes |
No |
Questions on the Fruits and Vegetables Your Child Eats
For the next questions think about what your child ate during the past week, or the past 7 days. Do not include school or day care time.
How many days during the past week did your child eat more than one kind of fruit each day? Do not include fruit juice. (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
During the past week, how many cups of fruit did your child eat each day? Do not include fruit juice. (Circle one.)
1. None
2. 1/2 cup
3. 1 cup
4. 1 ½ cups
5. 2 cups
None
1 cup
2 cups
3 cups
6. 2 ½ cups
7. 3 cups or more
How many days during the past week did your child eat more than one kind of vegetable each day? Do not include vegetable juice. (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
During the past week, how many cups of vegetables did your child eat each day? Do not include vegetable juice. (Circle one.)
1. None
2. 1/2 cup
3. 1 cup
4. 1 ½ cups
5. 2 cups
None
1 cup
2 cups
3 cups
6. 2 ½ cups
7. 3 cups or more
During the past week, did your child eat any meals or snacks that were provided by his or her school or day care? (Circle all that apply.)
1. Yes, breakfast
2. Yes, lunch
3. Yes, snacks
4. No, did not eat breakfast, lunch, or snacks provided by school or day care
Is your child willing to try a new kind of fruit? (Circle one.)
1. No
2. Maybe
3. Yes
How many days during the past week did you give your child fruit as a snack? (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
How many days during the past week did your child ask or help himself or herself to fruit for a snack? (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
How many days during the past week did you give your child fruit at dinner? (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
Is your child willing to try a new kind of vegetable? (Circle one.)
1. No
2. Maybe
3. Yes
How many days during the past week did you give your child a vegetable as a snack? (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
How many days during the past week did your child ask or help himself or herself to vegetables as a snack? (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
How many days during the past week did you give your child a vegetable at dinner? (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
Questions on Your Child’s Eating Habits
How many days during the past week did your child help you make a snack or cook a meal? For example, did your child wash fruits or vegetables or crack an egg? (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
How much do you agree or disagree with the following statement? “If my child eats healthy, he or she will be healthier when he or she gets older.” (Circle one.)
1. Strongly agree
2. Agree
3. Disagree
4. Strongly disagree
How much do you agree or disagree with the following statement? “I am a good role model for my child by eating healthy foods.” (Circle one.)
1. Strongly agree
2. Agree
3. Disagree
4. Strongly disagree
How strongly do you agree or disagree with the following statement? “I can help my child eat a diet that is healthy.” (Circle one.)
1. Strongly agree
2. Agree
3. Disagree
4. Strongly disagree
Thank you for completing
our survey.
Please return the survey in the enclosed envelope.
OMB No. 0584-NEW
Expiration date: XX/XXXX
What
Does Your Child Eat?
Telephone Questionnaire for Nonrespondents
to Mail Survey
(Pre- and Post-surveys, Intervention and Control Groups)
Instrument for CNNS Impact Evaluation
To begin the survey, I’m going to read a list of foods. For each food, please tell me if it was available in your home during the past week. Please include fresh, frozen, canned, and dried foods. Answer yes or no for each food. The first food is…
|
YES |
NO |
DK |
RF |
|
YES |
NO |
DK |
RF |
|
YES |
NO |
DK |
RF |
|
YES |
NO |
DK |
RF |
|
YES |
NO |
DK |
RF |
|
YES |
NO |
DK |
RF |
|
YES |
NO |
DK |
RF |
|
YES |
NO |
DK |
RF |
|
YES |
NO |
DK |
RF |
|
YES |
NO |
DK |
RF |
|
YES |
NO |
DK |
RF |
For the next set of questions think about what your child ate during the past week, or the past 7 days. Do not include school or day care time.
How many days during the past week did your child eat more than one kind of fruit each day? Do not include fruit juice. Would you say…? SELECT ONE.
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
-4. DON’T KNOW
-7. REFUSAL
During the past week, how many cups of fruit did your child eat each day? Do not include fruit juice. Would you say your child had…? SELECT ONE.
1. No fruit
2. ½ cup
3. 1 cup
4. 1 ½ cups
5. 2 cups
6. 2 ½ cups
7. 3 cups or more
-4. DON’T KNOW
-7. REFUSAL
How many days during the past week did your child eat more than one kind of vegetable each day? Do not include vegetable juice. Would you say…? SELECT ONE.
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
-4. DON’T KNOW
-7. REFUSAL
During the past week, how many cups of vegetables did your child eat each day? Do not include vegetable juice. Would you say your child had…? SELECT ONE.
1. No vegetables
2. ½ cup
3. 1 cup
4. 1 ½ cups
5. 2 cups
6. 2 ½ cups
7. 3 cups or more
-4. DON’T KNOW
-7. REFUSAL
During the past week, did your child eat any meals or snacks that were provided by his or her school or day care? Would you say…? SELECT ALL THAT APPLY.
1. Yes, breakfast
2. Yes, lunch
3. Yes, snacks
4. No, did not eat breakfast, lunch, or snacks provided by school or day care
-4. DON’T KNOW
-7. REFUSAL
Is your child willing to try a new kind of fruit? Would you say…? SELECT ONE.
1. No
2. Maybe
3. Yes
-4. DON’T KNOW
-7. REFUSAL
How many days during the past week did you give your child fruit as a snack? Would you say…? SELECT ONE.
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
-4. DON’T KNOW
-7. REFUSAL
How many days during the past week did your child ask or help himself or herself to fruit for a snack? Would you say…? SELECT ONE.
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
-4. DON’T KNOW
-7. REFUSAL
How many days during the past week did you give your child fruit at dinner? Would you say…? SELECT ONE.
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
-4. DON’T KNOW
-7. REFUSAL
Is your child willing to try a new kind of vegetable? Would you say…? SELECT ONE.
1. No
2. Maybe
3. Yes
-4. DON’T KNOW
-7. REFUSAL
How many days during the past week did you give your child a vegetable as a snack? Would you say…? SELECT ONE.
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
-4. DON’T KNOW
-7. REFUSAL
How many days during the past week did your child ask or help himself or herself to vegetables for a snack? Would you say…? SELECT ONE.
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
-4. DON’T KNOW
-7. REFUSAL
How many days during the past week did you give your child a vegetable at dinner? Would you say…? SELECT ONE.
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
-4. DON’T KNOW
-7. REFUSAL
How many days during the past week did your child help you make a snack or cook a meal? For example, did your child wash fruits or vegetables or crack an egg? Would you say…? SELECT ONE.
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
-4. DON’T KNOW
-7. REFUSAL
For the next three questions, I’m going to read you a statement. For each statement, please tell me whether you strongly agree, agree, disagree, or strongly disagree with the statement.
First, how much do you agree or disagree with the following statement? “If my child eats healthy, he or she will be healthier when he or she gets older.” Would you say…? SELECT ONE.
1. Strongly agree
2. Agree
3. Disagree
4. Strongly disagree
-4. DON’T KNOW
-7. REFUSAL
How much do you agree or disagree with the following statement? “I am a good role model for my child by eating healthy foods.” Would you say…? SELECT ONE.
1. Strongly agree
2. Agree
3. Disagree
4. Strongly disagree
-4. DON’T KNOW
-7. REFUSAL
How strongly do you agree or disagree with the following statement? “I can help my child eat a diet that is healthy.” Would you say…? SELECT ONE.
1. Strongly agree
2. Agree
3. Disagree
4. Strongly disagree
-4. DON’T KNOW
-7. REFUSAL
[IF ADMINISTRATION IS PRE-SURVEY/BASELINE, BOTH INTERVENTION AND CONTROL GROUPS, GO TO Q26.]
[IF ADMINISTRATION IS POST-SURVEY, CONTROL GROUP ONLY, GO TO Q33.]
The last set of questions asks about materials your child got at school and may have brought home.
First, your child got four picture books called, “The Eagle Books.” These books help children understand why it is important to eat healthy and get exercise. How many Eagle books did you or someone else in your household read to your child? Would you say…? SELECT ONE.
1. None
2. One
3. Two
4. Three
5. Four
6. DID NOT GET BOOKS
-4. DON’T KNOW
-7. REFUSAL
Your child’s teacher sent home recipes for healthy meals and snacks. How many recipes did you or someone else in your household use to make a snack or meal for your child? Would you say…? SELECT ONE.
1. None
2. One
3. Two
4. Three
5. Four
6. DID NOT GET RECIPES [Go to Question 22.]
-4. DON’T KNOW
-7. REFUSAL
Did your child help you or someone else in your household make snacks or meals using the recipes? Would you say…? SELECT ONE.
1. Yes, all or most of them
2. Yes, some of them
3. No
4. DID NOT GET RECIPES
-4. DON’T KNOW
-7. REFUSAL
Your child got a worksheet that asked about healthy and less healthy eating behaviors. Did you or someone else in your household help your child complete and return the worksheet to your child’s teacher? SELECT ONE.
1. YES
2. NO
3. DID NOT GET HEALTH HOMEWORK
-4. DON’T KNOW
-7. REFUSAL
How easy was it to understand the Eagle books, recipes, worksheet, and other materials and activities sent home with your child? Would you say…? SELECT ONE.
1. Very easy
2. Easy
3. Somewhat easy
4. Not very easy
5. Not at all easy
6. DID NOT READ OR USE THESE MATERIALS AND ACTIVITIES [Go to Question 25.]
-4. DON’T KNOW
-7. REFUSAL
How useful were the Eagle books, recipes, worksheet, and other materials and activities in helping you to get your child to eat healthier? Would you say…? SELECT ONE.
1. Very useful
2. Useful
3. Somewhat useful
4. Not very useful
5. Not at all useful
6. DID NOT READ OR USE THESE MATERIALS AND ACTIVITIES
-4. DON’T KNOW
-7. REFUSAL
Please share any comments about the Eagle books, recipes, worksheet, and other materials and activities.
[ALL GO TO QUESTION 33.]
During the past year, how often did you run out of food before the end of the month? SELECT ONE.
1. Did not run out of food
2. Seldom
3. Sometimes
4. Most of the time
5. Almost always
-4. DON’T KNOW
-7. REFUSAL
How many people under 18 years of age live in your household?
____
-4. DON’T KNOW
-7. REFUSAL
Including yourself, how many people 18 years of age or older live in your household?
____
-4. DON’T KNOW
-7. REFUSAL
Which of the following categories best describes your age? SELECT ONE.
1. 18 to 24
2. 25 to 34
3. 35 to 44
4. 45 to 54
5. 55 to 64
6. 65 to 74
7. Over 74
-4. DON’T KNOW
-7. REFUSAL
What is your gender? SELECT ONE.
1. MALE
2. FEMALE
-4. DON’T KNOW
-7. REFUSAL
Are you Hispanic or Latino? SELECT ONE.
1. YES
2. NO
-4. DON’T KNOW
-7. REFUSAL
What is your race? SELECT ALL THAT APPLY.
1. American Indian or Alaska Native
2. Asian
3. Black or African American
4. Native Hawaiian or other Pacific Islander
5. White
-4. DON’T KNOW
-7. REFUSAL
33. That is all the questions I have. Thank you for completing our survey. Before saying goodbye, I’d like to confirm that I have your correct name and address for sending your cash incentive in appreciation for completing this survey. I have [RESPONDENT NAME] spelled _____________________. Is this correct?
YES
CORRECT NAME [PROGRAMMER – SET UP TO ENTER CORRECTIONS]
-7. REFUSAL
34. For your street address, I have [RESPONDENT STREET ADDRESS] Is this correct?
YES
NO [PROGRAMMER – SET UP TO ENTER CORRECT ADDRESS]
-7. REFUSAL
35. For your city, state, and zip code, I have [RESPONDENT CITY, STATE, ZIP CODE] Is this correct?
YES
CORRECT CITY
CORRECT STATE
CORRECT ZIPCODE [PROGRAMMER – SET UP TO ALLOW FOR GENERATION OF ADDRESS LABELS FOR INCENTIVE LETTERS]
-7. REFUSAL
Thank you again. Have a nice (day/evening).
Impact Evaluation Instrument for the University of Nevada
For the University of Nevada project, we will survey parents/caregivers of preschool children at pre- and post-intervention. We will administer the survey to parents/caregivers in-person at their child’s Head Start Center at scheduled interview times. We will coordinate scheduling the in-person interviews with University of Nevada, and randomly rotate the order of the two surveys. During the interview, we will collect parents/caregivers’ contact information so that we can survey them at post-intervention using a mail/telephone survey approach. We provide the following four versions of the instrument:
interviewer-administered questionnaire (pre-survey - intervention and control groups),
mail questionnaire (post-survey - intervention group),
mail questionnaire (post-survey - control group), and
telephone questionnaire for nonrespondents to mail survey (post-survey - intervention and control groups).
English and Spanish versions are provided. The Spanish translation takes into consideration the Mexican population in Nevada.
English Version
O
Date:___________________ Time:______________________
Expiration date: XX/XXXX
What
Does Your Child Eat?
Interviewer-administered Questionnaire
(Pre-survey, Intervention and Control Groups)
Instrument for University of Nevada Impact Evaluation
To begin the survey, I’m going to read a list of foods. For each food, please tell me if it was available in your home during the past week. Please include fresh, frozen, canned, and dried foods. Answer yes or no for each food. The first food is…
a. Bananas |
YES |
NO |
DK |
RF |
b. Apples |
YES |
NO |
DK |
RF |
c. Grapes |
YES |
NO |
DK |
RF |
d. Mangoes |
YES |
NO |
DK |
RF |
e. Kiwis |
YES |
NO |
DK |
RF |
f. Carrots |
YES |
NO |
DK |
RF |
g. Jicamas |
YES |
NO |
DK |
RF |
h. Potato chips, nacho chips, or corn chips |
YES |
NO |
DK |
RF |
i. Graham crackers |
YES |
NO |
DK |
RF |
j. String cheese |
YES |
NO |
DK |
RF |
k. Regular soft drinks or sodas |
YES |
NO |
DK |
RF |
l. Diet or low calorie soft drinks or sodas |
YES |
NO |
DK |
RF |
For the next questions think about what your child ate during the past week, or the past 7 days. Do not include school or day care time.
How many days during the past week did your child eat more than one kind of fruit each day? Do not include fruit juice. Would you say…? SELECT ONE.
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
-4. DON’T KNOW
-7. REFUSAL
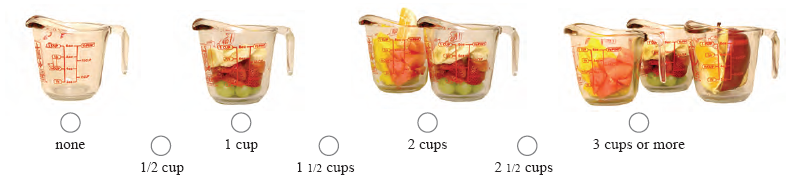
During the past week, how many cups of fruit did your child eat each day? Do not include fruit juice. Would you say your child had…? GIVE RESPONDENT PICTURE OF CUPS. SELECT ONE.
1. No fruit
2. ½ cup
3. 1 cup
4. 1 ½ cups
5. 2 cups
6. 2 ½ cups
7. 3 cups or more
-4. DON’T KNOW
-7. REFUSAL
How many days during the past week did your child eat more than one kind of vegetable each day? Do not include vegetable juice. Would you say…? SELECT ONE.
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
-4. DON’T KNOW
-7. REFUSAL
During the past week, how many cups of vegetables did your child eat each day? Do not include vegetable juice. Would you say your child had …? GIVE RESPONDENT PICTURE OF CUPS. SELECT ONE.
1. No vegetables
2. ½ cup
3. 1 cup
4. 1 ½ cups
5. 2 cups
6. 2 ½ cups
7. 3 cups or more
-4. DON’T KNOW
-7. REFUSAL
During the past week, did your child eat any meals or snacks that were provided by his or her school or day care? Would you say…? SELECT ALL THAT APPLY.
1. Yes, breakfast
2. Yes, lunch
3. Yes, snacks
4. No, did not eat breakfast, lunch, or snacks provided by school or day care
-4. DON’T KNOW
-7. REFUSAL
Is your child willing to try a new kind of fruit? Would you say…? SELECT ONE.
1. No
2. Maybe
3. Yes
-4. DON’T KNOW
-7. REFUSAL
How many days during the past week did you give your child fruit as a snack? Would you say…? SELECT ONE.
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
-4. DON’T KNOW
-7. REFUSAL
How many days during the past week did your child ask or help himself or herself to fruit for a snack? Would you say…? SELECT ONE.
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
-4. DON’T KNOW
-7. REFUSAL
How many days during the past week did you give your child fruit at dinner? Would you say…? SELECT ONE.
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
-4. DON’T KNOW
-7. REFUSAL
Is your child willing to try a new kind of vegetable? Would you say…? SELECT ONE.
1. No
2. Maybe
3. Yes
-4. DON’T KNOW
-7. REFUSAL
How many days during the past week did you give your child a vegetable as a snack? Would you say…? SELECT ONE.
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
-4. DON’T KNOW
-7. REFUSAL
How many days during the past week did your child ask or help himself or herself to vegetables for a snack? Would you say…? SELECT ONE.
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
-4. DON’T KNOW
-7. REFUSAL
How many days during the past week did you give your child a vegetable at dinner? Would you say…? SELECT ONE.
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
-4. DON’T KNOW
-7. REFUSAL
How many days during the past week did you make your child eat everything on his or her dinner plate? Would you say…? SELECT ONE.
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
-4. DON’T KNOW
-7. REFUSAL
During the past month, when ordering food for your child at a fast food restaurant, how often did you order fruits or vegetables (for example, apple slices or carrot sticks) instead of French fries? Would you say…? SELECT ONE.
1. DID NOT EAT AT FAST FOOD RESTAURANTS [Go to Question 18.]
2. Never
3. Seldom
4. Sometimes
5. Most of the times
6. Almost always
-4. DON’T KNOW
-7. REFUSAL
During the past month, when eating out at a fast food restaurant, how often did your child ask for fruits or vegetables (for example, apple slices or carrot sticks) instead of French fries? Would you say…? SELECT ONE.
1. DID NOT EAT AT FAST FOOD RESTAURANTS
2. Never
3. Seldom
4. Sometimes
5. Most of the times
6. Almost always
-4. DON’T KNOW
-7. REFUSAL
For the next two questions, I’m going to read a statement. For each statement, please tell me if you strongly agree, agree, disagree, or strongly disagree with the statement.
How much do you agree or disagree with the following statement? “If my child eats healthy, he or she will be healthier when he or she gets older.” Would you say…? SELECT ONE.
1. Strongly agree
2. Agree
3. Disagree
4. Strongly disagree
-4. DON’T KNOW
-7. REFUSAL
How much do you agree or disagree with the following statement? “I am a good role model for my child by eating healthy foods.” Would you say…? SELECT ONE.
1. Strongly agree
2. Agree
3. Disagree
4. Strongly disagree
-4. DON’T KNOW
-7. REFUSAL
During the past year, how often did you run out of food before the end of the month? SELECT ONE.
1. Did not run out of food
2. Seldom
3. Sometimes
4. Most of the time
5. Almost always
-4. DON’T KNOW
-7. REFUSAL
How many people under 18 years of age live in your household?
____
-4. DON’T KNOW
-7. REFUSAL
Including yourself, how many people 18 years of age or older live in your household?
____
-4. DON’T KNOW
-7. REFUSAL
Which of the following categories best describes your age? SELECT ONE.
1. 18 to 24
2. 25 to 34
3. 35 to 44
4. 45 to 54
5. 55 to 64
6. 65 to 74
7. Over 74
-4. DON’T KNOW
-7. REFUSAL
What is your gender? SELECT ONE.
1. MALE
2. FEMALE
-4. DON’T KNOW
-7. REFUSAL
Are you Hispanic or Latino? SELECT ONE.
1. YES
2. NO
-4. DON’T KNOW
-7. REFUSAL
What is your race? SELECT ALL THAT APPLY.
1. American Indian or Alaska Native
2. Asian
3. Black or African American
4. Native Hawaiian or other Pacific Islander
5. White
-4. DON’T KNOW
-7. REFUSAL
Does your family speak English at home? Would you say … SELECT ONE.
1. Speak English all of the time at home.
2. Speak English some of the time at home and speak another language some of the time.
3. Never speak English at home. We speak another language.
-4. DON’T KNOW
-7. REFUSAL
Thank
you for completing our survey.
|
3 cups |
|
|
3 cups |
|
|
|
||||
|
|
|
|
||
2 cups |
2 cups |
|
|||
|
|
|
|||
1 cup |
1 cup |
|
|||
|
|
|
|||
None |
|||||
None |
|


OMB No. 0584-NEW
Expiration date: XX/XXXX
See OMB statement on inside cover
What Does Your Child Eat?
|
|
Thank you for taking part in this important study!
Please fill out and return the survey in the enclosed envelope within the next week.
If you have any questions about the What Does Your Child Eat? study, please send an e-mail to xxxx@rti.org or call toll-free at 1-800-xxx-xxxx.
Public reporting burden for this collection of information is estimated to average 15 minutes per response, including the time for reviewing instructions, searching existing data sources, gathering and maintaining the data needed, and completing and reviewing the collection of information.
An agency may not conduct or sponsor, and a person is not required to respond to, a collection of information unless it displays a currently valid OMB control number.
Send comments regarding this burden estimate or any other aspect of this collection of information, including suggestions for reducing this burden, to: U.S. Department of Agriculture, Food and Nutrition Services, Office of Research and Analysis, Room 1014, Alexandria, VA 22302 ATTN: PRA (0584-xxxx*). Do not return the completed form to this address.
If you have questions regarding your rights as a research participant, you may contact RTI’s Office of Research Protection toll-free at 866-214-2043.
What
Does Your Child Eat?
Mail Questionnaire (Post-survey,
Intervention Group)
Instrument for University of Nevada Impact Evaluation
This survey asks about what your child eats. This study is being sponsored by the U.S. Department of Agriculture’s Food & Nutrition Service and conducted by RTI International, a non-profit research organization. The survey will take about 15 to 20 minutes to complete. You will receive $15 for completing this survey.
All of your answers to the survey will be kept private. We will not share your answers with anyone. You may skip any questions you do not want to answer. If you have any questions, please call xxxx xxxx at RTI International at 1-800-xxx-xxxx.
Questions on Whether Certain Foods Are Available at Home
Were any of the following foods available in your home during the past week? Include fresh, frozen, canned, and dried foods. (Circle yes or no for each food.)
a. Bananas |
Yes |
No |
b. Apples |
Yes |
No |
c. Grapes |
Yes |
No |
d. Mangoes |
Yes |
No |
e. Kiwis |
Yes |
No |
f. Carrots |
Yes |
No |
g. Jicamas |
Yes |
No |
h. Potato chips, nacho chips, or corn chips |
Yes |
No |
i. Graham crackers |
Yes |
No |
j. String cheese |
Yes |
No |
k. Regular soft drinks or sodas |
Yes |
No |
l. Diet or low calorie soft drinks or sodas |
Yes |
No |
Questions on the Fruits and Vegetables Your Child Eats
For the next questions think about what your child ate during the past week, or the past 7 days. Do not include school or day care time.
How many days during the past week did your child eat more than one kind of fruit each day? Do not include fruit juice. (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
During the past week, how many cups of fruit did your child eat each day? Do not include fruit juice. (Circle one.)
1. None
2. 1/2 cup
3. 1 cup
4. 1 ½ cups
5. 2 cups
None
1 cup
2 cups
3 cups
6. 2 ½ cups
7. 3 cups or more
How many days during the past week did your child eat more than one kind of vegetable each day? Do not include vegetable juice. (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
During the past week, how many cups of vegetables did your child eat each day? Do not include vegetable juice. (Circle one.)
1. None
2. 1/2 cup
3. 1 cup
4. 1 ½ cups
5. 2 cups
None
1 cup
2 cups
3 cups
6. 2 ½ cups
7. 3 cups or more
During the past week, did your child eat any meals or snacks that were provided by his or her school or day care? (Circle all that apply.)
1. Yes, breakfast
2. Yes, lunch
3. Yes, snacks
4. No, did not eat breakfast, lunch, or snacks provided by school or day care
Is your child willing to try a new kind of fruit? (Circle one.)
1. No
2. Maybe
3. Yes
How many days during the past week did you give your child fruit as a snack? (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
How many days during the past week did your child ask or help himself or herself to fruit for a snack? (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
How many days during the past week did you give your child fruit at dinner? (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
Is your child willing to try a new kind of vegetable? (Circle one.)
1. No
2. Maybe
3. Yes
How many days during the past week did you give your child a vegetable as a snack? (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
How many days during the past week did your child ask or help himself or herself to vegetables for a snack? (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
How many days during the past week did you give your child a vegetable at dinner? (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
Questions on Your Child’s Eating Habits
How many days during the past week did you make your child eat everything on his or her dinner plate? (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
During the past month, when ordering food for your child at a fast food restaurant, how often did you order fruits or vegetables (for example, apple slices or carrot sticks) instead of French fries? (Circle one.)
1. Did not eat at fast food restaurants
2. Never
3. Seldom
4. Sometimes
5. Most of the times
6. Almost always
During the past month, when eating out at a fast food restaurant, how often did your child ask for fruits or vegetables (for example, apple slices or carrot sticks) instead of French fries? (Circle one.)
1. Did not eat at fast food restaurants
2. Never
3. Seldom
4. Sometimes
5. Most of the times
6. Almost always
How much do you agree or disagree with the following statement? “If my child eats healthy, he or she will be healthier when he or she gets older.” (Circle one.)
1. Strongly agree
2. Agree
3. Disagree
4. Strongly disagree
How much do you agree or disagree with the following statement? “I am a good role model for my child by eating healthy foods.” (Circle one.)
1. Strongly agree
2. Agree
3. Disagree
4. Strongly disagree
Questions on Materials Your Child Got at Child Care
Your child got “Smart Snack Cards.” Each card had a picture of a healthy snack food and the serving size. Did you or someone else in your household use the “Smart Snack Cards” with your child to pick a healthy snack? (Circle one.)
1. Yes
2. No
3. Did not get Smart Snack Cards
Your child got a worksheet called, “Let’s Hunt for Healthy Foods.” The worksheet asked you and your child to find specific foods at the grocery store and check them off the worksheet. Did you or someone else in your household do the worksheet with your child? (Circle one.)
1. Yes
2. No
3. Did not get worksheet
Your child got a “Hungry Meter” that helps your child know when he or she is hungry or full. Did you or someone else in your household do the “Hungry Meter” activity with your child? (Circle one.)
1. Yes
2. No
3. Did not get the Hungry Meter
How easy was it to understand the materials and activities sent home with your child? (Circle one.)
1. Very easy
2. Easy
3. Somewhat easy
4. Not very easy
5. Not at all easy
6. Did not read the materials or do the activities sent home with my child
How useful were the materials and activities in helping you to get your child to eat healthier? (Circle one.)
1. Very useful
2. Useful
3. Somewhat useful
4. Not very useful
5. Not at all useful
6. Did not read the materials or do the activities sent home with my child
Your child’s Head Start center had a Family Activity event each month for 3 months. These events talked about how to be healthy and included food tastings and dancing. Did you or someone else in your household go to any of the Family Activity events? (Circle one.)
1. Yes
2. No [Go to Question 29]
How many Family Activity events did you or someone else in your household attend? (Circle one.)
1. One
2. Two
3. Three [Go to Question 28]
Why did you decide not to go to all of the Family Activity events? (Circle all that apply.)
1. Did not know about the other events
2. The events were offered at times that did not work for me
3. Did not think the events would be useful
4. Do not like to go to events like this
5. Other reason (specify):
How useful were the Family Activity events in helping you to get your child to eat healthier? (Circle one.) [Go to Question 30 after answering this question.]
1. Very useful
2. Useful
3. Somewhat useful
4. Not very useful
5. Not at all useful
Why did you decide not to go to any of the Family Activity events? (Circle all that apply.)
1. Did not know about the events
2. The events were offered at times that did work for me
3. Did not think the events would be useful
4. Do not like to go to events like this
5. Other reason (specify):
Please share any comments about the materials, activities, and the Family Activity events.
Thank
you for completing our survey.
Please return the survey in the
enclosed envelope.
OMB No. 0584-NEW
Expiration date: XX/XXXX
See OMB statement on inside cover
What Does Your Child Eat?
|
|
Thank you for taking part in this important study!
Please fill out and return the survey in the enclosed envelope within the next week.
If you have any questions about the What Does Your Child Eat? study, please send an e-mail to xxxx@rti.org or call toll-free at 1-800-xxx-xxxx.
Public reporting burden for this collection of information is estimated to average 15 minutes per response, including the time for reviewing instructions, searching existing data sources, gathering and maintaining the data needed, and completing and reviewing the collection of information.
An agency may not conduct or sponsor, and a person is not required to respond to, a collection of information unless it displays a currently valid OMB control number.
Send comments regarding this burden estimate or any other aspect of this collection of information, including suggestions for reducing this burden, to: U.S. Department of Agriculture, Food and Nutrition Services, Office of Research and Analysis, Room 1014, Alexandria, VA 22302 ATTN: PRA (0584-xxxx*). Do not return the completed form to this address.
If you have questions regarding your rights as a research participant, you may contact RTI’s Office of Research Protection toll-free at 866-214-2043.
What
Does Your Child Eat?
Mail Questionnaire (Post-survey, Control
Group)
Instrument for University of Nevada Impact Evaluation
This survey asks about what your child eats. This study is being sponsored by the U.S. Department of Agriculture’s Food & Nutrition Service and conducted by RTI International, a non-profit research organization. The survey will take about 15 to 20 minutes to complete. You will receive $15 for completing this survey.
All of your answers to the survey will be kept private. We will not share your answers with anyone. You may skip any questions you do not want to answer. If you have any questions, please call xxxx xxxx at RTI International at 1-800-xxx-xxxx.
Questions on Whether Certain Foods Are Available at Home
Were any of the following foods available in your home during the past week? Include fresh, frozen, canned, and dried foods. (Circle yes or no for each food.)
a. Bananas |
Yes |
No |
b. Apples |
Yes |
No |
c. Grapes |
Yes |
No |
d. Mangoes |
Yes |
No |
e. Kiwis |
Yes |
No |
f. Carrots |
Yes |
No |
g. Jicamas |
Yes |
No |
h. Potato chips, nacho chips, or corn chips |
Yes |
No |
i. Graham crackers |
Yes |
No |
j. String cheese |
Yes |
No |
k. Regular soft drinks or sodas |
Yes |
No |
l. Diet or low calorie soft drinks or sodas |
Yes |
No |
Questions on the Fruits and Vegetables Your Child Eats
For the next questions think about what your child ate during the past week, or the past 7 days. Do not include school or day care time.
How many days during the past week did your child eat more than one kind of fruit each day? Do not include fruit juice. (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
During the past week, how many cups of fruit did your child eat each day? Do not include fruit juice. (Circle one.)
1. None
2. 1/2 cup
3. 1 cup
4. 1 ½ cups
5. 2 cups
None
1 cup
2 cups
3 cups
6. 2 ½ cups
7. 3 cups or more
How many days during the past week did your child eat more than one kind of vegetable each day? Do not include vegetable juice. (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
During the past week, how many cups of vegetables did your child eat each day? Do not include vegetable juice. (Circle one.)
1. None
2. 1/2 cup
3. 1 cup
4. 1 ½ cups
5. 2 cups
None
1 cup
2 cups
3 cups
6. 2 ½ cups
7. 3 cups or more
During the past week, did your child eat any meals or snacks that were provided by his or her school or day care? (Circle all that apply.)
1. Yes, breakfast
2. Yes, lunch
3. Yes, snacks
4. No, did not eat breakfast, lunch, or snacks provided by school or day care
Is your child willing to try a new kind of fruit? (Circle one.)
1. No
2. Maybe
3. Yes
How many days during the past week did you give your child fruit as a snack? (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
How many days during the past week did your child ask or help himself or herself to fruit for a snack? (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
How many days during the past week did you give your child fruit at dinner? (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
Is your child willing to try a new kind of vegetable? (Circle one.)
1. No
2. Maybe
3. Yes
How many days during the past week did you give your child a vegetable as a snack? (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
How many days during the past week did your child ask or help himself or herself to vegetables for a snack? (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
How many days during the past week did you give your child a vegetable at dinner? (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
Questions on Your Child’s Eating Habits
How many days during the past week did you make your child eat everything on his or her dinner plate? (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
During the past month, when ordering food for your child at a fast food restaurant, how often did you order fruits or vegetables (for example, apple slices or carrot sticks) instead of French fries? (Circle one.)
1. Did not eat at fast food restaurants
2. Never
3. Seldom
4. Sometimes
5. Most of the times
6. Almost always
During the past month, when eating out at a fast food restaurant, how often did your child ask for fruits or vegetables (for example, apple slices or carrot sticks) instead of French fries? (Circle one.)
1. Did not eat at fast food restaurants
2. Never
3. Seldom
4. Sometimes
5. Most of the times
6. Almost always
How much do you agree or disagree with the following statement? “If my child eats healthy, he or she will be healthier when he or she gets older.” (Circle one.)
1. Strongly agree
2. Agree
3. Disagree
4. Strongly disagree
How much do you agree or disagree with the following statement? “I am a good role model for my child by eating healthy foods.” (Circle one.)
1. Strongly agree
2. Agree
3. Disagree
4. Strongly disagree
Thank
you for completing our survey.
Please return the survey in the
enclosed envelope.
OMB No. 0584-NEW
Expiration date: XX/XXXX
What
Does Your Child Eat?
Telephone Questionnaire for Nonrespondents
(Post-survey, Intervention and Control Groups)
Instrument for University of Nevada Impact Evaluation
To begin the survey, I’m going to read a list of foods. For each food, please tell me if it was available in your home during the past week? Please include fresh, frozen, canned, and dried foods. Answer yes or no for each food. The first food is…
a. Bananas |
YES |
NO |
DK |
RF |
b. Apples |
YES |
NO |
DK |
RF |
c. Grapes |
YES |
NO |
DK |
RF |
d. Mangoes |
YES |
NO |
DK |
RF |
e. Kiwis |
YES |
NO |
DK |
RF |
f. Carrots |
YES |
NO |
DK |
RF |
g. Jicamas |
YES |
NO |
DK |
RF |
h. Potato chips, nacho chips, or corn chips |
YES |
NO |
DK |
RF |
i. Graham crackers |
YES |
NO |
DK |
RF |
j. String cheese |
YES |
NO |
DK |
RF |
k. Regular soft drinks or sodas |
YES |
NO |
DK |
RF |
l. Diet or low calorie soft drinks or sodas |
YES |
NO |
DK |
RF |
For the next questions think about what your child ate during the past week, or the past 7 days. Do not include school or day care time.
How many days during the past week did your child eat more than one kind of fruit each day? Do not include fruit juice. Would you say…? SELECT ONE.
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
-4. DON’T KNOW
-7. REFUSAL
During the past week, how many cups of fruit did your child eat each day? Do not include fruit juice. Would you say your child had…? SELECT ONE.
1. No fruit
2. ½ cup
3. 1 cup
4. 1 ½ cups
5. 2 cups
6. 2 ½ cups
7. 3 cups or more
-4. DON’T KNOW
-7. REFUSAL
How many days during the past week did your child eat more than one kind of vegetable each day? Do not include vegetable juice. Would you say…? SELECT ONE.
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
-4. DON’T KNOW
-7. REFUSAL
During the past week, how many cups of vegetables did your child eat each day? Do not include vegetable juice. Would you say your child had …? SELECT ONE.
1. No vegetables
2. ½ cup
3. 1 cup
4. 1 ½ cups
5. 2 cups
6. 2 ½ cups
7. 3 cups or more
-4. DON’T KNOW
-7. REFUSAL
During the past week, did your child eat any meals or snacks that were provided by his or her school or day care? Would you say…? SELECT ALL THAT APPLY.
1. Yes, breakfast
2. Yes, lunch
3. Yes, snacks
4. No, did not eat breakfast, lunch, or snacks provided by school or day care
-4. DON’T KNOW
-7. REFUSAL
Is your child willing to try a new kind of fruit? Would you say…? SELECT ONE.
1. No
2. Maybe
3. Yes
-4. DON’T KNOW
-7. REFUSAL
How many days during the past week did you give your child fruit as a snack? Would you say…? SELECT ONE.
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
-4. DON’T KNOW
-7. REFUSAL
How many days during the past week did your child ask or help himself or herself to fruit for a snack? Would you say…? SELECT ONE.
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
-4. DON’T KNOW
-7. REFUSAL
How many days during the past week did you give your child fruit at dinner? Would you say…? SELECT ONE.
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
-4. DON’T KNOW
-7. REFUSAL
Is your child willing to try a new kind of vegetable? Would you say…? SELECT ONE.
1. No
2. Maybe
3. Yes
-4. DON’T KNOW
-7. REFUSAL
How many days during the past week did you give your child a vegetable as a snack? Would you say…? SELECT ONE.
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
-4. DON’T KNOW
-7. REFUSAL
How many days during the past week did your child ask or help himself or herself to vegetables for a snack? Would you say…? SELECT ONE.
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
-4. DON’T KNOW
-7. REFUSAL
How many days during the past week did you give your child a vegetable at dinner? Would you say…? SELECT ONE.
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
-4. DON’T KNOW
-7. REFUSAL
How many days during the past week did you make your child eat everything on his or her dinner plate? Would you say…? SELECT ONE.
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
-4. DON’T KNOW
-7. REFUSAL
During the past month, when ordering food for your child at a fast food restaurant, how often did you order fruits or vegetables (for example, apple slices or carrot sticks) instead of French fries? Would you say…? SELECT ONE.
1. DID NOT EAT AT FAST FOOD RESTAURANTS [Go to Question 18.]
2. Never
3. Seldom
4. Sometimes
5. Most of the times
6. Almost always
-4. DON’T KNOW
-7. REFUSAL
During the past month, when eating out at a fast food restaurant, how often did your child ask for fruits or vegetables (for example, apple slices or carrot sticks) instead of French fries? Would you say…? SELECT ONE.
1. DID NOT EAT AT FAST FOOD RESTAURANTS
2. Never
3. Seldom
4. Sometimes
5. Most of the times
6. Almost always
-4. DON’T KNOW
-7. REFUSAL
For the next two questions, I’m going to read a statement. For each statement, please tell me if you strongly agree, agree, disagree, or strongly disagree with the statement.
How much do you agree or disagree with the following statement? “If my child eats healthy, he or she will be healthier when he or she gets older.” Would you say…? SELECT ONE.
1. Strongly agree
2. Agree
3. Disagree
4. Strongly disagree
-4. DON’T KNOW
-7. REFUSAL
How much do you agree or disagree with the following statement? “I am a good role model for my child by eating healthy foods.” Would you say…? SELECT ONE.
1. Strongly agree
2. Agree
3. Disagree
4. Strongly disagree
-4. DON’T KNOW
-7. REFUSAL
[IF CONTROL GROUP THEN GO TO Q31]
The last set of questions asks about materials your child got at school and may have brought home.
Your child got “Smart Snack Cards.” Each card had a picture of a healthy snack food and the serving size. Did you or someone else in your household use the “Smart Snack Cards” with your child to pick a healthy snack? SELECT ONE.
1. YES
2. NO
3. DID NOT GET SMART SNACK CARDS
-4. DON’T KNOW
-7. REFUSAL
Your child got a worksheet called, “Let’s Hunt for Healthy Foods.” The worksheet asked you and your child to find specific foods at the grocery store and check them off the worksheet. Did you or someone else in your household do the worksheet with your child? SELECT ONE.
1. YES
2. NO
3. DID NOT GET WORKSHEET
-4. DON’T KNOW
-7. REFUSAL
Your child got a “Hungry Meter” that helps your child know when he or she is hungry or full. Did you or someone else in your household do the “Hungry Meter” activity with your child? SELECT ONE.
1. YES
2. NO
3. DID NOT GET HUNGRY METER
-4. DON’T KNOW
-7. REFUSAL
How easy was it to understand the materials and activities sent home with your child? SELECT ONE.
1. Very easy
2. Easy
3. Somewhat easy
4. Not very easy
5. Not at all easy
6. DID NOT READ THE MATERIALS OR DO THE ACTIVITIES SENT HOME WITH MY CHILD [Go to Question 25.]
-4. DON’T KNOW
-7. REFUSAL
How useful were the materials and activities in helping you to get your child to eat healthier? SELECT ONE.
1. Very useful
2. Useful
3. Somewhat useful
4. Not very useful
5. Not at all useful
6. DID NOT READ THE MATERIALS OR DO THE ACTIVITIES SENT HOME WITH MY CHILD
-4. DON’T KNOW
-7. REFUSAL
Your child’s Head Start center had a Family Activity event each month for 3 months. These events talked about how to be healthy and included food tastings and dancing. Did you or someone else in your household go to any of the Family Activity events? SELECT ONE.
1. YES
2. NO [Go to Question 29]
-4. DON’T KNOW [Go to Question 29]
-7. REFUSAL [Go to Question 29]
How many Family Activity events did you or someone else in your household attend? SELECT ONE.
1. One
2. Two
3. Three [Go to Question 28]
-4. DON’T KNOW [Go to Question 28]
-7. REFUSAL [Go to Question 28]
Why did you decide not to go to all of the Family Activity events? Was it because…? SELECT ALL THAT APPLY.
1. You did not know about the other events
2. The events were offered at times that did not work for you
3. You did not think the events would be useful
4. You do not like to go to events like this
5. Some other reason (SPECIFY):
-4. DON’T KNOW
-7. REFUSAL
How useful were the Family Activity events in helping you to get your child to eat healthier? Would you say…? SELECT ONE.
1. Very useful
2. Useful
3. Somewhat useful
4. Not very useful
5. Not at all useful
-4. DON’T KNOW
-7. REFUSAL
[ALL GO TO Q30.]
Why did you decide not to go to any of the Family Activity events? Was it because…? SELECT ALL THAT APPLY.
1. You did not know about the events
2. The events were offered at times that did work for you
3. You did not think the events would be useful
4. You do not like to go to events like this
5. Some other reason (SPECIFY):
-4. DON’T KNOW
-7. REFUSAL
Please share any comments about the materials, activities, and the Family Activity events.
31. That is all the questions I have. Thank you for completing our survey. Before saying goodbye, I’d like to confirm that I have your correct name and address for sending your cash incentive in appreciation for completing this survey. I have [RESPONDENT NAME] spelled _____________________. Is this correct?
YES
CORRECT NAME [PROGRAMMER – SET UP TO ENTER CORRECTIONS]
-7. REFUSAL
32. For your street address, I have [RESPONDENT STREET ADDRESS] Is this correct?
YES
NO [PROGRAMMER –SET UP TO ENTER CORRECT ADDRESS]
-7 REFUSAL
33. For your city, state, and zip code, I have [RESPONDENT CITY, STATE, ZIP CODE] Is this correct?
YES
CORRECT CITY
CORRECT STATE
CORRECT ZIPCODE [PROGRAMMER – SET UP TO ALLOW FOR GENERATION OF ADDRESS LABELS FOR INCENTIVE LETTERS]
-7. REFUSAL
Thank you again. Have a nice (day/evening).
Spanish Version
Impact Evaluation Instrument for the University of Nevada
For the University of Nevada project, we will survey parents/caregivers of preschool children at pre- and post-intervention. We will administer the survey to parents/caregivers in-person at their child’s Head Start Center at scheduled interview times. We will coordinate scheduling the in-person interviews with University of Nevada, and randomly rotate the order of the two surveys. During the interview, we will collect parents/caregivers’ contact information so that we can survey them at post-intervention using a mail/telephone survey approach. We provide the following four versions of the instrument:
1. interviewer-administered questionnaire (pre-survey - intervention and control groups),
2. mail questionnaire (post-survey - intervention group),
3. mail questionnaire (post-survey - control group), and
4. telephone questionnaire for nonrespondents to mail survey (post-survey - intervention and control groups).
OMB No. 0584-NEW
Fecha de expiración: XX/XXXX
What Does Your Child Eat?
(¿Qué come su niño?)
Interviewer-administered
Questionnaire
(Pre-survey, Intervention and Control Groups)
Instrument for University of Nevada Impact Evaluation
Para comenzar esta encuesta, le voy a leer una lista de alimentos. Por cada uno de ellos, dígame por favor si estuvo disponible ese alimento en su hogar durante la semana pasada. Por favor, incluya alimentos frescos, congelados, enlatados y secos. Responda sí o no por cada alimento. El primer alimento es…
a. Plátanos |
Sí |
NO |
DK |
RF |
b. Manzanas |
Sí |
NO |
DK |
RF |
c. Uvas |
Sí |
NO |
DK |
RF |
d. Mangos |
Sí |
NO |
DK |
RF |
e. Kiwis |
Sí |
NO |
DK |
RF |
f. Zanahorias |
Sí |
NO |
DK |
RF |
g. Jícamas |
Sí |
NO |
DK |
RF |
h. Papas fritas en bolsa, nachos u hojuelas de maíz ‘corn chips’ |
Sí |
NO |
DK |
RF |
i. Galletas dulces ‘graham’ |
Sí |
NO |
DK |
RF |
j. Queso en tiras |
Sí |
NO |
DK |
RF |
k. Gaseosas o sodas regulares |
Sí |
NO |
DK |
RF |
l. Gaseosas o sodas de dieta o de bajas calorías |
Sí |
NO |
DK |
RF |
Para las siguientes preguntas, piense sobre lo que su niño(a) comió durante la semana pasada o en los últimos 7 días. No incluya el tiempo en la escuela o la guardería infantil.
¿Cuántos días durante la semana pasada comió su niño(a) más de un tipo de fruta cada día? No incluya jugo de frutas. ¿Diría usted… SELECT ONE.
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
-4. DON’T KNOW
-7. REFUSAL
Durante la semana pasada, ¿cuántas tazas de fruta comió su niño(a) cada día? No incluya jugo de frutas. ¿Diría que su niño(a) comió…? GIVE RESPONDENT PICTURE OF CUPS. SELECT ONE.
1. Ninguna fruta
2. ½ taza
3. 1 taza
4. 1 ½ tazas
5. 2 tazas
6. 2 ½ tazas
7. 3 tazas o más
-4. DON’T KNOW
-7. REFUSAL
¿Cuántos días durante la semana pasada comió su niño(a) más de un tipo de vegetal cada día? No incluya jugo de vegetales. ¿Diría usted…? SELECT ONE.
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
-4. DON’T KNOW
-7. REFUSAL
Durante la semana pasada, ¿cuántas tazas de vegetales comió su niño(a) cada día? No incluya jugo de vegetales. ¿Diría usted que su niño(a) comió…? GIVE RESPONDENT PICTURE OF CUPS. SELECT ONE.
1. Ningún vegetal
2. ½ taza
3. 1 taza
4. 1 ½ tazas
5. 2 tazas
6. 2 ½ tazas
7. 3 tazas o más
-4. DON’T KNOW
-7. REFUSAL
Durante la semana pasada, ¿comió su niño(a) algún alimento o merienda o ‘snack’ que fue proporcionado en su escuela o guardería infantil? ¿Diría usted que…? SELECT ALL THAT APPLY.
1. Sí, en el desayuno
2. Sí, en el almuerzo
3. Sí, comió meriendas o ‘snacks’
4. No, no comió en el desayuno, almuerzo, ni meriendas o ‘snacks’ proporcionados por la escuela o guardería infantil
-4. DON’T KNOW
-7. REFUSAL
¿Está su niño(a) dispuesto(a) a probar un nuevo tipo de fruta? ¿Diría usted…? SELECT ONE.
1. No
2. Quizás
3. Sí
-4. DON’T KNOW
-7. REFUSAL
¿Cuántos días durante la semana pasada le dio usted fruta a su niño(a) como merienda o ‘snack’? ¿Diría usted…? SELECT ONE.
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
-4. DON’T KNOW
-7. REFUSAL
¿Cuántos días durante la semana pasada le pidió su niño(a) o se sirvió él o ella por sí mismo(a) fruta como merienda o ‘snack’? ¿Diría usted…? SELECT ONE.
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
-4. DON’T KNOW
-7. REFUSAL
¿Cuántos días durante la semana pasada le dio a su niño(a) fruta en la cena? ¿Diría usted…? SELECT ONE.
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
-4. DON’T KNOW
-7. REFUSAL
¿Estaría su niño(a) dispuesto(a) a probar un nuevo tipo de vegetal? ¿Diría usted…? SELECT ONE.
1. No
2. Quizás
3. Sí
-4. DON’T KNOW
-7. REFUSAL
¿Cuántos días durante la semana pasada le dio vegetales a su niño(a) como merienda o ‘snack’? ¿Diría usted…? SELECT ONE.
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
-4. DON’T KNOW
-7. REFUSAL
¿Cuántos días durante la semana pasada le pidió su niño(a) o se sirvió él o ella por sí mismo(a) vegetales como merienda o ‘snack’? ¿Diría usted…? SELECT ONE.
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
-4. DON’T KNOW
-7. REFUSAL
¿Cuántos días durante la semana pasada le dio a su niño(a) vegetales en la cena? ¿Diría usted…? SELECT ONE.
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
-4. DON’T KNOW
-7. REFUSAL
¿Cuántos días durante la semana pasada hizo usted que su niño(a) comiera todo lo que estaba en su plato de comida? ¿Diría usted…? SELECT ONE.
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
-4. DON’T KNOW
-7. REFUSAL
Durante el mes pasado, al ordenar comida para su niño(a) en un restaurante de comida rápida, ¿con qué frecuencia pidió frutas o vegetales (por ejemplo, rebanadas de manzanas o palitos de zanahorias) en lugar de papas fritas? ¿Diría usted…? SELECT ONE.
1. NO COMIÓ EN RESTAURANTES DE COMIDA RÁPIDA [Go to Question 18.]
2. Nunca
3. Rara vez
4. Algunas veces
5. La mayoría de veces
6. Casi siempre
-4. DON’T KNOW
-7. REFUSAL
Durante el mes pasado, al salir a comer a un restaurante de comida rápida, ¿con qué frecuencia pedía su niño(a) frutas o vegetales (por ejemplo, rebanadas de manzanas o palitos de zanahorias) en lugar de papas fritas? ¿Diría usted…? SELECT ONE.
1. NO COMIÓ EN RESTAURANTES DE COMIDA RÁPIDA
2. Nunca
3. Rara vez
4. Algunas veces
5. La mayoría de veces
6. Casi siempre
-4. DON’T KNOW
-7. REFUSAL
Para las siguientes dos preguntas, le voy a leer una declaración. Por cada declaración, dígame por favor si usted está muy de acuerdo, de acuerdo, en desacuerdo o muy en desacuerdo con la declaración.
¿Qué tan de acuerdo o en desacuerdo está usted con la siguiente declaración? “Si mi niño(a) come de manera saludable, él o ella será más saludable cuando tenga más edad”. ¿Diría usted…? SELECT ONE.
1. Muy de acuerdo
2. De acuerdo
3. En desacuerdo
4. Muy en desacuerdo
-4. DON’T KNOW
-7. REFUSAL
¿Qué tan de acuerdo o en desacuerdo está usted con la siguiente declaración? “Yo soy un buen ejemplo para mi niño(a) al comer alimentos saludables”. ¿Diría usted…? SELECT ONE.
1. Muy de acuerdo
2. De acuerdo
3. En desacuerdo
4. Muy en desacuerdo
-4. DON’T KNOW
-7. REFUSAL
Durante el año pasado, ¿con qué frecuencia se le acabó la comida antes de fin de mes? SELECT ONE.
1. No se acabó la comida
2. Rara vez
3. Algunas veces
4. La mayor parte del tiempo
5. Casi siempre
-4. DON’T KNOW
-7. REFUSAL
¿Cuántas personas menores de 18 años de edad viven en su hogar?
____
-4. DON’T KNOW
-7. REFUSAL
Incluyéndose usted, ¿cuántas personas de 18 años de edad o más viven en su hogar?
____
-4. DON’T KNOW
-7. REFUSAL
¿Cuál de las siguientes categorías describe mejor su edad? SELECT ONE.
1. De 18 a 24
2. De 25 a 34
3. De 35 a 44
4. De 45 a 54
5. De 55 a 64
6. De 65 a 74
7. Más de 74
-4. DON’T KNOW
-7. REFUSAL
¿Es usted hombre o mujer? SELECT ONE.
1. HOMBRE
2. MUJER
-4. DON’T KNOW
-7. REFUSAL
¿Es usted hispano(a) o latino(a)? SELECT ONE.
1. YES
2. NO
-4. DON’T KNOW
-7. REFUSAL
¿Cuál es su raza? SELECT ALL THAT APPLY.
1. India Americana o nativa de Alaska
2. Asiática
3. Negra o africana americana
4. Nativa de Hawai o de alguna otra isla del Pacífico
5. Blanca
-4. DON’T KNOW
-7. REFUSAL
¿Habla su familia inglés en el hogar? ¿Diría usted que…? SELECT ONE.
1. Hablan inglés todo el tiempo en el hogar.
2. Hablan inglés algunas veces en el hogar y también hablan otro idioma algunas veces.
3. Nunca hablan inglés en el hogar. Hablan otro idioma.
-4. DON’T KNOW
-7. REFUSAL
Gracias por completar la encuesta.
|
3 tazas |
|
|
3 tazas |
|
|
|
||||
|
|
|
|
||
2 tazas |
2 tazas |
|
|||
|
|
|
|||
1 taza |
1 taza |
|
|||
|
|
|
|||
Ninguna |
|||||
Ninguna |
|
OMB No. 0584-NEW
Fecha de expiración: XX/XXXX
Ver la declaración OMB en la parte interior de la portada
¿Qué come su niño?
|
|
¡Gracias por participar en este importante estudio!
Por favor, complete y devuelva la encuesta en el sobre adjunto a más tardar la próxima semana. Si tiene alguna pregunta sobre el estudio ¿Qué come su niño?, por favor envíe un mensaje por correo electrónico a xxxx@rti.org o llame al número gratuito 1-800-xxx-xxxx.
Se calcula que el tiempo aproximado que le tomará a cada participante en dar esta información será de 15 minutos, incluyendo el tiempo para repasar las instrucciones, buscar las fuentes de información existentes, juntar y mantener los datos requeridos, así como completar y revisar la recopilación de datos.
Ninguna agencia está autorizada a realizar o patrocinar ninguna recopilación de datos o información sin presentar un número actual de control OMB válido, ni está obligada ninguna persona a participar en una recopilación de datos si no existe dicho número.
Envíe sus comentarios acerca de este cálculo de tiempo o cualquier otro aspecto relacionado con esta recolección de datos, incluyendo sugerencias para reducir el tiempo, a: U.S. Department of Agriculture, Food and Nutrition Services, Office of Research and Analysis, Room 1014, Alexandria, VA 22302. ATTN: PRA (0584-xxxx*). No envíe el cuestionario con sus respuestas a esta dirección.
Si tiene preguntas sobre sus derechos como participante en un estudio, puede comunicarse con la Oficina de RTI para la Protección de Participantes en Estudios al número gratuito 1-866-214-2043.
What Does Your Child Eat?
(¿Qué come su niño?)
Mail Questionnaire
(Post-survey, Intervention Group)
Instrument for University of Nevada Impact Evaluation
Esta encuesta pregunta sobre lo que come su niño(a). Este estudio está patrocinado por el Servicio de Alimentos y Nutrición del Departamento de Agricultura de los Estados Unidos y lo realiza RTI International, una organización sin fines de lucro que realiza estudios sobre la salud. La encuesta tomará entre 15 y 20 minutos en completarse. Usted recibirá $15 dólares por completar la entrevista.
Todas sus respuestas a la encuesta se mantendrán privadas. Nosotros no compartiremos sus respuestas con nadie. Usted puede dejar de contestar cualquier pregunta que no desee contestar. Si tiene alguna pregunta, por favor llame a xxxx xxxx en RTI International al 1-800-xxx-xxxx.
Preguntas sobre la disponibilidad de ciertos alimentos en el hogar
¿Estuvieron disponibles algunos de los siguientes alimentos en su hogar durante la semana pasada? Incluya alimentos frescos, congelados, enlatados y secos. (Marque con un círculo la respuesta Sí o No por cada alimento).
a. Plátanos |
Sí |
No |
b. Manzanas |
Sí |
No |
c. Uvas |
Sí |
No |
d. Mangos |
Sí |
No |
e. Kiwis |
Sí |
No |
f. Zanahorias |
Sí |
No |
g. Jícamas |
Sí |
No |
h. Papas fritas en bolsa, nachos u hojuelas de maíz ‘corn chips’ |
Sí |
No |
i. Galletas dulces ‘graham’ |
Sí |
No |
j. Queso en tiras |
Sí |
No |
k. Gaseosas o sodas regulares |
Sí |
No |
l. Gaseosas o sodas de dieta o de bajas calorías |
Sí |
No |
Preguntas sobre las frutas y vegetales que come su niño(a)
Para las siguientes preguntas, piense en lo que su niño(a) comió durante la semana pasada o en los últimos 7 días. No incluya el tiempo en la escuela o la guardería infantil.
¿Cuántos días durante la semana pasada comió su niño(a) más de un tipo de fruta cada día? No incluya jugo de frutas. (Marque una respuesta con un círculo).
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
Durante la semana pasada, ¿cuántas tazas de fruta comió su niño(a) cada día? No incluya jugo de frutas. (Marque una respuesta con un círculo).
1. Ninguna
2. 1/2 taza
3. 1 taza
4. 1 ½ tazas
5. 2 tazas
Ninguna
1 taza
2 tazas
3 tazas
6. 2 ½ tazas
7. 3 tazas o más
¿Cuántos días durante la semana pasada comió su niño(a) más de un tipo de vegetal cada día? No incluya jugo de vegetales. (Marque una respuesta con un círculo).
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
Durante la semana pasada, ¿cuántas tazas de vegetales comió su niño(a) cada día? No incluya jugo de vegetales. (Marque una respuesta con un círculo).
1. Ninguna
2. 1/2 taza
3. 1 taza
4. 1 ½ tazas
5. 2 tazas
Ninguna
1 taza
2 tazas
3 tazas
6. 2 ½ tazas
7. 3 tazas o más
Durante la semana pasada, ¿comió su niño(a) algún alimento o merienda o ‘snack’ que fue proporcionado por su escuela o guardería infantil? (Marque con un círculo todas las respuestas que correspondan).
1. Sí, en el desayuno
2. Sí, en el almuerzo
3. Sí, comió meriendas o ‘snacks’
4. No, no comió desayuno, almuerzo, ni meriendas o ‘snacks’ proporcionados por la escuela o guardería infantil.
¿Está su niño(a) dispuesto a probar un nuevo tipo de fruta? (Marque una respuesta con un círculo).
1. No
2. Quizás
3. Sí
¿Cuántos días durante la semana pasada le dio usted fruta a su niño(a) como merienda o ‘snack’? (Marque una respuesta con un círculo).
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
¿Cuántos días durante la semana pasada le pidió su niño(a) o se sirvió él o ella por sí mismo(a) fruta como merienda o ‘snack’? (Marque una respuesta con un círculo).
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
¿Cuántos días durante la semana pasada le dio a su niño(a) fruta en la cena? (Marque una respuesta con un círculo).
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
¿Está su niño(a) dispuesto(a) a probar un nuevo tipo de vegetal? (Marque una respuesta con un círculo).
1. No
2. Quizás
3. Sí
¿Cuántos días durante la semana pasada le dio vegetales a su niño(a) como merienda o ‘snack’? (Marque una respuesta con un círculo).
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
¿Cuántos días durante la semana pasada le pidió su niño(a) o se sirvió él o ella por sí mismo(a) vegetales como merienda o ‘snack’? (Marque una respuesta con un círculo).
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
¿Cuántos días durante la semana pasada le dio a su niño(a) vegetales en la cena? (Marque una respuesta con un círculo).
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
Preguntas sobre los hábitos alimenticios de su niño(a)
¿Cuántos días durante la semana pasada hizo usted que su niño(a) comiera todo lo que estaba en su plato de comida? (Marque una respuesta con un círculo).
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
Durante el mes pasado, cuando ordenaba comida para su niño(a) en un restaurante de comida rápida, ¿con qué frecuencia pidió frutas o vegetales (por ejemplo, rebanadas de manzanas o palitos de zanahorias) en lugar de papas fritas? (Marque una respuesta con un círculo).
1. No comimos en restaurantes de comida rápida
2. Nunca
3. Rara vez
4. Algunas veces
5. La mayoría de veces
6. Casi siempre
Durante el mes pasado, cuando salía a comer a un restaurante de comida rápida, ¿con qué frecuencia pedía su niño(a) frutas o vegetales (por ejemplo, rebanadas de manzanas o palitos de zanahorias) en lugar de papas fritas? (Marque una respuesta con un círculo).
1. No comimos en restaurantes de comida rápida
2. Nunca
3. Rara vez
4. Algunas veces
5. La mayoría de veces
6. Casi siempre
¿Qué tan de acuerdo o en desacuerdo está usted con la siguiente declaración? “Si mi niño(a) come de manera saludable, él o ella será más saludable cuando tenga más edad”. (Marque una respuesta con un círculo).
1. Muy de acuerdo
2. De acuerdo
3. En desacuerdo
4. Muy en desacuerdo
¿Qué tan de acuerdo o en desacuerdo está usted con la siguiente declaración? “Yo soy un buen ejemplo para mi niño(a) al comer alimentos saludables”. (Marque una respuesta con un círculo).
1. Muy de acuerdo
2. De acuerdo
3. En desacuerdo
4. Muy en desacuerdo
Preguntas sobre materiales que su niño(a) recibió en la guardería infantil
Su niño recibió unas “Tarjetas inteligentes de meriendas o snacks”. Cada tarjeta tiene una foto de una merienda o ‘snack’ saludable y el tamaño de la porción. ¿Usó usted o alguien más en su hogar las “Tarjetas inteligentes de meriendas o snacks” con su niño(a) para seleccionar una merienda o ‘snack’ saludable? (Marque una respuesta con un círculo).
1. Sí
2. No
3. No recibió las Tarjetas inteligentes de meriendas o snacks
Su niño(a) recibió una hoja de tarea que se llama “Busquemos alimentos saludables”. La hoja de tarea pedía que usted y su niño(a) encuentren alimentos específicos en el supermercado y los marquen en la lista. ¿Hizo usted o alguien más en su hogar la tarea con su niño(a)? (Marque una respuesta con un círculo).
1. Sí
2. No
3. No recibió la hoja de tarea
Su niño(a) recibió un “Medidor de hambre” que ayuda a su niño(a) a saber cuando él o ella tiene hambre o está satisfecho(a). ¿Realizó usted o alguien en su hogar la actividad del “Medidor de hambre” con su niño(a)? (Marque una respuesta con un círculo).
1. Sí
2. No
3. No recibió el “Medidor de hambre”
¿Qué tan fácil fue entender los materiales y las actividades que se enviaron al hogar con su niño(a)? (Marque una respuesta con un círculo).
1. Muy fácil
2. Fácil
3. Algo fácil
4. No muy fácil
5. Nada fácil
6. No leí los materiales o no hice las actividades que se enviaron al hogar con mi niño(a)
¿Qué tan útiles fueron los materiales y las actividades para ayudarlo(a) a usted a que haga que su niño(a) coma de manera más saludable? (Marque una respuesta con un círculo).
1. Muy útil
2. Útil
3. Algo útil
4. No muy útil
5. Nada útil
6. No leí los materiales o no hice las actividades que se enviaron al hogar con mi niño(a)
El centro Head Start de su niño(a) tuvo un evento de actividad familiar cada mes durante 3 meses. Estos eventos trataban sobre cómo estar saludables y se ofrecían alimentos para probar y hubieron bailes. ¿Asistió usted o alguien más en su hogar a alguno de los eventos de actividad familiar? (Marque una respuesta con un círculo).
1. Sí
2. No [Vaya a la pregunta 29]
¿A cuántos eventos de actividad familiar asistió usted o alguien más en su hogar? (Marque una respuesta con un círculo).
1. Uno
2. Dos
3. Tres [Vaya a la pregunta 28]
¿Por qué decidió no ir a todos los eventos de actividad familiar? (Marque con un círculo todas las respuestas que correspondan).
1. No sabía de los otros eventos
2. Los eventos se ofrecían a horas que no eran convenientes para mí
3. No pensé que los eventos serían de utilidad
4. No me gusta ir a eventos de este tipo
5. Otra razón (especifique):
¿Qué tan útiles fueron los eventos de actividad familiar para ayudarlo(a) a usted a que haga que su niño(a) coma de manera más saludable? (Marque una respuesta con un círculo). [Vaya a la pregunta 30 después de contestar esta pregunta].
1. Muy útil
2. Útil
3. Algo útil
4. No muy útil
5. Nada útil
¿Por qué decidió no ir a ninguno de los eventos de actividad familiar? (Marque con un círculo todas las respuestas que correspondan).
1. No sabía de los eventos
2. Los eventos se ofrecían a horas que no eran convenientes para mí
3. No pensé que los eventos serían de utilidad
4. No me ir a eventos de este tipo
5. Otra razón (especifique):
Por favor, comparta cualquier comentario que tenga sobre los materiales, actividades y los eventos de actividad familiar.
Gracias por completar nuestra encuesta.
Por favor,
devuelva la encuesta en el sobre adjunto.
OMB No. 0584-NEW
Fecha de expiración: XX/XXXX
Ver la declaración OMB en la parte interior de la portada
¿Qué come su niño?
|
|
¡Gracias por participar en este importante estudio!
Por favor, complete y devuelva la encuesta en el sobre adjunto a más tardar la próxima semana. Si tiene alguna pregunta sobre el estudio ¿Qué come su niño?, por favor envíe un mensaje por correo electrónico a xxxx@rti.org o llame al número gratuito 1-800-xxx-xxxx.
Se calcula que el tiempo aproximado que le tomará a cada participante en dar esta información será de 15 minutos, incluyendo el tiempo para repasar las instrucciones, buscar las fuentes de información existentes, juntar y mantener los datos requeridos, así como completar y revisar la recopilación de datos.
Ninguna agencia está autorizada a realizar o patrocinar ninguna recopilación de datos o información sin presentar un número actual de control OMB válido, ni está obligada ninguna persona a participar en una recopilación de datos si no existe dicho número.
Envíe sus comentarios acerca de este cálculo de tiempo o cualquier otro aspecto relacionado con esta recolección de datos, incluyendo sugerencias para reducir el tiempo, a: U.S. Department of Agriculture, Food and Nutrition Services, Office of Research and Analysis, Room 1014, Alexandria, VA 22302. ATTN: PRA (0584-xxxx*). No envíe el cuestionario con sus respuestas a esta dirección.
Si tiene preguntas sobre sus derechos como participante en un estudio, puede comunicarse con la Oficina de RTI para la Protección de Participantes en Estudios al número gratuito 1-866-214-2043.
What
Does Your Child Eat? (¿Qué
come su niño?)
Mail
Questionnaire (Post-survey, Control Group)
Instrument for University of Nevada Impact Evaluation
Esta encuesta pregunta sobre lo que come su niño(a). Este estudio está patrocinado por el Servicio de Alimentos y Nutrición del Departamento de Agricultura de los Estados Unidos y lo realiza RTI International, una organización sin fines de lucro que realiza estudios sobre la salud. La encuesta tomará entre 15 y 20 minutos en completarse. Usted recibirá $15 dólares por completar la entrevista.
Todas sus respuestas a la encuesta se mantendrán privadas. Nosotros no compartiremos sus respuestas con nadie. Usted puede dejar de contestar cualquier pregunta que no desee contestar. Si tiene alguna pregunta, por favor llame a xxxx xxxx en RTI International al 1-800-xxx-xxxx.
Preguntas sobre la disponibilidad de ciertos alimentos en el hogar
1. ¿Estuvieron disponibles algunos de los siguientes alimentos en su hogar durante la semana pasada? Incluya alimentos frescos, congelados, enlatados y secos. (Marque con un círculo la respuesta Sí o No por cada alimento).
a. Plátanos |
Sí |
No |
b. Manzanas |
Sí |
No |
c. Uvas |
Sí |
No |
d. Mangos |
Sí |
No |
e. Kiwis |
Sí |
No |
f. Zanahorias |
Sí |
No |
g. Jícamas |
Sí |
No |
h. Papas fritas en bolsa, nachos u hojuelas de maíz ‘corn chips’ |
Sí |
No |
i. Galletas dulces ‘graham’ |
Sí |
No |
j. Queso en tiras |
Sí |
No |
k. Gaseosas o sodas regulares |
Sí |
No |
l. Gaseosas o sodas de dieta o de bajas calorías |
Sí |
No |
Preguntas sobre las frutas y vegetales que come su niño(a)
Para las siguientes preguntas, piense en lo que su niño(a) comió durante la semana pasada o en los últimos 7 días. No incluya el tiempo en la escuela o la guardería infantil.
2. ¿Cuántos días durante la semana pasada comió su niño(a) más de un tipo de fruta cada día? No incluya jugo de frutas. (Marque una respuesta con un círculo).
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
3. Durante la semana pasada, ¿cuántas tazas de fruta comió su niño(a) cada día? No incluya jugo de frutas. (Marque una respuesta con un círculo).
1. Ninguna |
|
||||||
2. 1/2 taza |
|||||||
3. 1 taza |
|||||||
4. 1 ½ tazas |
|||||||
5. 2 tazas |
Ninguna |
|
1 taza |
|
2 tazas |
|
3 tazas |
6. 2 ½ tazas |
|
|
|
|
|
||
7. 3 tazas o más |
|
||||||
4. ¿Cuántos días durante la semana pasada comió su niño(a) más de un tipo de vegetal cada día? No incluya jugo de vegetales. (Marque una respuesta con un círculo).
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
5. Durante la semana pasada, ¿cuántas tazas de vegetales comió su niño(a) cada día? No incluya jugo de vegetales. (Marque una respuesta con un círculo).
1. Ninguna |
|
||||||
2. 1/2 taza |
|||||||
3. 1 taza |
|||||||
4. 1 ½ tazas |
|||||||
5. 2 tazas |
Ninguna |
|
1 taza |
|
2 tazas |
|
3 tazas |
6. 2 ½ tazas |
|
|
|
|
|
||
7. 3 tazas o más |
|
||||||
6. Durante la semana pasada, ¿comió su niño(a) algún alimento o merienda o ‘snack’ que fue proporcionado por su escuela o guardería infantil? (Marque con un círculo todas las respuestas que correspondan).
1. Sí, en el desayuno
2. Sí, en el almuerzo
3. Sí, comió meriendas o ‘snacks’
4. No, no comió desayuno, almuerzo, ni meriendas o ‘snacks’ proporcionados por la escuela o guardería infantil.
7. ¿Está su niño(a) dispuesto a probar un nuevo tipo de fruta? (Marque una respuesta con un círculo).
1. No
2. Quizás
3. Sí
8. ¿Cuántos días durante la semana pasada le dio usted fruta a su niño(a) como merienda o ‘snack’? (Marque una respuesta con un círculo).
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
9. ¿Cuántos días durante la semana pasada le pidió su niño(a) o se sirvió él o ella por sí mismo(a) fruta como merienda o ‘snack’? (Marque una respuesta con un círculo).
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
10. ¿Cuántos días durante la semana pasada le dio a su niño(a) fruta en la cena? (Marque una respuesta con un círculo).
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
11. ¿Está su niño(a) dispuesto(a) a probar un nuevo tipo de vegetal? (Marque una respuesta con un círculo).
1. No
2. Quizás
3. Sí
12. ¿Cuántos días durante la semana pasada le dio vegetales a su niño(a) como merienda o ‘snack’? (Marque una respuesta con un círculo).
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
13. ¿Cuántos días durante la semana pasada le pidió su niño(a) o se sirvió él o ella por sí mismo(a) vegetales como merienda o ‘snack’? (Marque una respuesta con un círculo).
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
14. ¿Cuántos días durante la semana pasada le dio a su niño(a) vegetales en la cena? (Marque una respuesta con un círculo).
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
Preguntas sobre los hábitos alimenticios de su niño(a)
15. ¿Cuántos días durante la semana pasada hizo usted que su niño(a) comiera todo lo que estaba en su plato de comida? (Marque una respuesta con un círculo).
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
16. Durante el mes pasado, cuando ordenaba comida para su niño(a) en un restaurante de comida rápida, ¿con qué frecuencia pidió frutas o vegetales (por ejemplo, rebanadas de manzanas o palitos de zanahorias) en lugar de papas fritas? (Marque una respuesta con un círculo).
1. No comimos en restaurantes de comida rápida
2. Nunca
3. Rara vez
4. Algunas veces
5. La mayoría de veces
6. Casi siempre
17. Durante el mes pasado, cuando salía a comer a un restaurante de comida rápida, ¿con qué frecuencia pedía su niño(a) frutas o vegetales (por ejemplo, rebanadas de manzanas o palitos de zanahorias) en lugar de papas fritas? (Marque una respuesta con un círculo).
1. No comimos en restaurantes de comida rápida
2. Nunca
3. Rara vez
4. Algunas veces
5. La mayoría de veces
6. Casi siempre
18. ¿Qué tan de acuerdo o en desacuerdo está usted con la siguiente declaración? “Si mi niño(a) come de manera saludable, él o ella será más saludable cuando tenga más edad”. (Marque una respuesta con un círculo).
1. Muy de acuerdo
2. De acuerdo
3. En desacuerdo
4. Muy en desacuerdo
19. ¿Qué tan de acuerdo o en desacuerdo está usted con la siguiente declaración? “Yo soy un buen ejemplo para mi niño(a) al comer alimentos saludables”. (Marque una respuesta con un círculo).
1. Muy de acuerdo
2. De acuerdo
3. En desacuerdo
4. Muy en desacuerdo
Gracias por completar nuestra encuesta.
Por favor,
devuelva la encuesta en el sobre adjunto.
OMB No. 0584-NEW
Fecha de expiración: XX/XXXX
What
Does Your Child Eat? ¿Qué
come su niño?
Telephone
Questionnaire for Nonrespondents
(Post-survey, Intervention and Control Groups)
Instrument for University of Nevada Impact Evaluation
Para comenzar esta encuesta, le voy a leer una lista de alimentos. Por cada uno de ellos, dígame por favor si estuvo disponible ese alimento en su hogar durante la semana pasada. Por favor, incluya alimentos frescos, congelados, enlatados y secos. Responda sí o no por cada alimento. El primer alimento es…
a. Plátanos |
Sí |
NO |
DK |
RF |
b. Manzanas |
Sí |
NO |
DK |
RF |
c. Uvas |
Sí |
NO |
DK |
RF |
d. Mangos |
Sí |
NO |
DK |
RF |
e. Kiwis |
Sí |
NO |
DK |
RF |
f. Zanahorias |
Sí |
NO |
DK |
RF |
g. Jícamas |
Sí |
NO |
DK |
RF |
h. Papas fritas en bolsa, nachos u hojuelas de maíz ‘corn chips’ |
Sí |
NO |
DK |
RF |
i. Galletas dulces ‘graham’ |
Sí |
NO |
DK |
RF |
j. Queso en tiras |
Sí |
NO |
DK |
RF |
k. Gaseosas o sodas regulares |
Sí |
NO |
DK |
RF |
l. Gaseosas o sodas de dieta o de bajas calorías |
Sí |
NO |
DK |
RF |
Para las siguientes preguntas, piense sobre lo que su niño(a) comió durante la semana pasada o en los últimos 7 días. No incluya el tiempo en la escuela o la guardería infantil.
¿Cuántos días durante la semana pasada comió su niño(a) más de un tipo de fruta cada día? No incluya jugo de frutas. ¿Diría usted… SELECT ONE.
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
-4. DON’T KNOW
-7. REFUSAL
Durante la semana pasada, ¿cuántas tazas de fruta comió su niño(a) cada día? No incluya jugo de frutas. ¿Diría que su niño(a) comió…? GIVE RESPONDENT PICTURE OF CUPS. SELECT ONE.
1. Ninguna fruta
2. ½ taza
3. 1 taza
4. 1 ½ tazas
5. 2 tazas
6. 2 ½ tazas
7. 3 tazas o más
-4. DON’T KNOW
-7. REFUSAL
¿Cuántos días durante la semana pasada comió su niño(a) más de un tipo de vegetal cada día? No incluya jugo de vegetales. ¿Diría usted…? SELECT ONE.
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
-4. DON’T KNOW
-7. REFUSAL
Durante la semana pasada, ¿cuántas tazas de vegetales comió su niño(a) cada día? No incluya jugo de vegetales. ¿Diría usted que su niño(a) comió…? SELECT ONE.
1. Ningún vegetal
2. ½ taza
3. 1 taza
4. 1 ½ tazas
5. 2 tazas
6. 2 ½ tazas
7. 3 tazas o más
-4. DON’T KNOW
-7. REFUSAL
Durante la semana pasada, ¿comió su niño(a) algún alimento o merienda o ‘snack’ que fue proporcionado en su escuela o guardería infantil? ¿Diría usted que…? SELECT ALL THAT APPLY.
1. Sí, en el desayuno
2. Sí, en el almuerzo
3. Sí, comió meriendas o ‘snacks’
4. No, no comió en el desayuno, almuerzo, ni meriendas o ‘snacks’ proporcionados por la escuela o guardería infantil
-4. DON’T KNOW
-7. REFUSAL
¿Está su niño(a) dispuesto(a) a probar un nuevo tipo de fruta? ¿Diría usted…? SELECT ONE.
1. No
2. Quizás
3. Sí
-4. DON’T KNOW
-7. REFUSAL
¿Cuántos días durante la semana pasada le dio usted fruta a su niño(a) como merienda o ‘snack’? ¿Diría usted…? SELECT ONE.
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
-4. DON’T KNOW
-7. REFUSAL
¿Cuántos días durante la semana pasada le pidió su niño(a) o se sirvió él o ella por sí mismo(a) fruta como merienda o ‘snack’? ¿Diría usted…? SELECT ONE.
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
-4. DON’T KNOW
-7. REFUSAL
¿Cuántos días durante la semana pasada le dio a su niño(a) fruta en la cena? ¿Diría usted…? SELECT ONE.
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
-4. DON’T KNOW
-7. REFUSAL
¿Estaría su niño(a) dispuesto(a) a probar un nuevo tipo de vegetal? ¿Diría usted…? SELECT ONE.
1. No
2. Quizás
3. Sí
-4. DON’T KNOW
-7. REFUSAL
¿Cuántos días durante la semana pasada le dio vegetales a su niño(a) como merienda o ‘snack’? ¿Diría usted…? SELECT ONE.
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
-4. DON’T KNOW
-7. REFUSAL
¿Cuántos días durante la semana pasada le pidió su niño(a) o se sirvió él o ella por sí mismo(a) vegetales como merienda o ‘snack’? ¿Diría usted…? SELECT ONE.
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
-4. DON’T KNOW
-7. REFUSAL
¿Cuántos días durante la semana pasada le dio a su niño(a) vegetales en la cena? ¿Diría usted…? SELECT ONE.
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
-4. DON’T KNOW
-7. REFUSAL
¿Cuántos días durante la semana pasada hizo usted que su niño(a) comiera todo lo que estaba en su plato de comida? ¿Diría usted…? SELECT ONE.
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
-4. DON’T KNOW
-7. REFUSAL
Durante el mes pasado, al ordenar comida para su niño(a) en un restaurante de comida rápida, ¿con qué frecuencia pidió frutas o vegetales (por ejemplo, rebanadas de manzanas o palitos de zanahorias) en lugar de papas fritas? ¿Diría usted…? SELECT ONE.
1. NO COMIÓ EN RESTAURANTES DE COMIDA RÁPIDA [Go to Question 18.]
2. Nunca
3. Rara vez
4. Algunas veces
5. La mayoría de veces
6. Casi siempre
-4. DON’T KNOW
-7. REFUSAL
Durante el mes pasado, al salir a comer a un restaurante de comida rápida, ¿con qué frecuencia pedía su niño(a) frutas o vegetales (por ejemplo, rebanadas de manzanas o palitos de zanahorias) en lugar de papas fritas? ¿Diría usted…? SELECT ONE.
1. NO COMIÓ EN RESTAURANTES DE COMIDA RÁPIDA
2. Nunca
3. Rara vez
4. Algunas veces
5. La mayoría de veces
6. Casi siempre
-4. DON’T KNOW
-7. REFUSAL
Para las siguientes dos preguntas, le voy a leer una declaración. Por cada declaración, dígame por favor si usted está muy de acuerdo, de acuerdo, en desacuerdo o muy en desacuerdo con la declaración.
¿Qué tan de acuerdo o en desacuerdo está usted con la siguiente declaración? “Si mi niño(a) come de manera saludable, él o ella será más saludable cuando tenga más edad”. ¿Diría usted…? SELECT ONE.
1. Muy de acuerdo
2. De acuerdo
3. En desacuerdo
4. Muy en desacuerdo
-4. DON’T KNOW
-7. REFUSAL
¿Qué tan de acuerdo o en desacuerdo está usted con la siguiente declaración? “Yo soy un buen ejemplo para mi niño(a) al comer alimentos saludables”. ¿Diría usted…? SELECT ONE.
1. Muy de acuerdo
2. De acuerdo
3. En desacuerdo
4. Muy en desacuerdo
-4. DON’T KNOW
-7. REFUSAL
[IF CONTROL GROUP THEN GO TO Q31]
El último grupo de preguntas son acerca de los materiales que recibió su niño(a) en la escuela y que puede haber llevado al hogar.
Su niño recibió unas “Tarjetas inteligentes de meriendas o snacks”. Cada tarjeta tiene una foto de una merienda o ‘snack’ saludable y el tamaño de la porción. ¿Usó usted o alguien más en su hogar las “Tarjetas inteligentes de meriendas o snacks” con su niño(a) para seleccionar una merienda o ‘snack’ saludable? SELECT ONE.
1. YES
2. NO
3. DID NOT GET “TARJETAS INTELIGENTES DE MERIENDAS O SNACKS”
-4. DON’T KNOW
-7. REFUSAL
Su niño(a) recibió una hoja de tarea que se llama “Busquemos alimentos saludables”. La hoja de tarea pedía que usted y su niño(a) encuentren alimentos específicos en el supermercado y los marquen en la lista. ¿Hizo usted o alguien más en su hogar la tarea con su niño(a)? SELECT ONE.
1. YES
2. NO
3. DID NOT GET “HOJA DE TAREA”
-4. DON’T KNOW
-7. REFUSAL
Su niño(a) recibió un “Medidor de hambre” que ayuda a su niño(a) a saber cuando él o ella tiene hambre o está satisfecho(a). ¿Realizó usted o alguien en su hogar la actividad del “Medidor de hambre” con su niño(a)? SELECT ONE.
1. YES
2. NO
3. DID NOT GET “MEDIDOR DE HAMBRE”
-4. DON’T KNOW
-7. REFUSAL
¿Qué tan fácil fue entender los materiales y las actividades que se enviaron al hogar con su niño(a)? SELECT ONE.
1. Muy fácil
2. Fácil
3. Algo fácil
4. No muy fácil
5. Nada fácil
6. NO LEÍ LOS MATERIALES O NO HICE LAS ACTIVIDADES QUE SE ENVIARON AL HOGAR CON MI NIÑO(A) [Go to Question 25.]
-4. DON’T KNOW
-7. REFUSAL
¿Qué tan útiles fueron los materiales y las actividades para ayudarlo(a) a usted a que haga que su niño(a) coma de manera más saludable? SELECT ONE.
1. Muy útil
2. Útil
3. Algo útil
4. No muy útil
5. Nada útil
6. NO LEÍ LOS MATERIALES O NO HICE LAS ACTIVIDADES QUE SE ENVIARON AL HOGAR CON MI NIÑO(A)
-4. DON’T KNOW
-7. REFUSAL
El centro Head Start de su niño(a) tuvo un evento de actividad familiar cada mes durante 3 meses. Estos eventos trataban sobre cómo estar saludables y se ofrecían alimentos para probar y hubieron bailes. ¿Asistió usted o alguien más en su hogar a alguno de los eventos de actividad familiar? SELECT ONE.
1. YES
2. NO [Go to Question 29]
-4. DON’T KNOW [Go to Question 29]
-7. REFUSAL [Go to Question 29]
¿A cuántos eventos de actividad familiar asistió usted o alguien más en su hogar? SELECT ONE.
1. Uno
2. Dos
3. Tres [Go to Question 28]
-4. DON’T KNOW [Go to Question 28]
-7. REFUSAL [Go to Question 28]
¿Por qué decidió no ir a todos los eventos de actividad familiar? ¿Fue porque…? SELECT ALL THAT APPLY.
1. No sabía de los otros eventos
2. Los eventos se ofrecían a horas que no eran convenientes para usted
3. No pensó que los eventos serían de utilidad
4. No le gusta ir a eventos de este tipo
5. Alguna otra razón (SPECIFY):
-4. DON’T KNOW
-7. REFUSAL
¿Qué tan útiles fueron los eventos de actividad familiar para ayudarlo(a) a usted a que haga que su niño(a) coma de manera más saludable? ¿Diría usted que…? SELECT ONE.
1. Muy útil
2. Útil
3. Algo útil
4. No muy útil
5. Nada útil
-4. DON’T KNOW
-7. REFUSAL
[ALL GO TO Q30.]
¿Por qué decidió no ir a ninguno de los eventos de actividad familiar? ¿Fue porque…? SELECT ALL THAT APPLY.
1. No sabía de los otros eventos
2. Los eventos se ofrecían a horas que no eran convenientes para usted
3. No pensó que los eventos serían de utilidad
4. No le gusta ir a eventos de este tipo
5. Alguna otra razón (SPECIFY):
-4. DON’T KNOW
-7. REFUSAL
Por favor, comparta cualquier comentario que tenga sobre los materiales, actividades y los eventos de actividad familiar.
31. Estas son todas las preguntas. Gracias por completar nuestra encuesta. Antes de despedirme, me gustaría confirmar que tengo su nombre y dirección correctos para enviarle el incentivo en efectivo como agradecimiento por haber completado esta encuesta. Tengo aquí que su nombre es [RESPONDENT NAME] y se escribe _____________________. ¿Es correcto?
1. YES
2. CORRECT NAME [PROGRAMMER –SET UP TO ENTER CORRECTIONS]
-7. REFUSAL
32. Tengo aquí que su dirección es [RESPONDENT STREET ADDRESS] ¿Es correcto?
1. YES
2. NO [PROGRAMMER –SET UP TO ENTER CORRECT ADDRESS]
-7. REFUSAL
33. Tengo aquí que la ciudad, estado y código postal donde vive es [RESPONDENT CITY, STATE, ZIP CODE] ¿Es correcto?
1. YES
2. CORRECT CITY
3. CORRECT STATE
4. CORRECT ZIPCODE [PROGRAMMER –SET UP TO ENTER ALLOW FOR GENERATION OF ADDRESS LABELS FOR INCENTIVE LETTERS]
-7. REFUSAL
Gracias nuevamente. Qué pase un buen día/una buena noche.
Impact Evaluation Instrument for NYSDOH
For the NYSDOH project, we will survey parents/caregivers of preschool children at pre- and post-intervention using a mail/telephone survey approach. We provide the following four versions of the instrument:
mail questionnaire (pre-survey - intervention and control groups),
mail questionnaire (post-survey - intervention group),
mail questionnaire (post-survey - control group), and
telephone questionnaire for nonrespondents to mail survey (pre- and post-surveys - intervention and control groups).
English and Spanish versions are provided. The Spanish translation takes into consideration the Puerto Rico population in New York.
English Version
OMB No. 0584-NEW
Expiration date: XX/XXXX
See OMB statement on inside cover
What Does Your Child Eat?
|
|
Thank you for taking part in this important study!
Please fill out and return the survey in the enclosed envelope within the next week.
If you have any questions about the What Does Your Child Eat? study, please send an e-mail to xxxx@rti.org or call toll-free at 1-800-xxx-xxxx.
Public reporting burden for this collection of information is estimated to average 15 minutes per response, including the time for reviewing instructions, searching existing data sources, gathering and maintaining the data needed, and completing and reviewing the collection of information.
An agency may not conduct or sponsor, and a person is not required to respond to, a collection of information unless it displays a currently valid OMB control number.
Send comments regarding this burden estimate or any other aspect of this collection of information, including suggestions for reducing this burden, to: U.S. Department of Agriculture, Food and Nutrition Services, Office of Research and Analysis, Room 1014, Alexandria, VA 22302 ATTN: PRA (0584-xxxx*). Do not return the completed form to this address.
If you have questions regarding your rights as a research participant, you may contact RTI’s Office of Research Protection toll-free at 866-214-2043.
What
Does Your Child Eat?
Mail Questionnaire (Pre-survey,
Intervention and Control Groups)
Instrument for NYSDOH Impact Evaluation
This survey asks about what your child eats. This study is being sponsored by the U.S. Department of Agriculture’s Food & Nutrition Service and conducted by RTI International, a non-profit research organization. The survey will take about 10 to 15 minutes to complete. You will receive $10 for completing this survey and $15 for completing a second survey that we will mail you in about 2 months.
All of your answers to the survey will be kept private. We will not share your answers with anyone. You may skip any questions you do not want to answer. If you have any questions, please call xxx xxxx at RTI International at 1-800-xxx-xxxx.
Questions on Whether Certain Foods Are Available at Home
Were any of the following foods available in your home during the past week? Include fresh, frozen, canned, and dried foods. (Circle yes or no for each food.)
a. Bananas |
Yes |
No |
b. Apples |
Yes |
No |
c. Grapes |
Yes |
No |
d. Melons (for example, cantaloupe, honeydew, or watermelon) |
Yes |
No |
e. Strawberries |
Yes |
No |
f. Carrots |
Yes |
No |
g. Potato chips, nacho chips, or corn chips |
Yes |
No |
h. Regular soft drinks or sodas |
Yes |
No |
i. Diet or low calorie soft drinks or sodas |
Yes |
No |
j. Regular whole or 2% milk |
Yes |
No |
k. 1% or skim milk |
Yes |
No |
Questions on the Fruits and Vegetables Your Child Eats
For the next questions think about what your child ate during the past week, or the past 7 days. Do not include school or day care time.
How many days during the past week did your child eat more than one kind of fruit each day? Do not include fruit juice. (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
During the past week, how many cups of fruit did your child eat each day? Do not include fruit juice. (Circle one.)
1. None
2. 1/2 cup
3. 1 cup
4. 1 ½ cups
5. 2 cups
None
1 cup
2 cups
3 cups
6. 2 ½ cups
7. 3 cups or more
How many days during the past week did your child eat more than one kind of vegetable each day? Do not include vegetable juice. (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
During the past week, how many cups of vegetables did your child eat each day? Do not include vegetable juice. (Circle one.)
1. None
2. 1/2 cup
3. 1 cup
4. 1 ½ cups
5. 2 cups
None
1 cup
2 cups
3 cups
6. 2 ½ cups
7. 3 cups or more
During the past week, did your child eat any meals or snacks that were provided by his or her school or day care? (Circle all that apply.)
1. Yes, breakfast
2. Yes, lunch
3. Yes, snacks
4. No, did not eat breakfast, lunch, or snacks provided by school or day care
Is your child willing to try a new kind of fruit? (Circle one.)
1. No
2. Maybe
3. Yes
How many days during the past week did you give your child fruit as a snack? (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
How many days during the past week did your child ask or help himself or herself to fruit for a snack? (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
How many days during the past week did you give your child fruit at dinner? (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
Is your child willing to try a new kind of vegetable? (Circle one.)
1. No
2. Maybe
3. Yes
How many days during the past week did you give your child a vegetable as a snack? (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
How many days during the past week did your child ask or help himself or herself to vegetables for a snack? (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
How many days during the past week did you give your child a vegetable at dinner? (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
Questions on the Dairy Products Your Child Eats
Did your child drink milk or use milk on his or her cereal at home during the past week? (Circle one.)
1. Yes
2. No [Go to Question 17]
What kind of milk did your child drink or use on his or her cereal at home during the past week? (Circle one.)
1. Regular whole milk
2. 2% milk
3. 1% milk
4. Skim or fat-free milk
5. Other type of milk (for example, soy or rice milk)
How many days during the past week did your child eat low-fat or fat-free yogurt at home? (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
How many days during the past week did your child eat regular-fat yogurt at home? (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
Questions on Your Child’s Eating Habits
How many days during the past week did your child help you make or cook a meal? For example, did your child wash fruits or vegetables? (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
How many days during the past week did you make your child eat everything on his or her dinner plate? (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
How much do you agree or disagree with the following statement? “If my child eats healthy, he or she will be healthier when he or she gets older.” (Circle one.)
1. Strongly agree
2. Agree
3. Disagree
4. Strongly disagree
How much do you agree or disagree with the following statement? “I am a good role model for my child by eating healthy foods.” (Circle one.)
1. Strongly agree
2. Agree
3. Disagree
4. Strongly disagree
Questions about You and Your Household
During the past year, how often did you run out of food before the end of the month? (Circle one.)
1. Did not run out of food
2. Seldom
3. Sometimes
4. Most of the time
5. Almost always
How many people under 18 years of age live in your household?
____
Including yourself, how many people 18 years of age or older live in your household?
____
Which of the following categories best describes your age? (Circle one.)
1. 18 to 24
2. 25 to 34
3. 35 to 44
4. 45 to 54
5. 55 to 64
6. 65 to 74
7. Over 74
What is your gender? (Circle one.)
1. Male
2. Female
Are you Hispanic or Latino? (Circle one.)
1. Yes
2. No
What is your race? (Circle all that apply.)
1. American Indian or Alaska Native
2. Asian
3. Black or African American
4. Native Hawaiian or other Pacific Islander
5. White
Does your family speak English at home? (Circle one.)
1. We speak English all of the time at home.
2. We speak English some of the time at home and speak another language some of the time.
3. We never speak English at home. We speak another language.
Thank
you for completing our survey.
Please return the survey in the
enclosed envelope.
OMB No. 0584-NEW
Expiration date: XX/XXXX
See OMB statement on inside cover
What Does Your Child Eat?
|
|
Thank you for taking part in this important study!
Please fill out and return the survey in the enclosed envelope within the next week.
If you have any questions about the What Does Your Child Eat? study, please send an e-mail to xxxx@rti.org or call toll-free at 1-800-xxx-xxxx.
Public reporting burden for this collection of information is estimated to average 15 minutes per response, including the time for reviewing instructions, searching existing data sources, gathering and maintaining the data needed, and completing and reviewing the collection of information.
An agency may not conduct or sponsor, and a person is not required to respond to, a collection of information unless it displays a currently valid OMB control number.
Send comments regarding this burden estimate or any other aspect of this collection of information, including suggestions for reducing this burden, to: U.S. Department of Agriculture, Food and Nutrition Services, Office of Research and Analysis, Room 1014, Alexandria, VA 22302 ATTN: PRA (0584-xxxx*). Do not return the completed form to this address.
If you have questions regarding your rights as a research participant, you may contact RTI’s Office of Research Protection toll-free at 866-214-2043.
What
Does Your Child Eat?
Mail Questionnaire (Post-survey,
Intervention Group)
Instrument for NYSDOH Impact Evaluation
This survey asks about what your child eats. This study is being sponsored by the U.S. Department of Agriculture’s Food & Nutrition Service and conducted by RTI International, a non-profit research organization. The survey will take about 10 to 15 minutes to complete. You will receive $15 for completing this survey.
All of your answers to the survey will be kept private. We will not share your answers with anyone. You may skip any questions you do not want to answer. If you have any questions, please call xxx xxxx at RTI International at 1-800-xxx-xxxx.
Questions on Whether Certain Foods Are Available at Home
Were any of the following foods available in your home during the past week? Include fresh, frozen, canned, and dried foods. (Circle yes or no for each food.)
a. Bananas |
Yes |
No |
b. Apples |
Yes |
No |
c. Grapes |
Yes |
No |
d. Melons (for example, cantaloupe, honeydew, or watermelon) |
Yes |
No |
e. Strawberries |
Yes |
No |
f. Carrots |
Yes |
No |
g. Potato chips, nacho chips, or corn chips |
Yes |
No |
h. Regular soft drinks or sodas |
Yes |
No |
i. Diet or low calorie soft drinks or sodas |
Yes |
No |
j. Regular whole or 2% milk |
Yes |
No |
k. 1% or skim milk |
Yes |
No |
Questions on the Fruits and Vegetables Your Child Eats
For the next questions think about what your child ate during the past week, or the past 7 days. Do not include school or day care time.
How many days during the past week did your child eat more than one kind of fruit each day? Do not include fruit juice. (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
During the past week, how many cups of fruit did your child eat each day? Do not include fruit juice. (Circle one.)
1. None
2. 1/2 cup
3. 1 cup
4. 1 ½ cups
5. 2 cups
None
1 cup
2 cups
3 cups
6. 2 ½ cups
7. 3 cups or more
How many days during the past week did your child eat more than one kind of vegetable each day? Do not include vegetable juice. (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
During the past week, how many cups of vegetables did your child eat each day? Do not include vegetable juice. (Circle one.)
1. None
2. 1/2 cup
3. 1 cup
4. 1 ½ cups
5. 2 cups
None
1 cup
2 cups
3 cups
6. 2 ½ cups
7. 3 cups or more
During the past week, did your child eat any meals or snacks that were provided by his or her school or day care? (Circle all that apply.)
1. Yes, breakfast
2. Yes, lunch
3. Yes, snacks
4. No, did not eat breakfast, lunch, or snacks provided by school or day care
Is your child willing to try a new kind of fruit? (Circle one.)
1. No
2. Maybe
3. Yes
How many days during the past week did you give your child fruit as a snack? (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
How many days during the past week did your child ask or help himself or herself to fruit for a snack? (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
How many days during the past week did you give your child fruit at dinner? (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
Is your child willing to try a new kind of vegetable? (Circle one.)
1. No
2. Maybe
3. Yes
How many days during the past week did you give your child a vegetable as a snack? (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
How many days during the past week did your child ask or help himself or herself to vegetables for a snack? (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
How many days during the past week did you give your child a vegetable at dinner? (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
Questions on the Dairy Products Your Child Eats
Did your child drink milk or use milk on his or her cereal at home during the past week? (Circle one.)
1. Yes
2. No [Go to Question 17]
What kind of milk did your child drink or use on his or her cereal at home during the past week? (Circle one.)
1. Regular whole milk
2. 2% milk
3. 1% milk
4. Skim or fat-free milk
5. Other type of milk (for example, soy or rice milk)
How many days during the past week did your child eat low-fat or fat-free yogurt at home? (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
How many days during the past week did your child eat regular-fat yogurt at home? (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
Questions on Your Child’s Eating Habits
How many days during the past week did your child help you make or cook a meal? For example, did your child wash fruits or vegetables? (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
How many days during the past week did you make your child eat everything on his or her dinner plate? (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
How much do you agree or disagree with the following statement? “If my child eats healthy, he or she will be healthier when he or she gets older.” (Circle one.)
1. Strongly agree
2. Agree
3. Disagree
4. Strongly disagree
How much do you agree or disagree with the following statement? “I am a good role model for my child by eating healthy foods.” (Circle one.)
1. Strongly agree
2. Agree
3. Disagree
4. Strongly disagree
Questions on Materials Your Child Got at Child Care
Your child’s teacher sent home a handout about eating vegetables. Did you or someone else in your household do the handout with your child? (Circle one.)
1. Yes
2. No
3. Did not get handout
Your child’s teacher sent home a handout about eating fruit. Did you or someone else in your household do the handout with your child? (Circle one.)
1. Yes
2. No
3. Did not get handout
Your child’s teacher sent home a handout about drinking and eating low-fat dairy products. Did you or someone else in your household do the handout with your child? (Circle one.)
1. Yes
2. No
3. Did not get handout
Your child’s teacher sent home several “Parent Pages” with tips on healthy eating and healthy recipes. Did you or someone else in your household read the “Parent Pages”? (Circle one.)
1. Yes, all or most of them
2. Yes, some of them
3. No
4. Did not get the “Parent Pages”
How easy was it to understand the handouts, the “Parent Pages,” and other materials sent home with your child? (Circle one.)
1. Very easy
2. Easy
3. Somewhat easy
4. Not very easy
5. Not at all easy
6. Did not get or read the handouts, the “Parent Pages,” and other materials
How useful were the handouts, the “Parent Pages,” and other materials sent home with your child in helping you to get your child to eat healthier? (Circle one.)
1. Very useful
2. Useful
3. Somewhat useful
4. Not very useful
5. Not at all useful
6. Did not get or read the handouts, the “Parent Pages” and other materials
During the past two months, six classes for parents were conducted by a registered dietitian at your child care facility on why it is important to eat healthy and be physically active. Did you or someone else in your household go to any of these classes? (Circle one.)
1. Yes
2. No [Go to Question 33]
Of these six classes on healthy eating and physical activity, how many did you or someone else in your household attend? (Circle one.)
1. One
2. Two
3. Three
4. Four
5. Five
6. Six [Go to Question 32]
Why did you decide not to go to all of the classes? (Circle all that apply.)
1. Did not know about the other classes
2. The classes were offered at times that did not work for me
3. Did not think the classes would be useful
4. Do not like to go to classes like this
5. Other reason (specify):
How useful were the classes in helping you to get your child to eat healthier? (Circle one.) [Go to Question 34 after answering this question.]
1. Very useful
2. Useful
3. Somewhat useful
4. Not very useful
5. Not at all useful
Why did you decide not to go to any of the classes? (Circle all that apply.)
1. Did not know about the classes
2. The classes were offered at times that did work for me
3. Did not think the classes would be useful
4. Do not like to go to classes like this
5. Other reason (specify):
Please share any comments about the handouts, “Parent Pages,” and classes.
Thank
you for completing our survey.
Please return the survey in the
enclosed envelope.
OMB No. 0584-NEW
Expiration date: XX/XXXX
See OMB statement on inside cover
What Does Your Child Eat?
|
|
Thank you for taking part in this important study!
Please fill out and return the survey in the enclosed envelope within the next week.
If you have any questions about the What Does Your Child Eat? study, please send an e-mail to xxxx@rti.org or call toll-free at 1-800-xxx-xxxx.
Public reporting burden for this collection of information is estimated to average 15 minutes per response, including the time for reviewing instructions, searching existing data sources, gathering and maintaining the data needed, and completing and reviewing the collection of information.
An agency may not conduct or sponsor, and a person is not required to respond to, a collection of information unless it displays a currently valid OMB control number.
Send comments regarding this burden estimate or any other aspect of this collection of information, including suggestions for reducing this burden, to: U.S. Department of Agriculture, Food and Nutrition Services, Office of Research and Analysis, Room 1014, Alexandria, VA 22302 ATTN: PRA (0584-xxxx*). Do not return the completed form to this address.
If you have questions regarding your rights as a research participant, you may contact RTI’s Office of Research Protection toll-free at 866-214-2043.
What
Does Your Child Eat?
Mail Questionnaire (Post-survey, Control
Group)
Instrument for NYSDOH Impact Evaluation
This survey asks about what your child eats. This study is being sponsored by the U.S. Department of Agriculture’s Food & Nutrition Service and conducted by RTI International, a non-profit research organization. The survey will take about 10 to 15 minutes to complete. You will receive $15 for completing this survey.
All of your answers to the survey will be kept private. We will not share your answers with anyone. You may skip any questions you do not want to answer. If you have any questions, please call xxx xxxx at RTI International at 1-800-xxx-xxxx.
Questions on Whether Certain Foods Are Available at Home
Were any of the following foods available in your home during the past week? Include fresh, frozen, canned, and dried foods. (Circle yes or no for each food.)
a. Bananas |
Yes |
No |
b. Apples |
Yes |
No |
c. Grapes |
Yes |
No |
d. Melons (for example, cantaloupe, honeydew, or watermelon) |
Yes |
No |
e. Strawberries |
Yes |
No |
f. Carrots |
Yes |
No |
g. Potato chips, nacho chips, or corn chips |
Yes |
No |
h. Regular soft drinks or sodas |
Yes |
No |
i. Diet or low calorie soft drinks or sodas |
Yes |
No |
j. Regular whole or 2% milk |
Yes |
No |
k. 1% or skim milk |
Yes |
No |
Questions on the Fruits and Vegetables Your Child Eats
For the next questions think about what your child ate during the past week, or the past 7 days. Do not include school or day care time.
How many days during the past week did your child eat more than one kind of fruit each day? Do not include fruit juice. (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
During the past week, how many cups of fruit did your child eat each day? Do not include fruit juice. (Circle one.)
1. None
2. 1/2 cup
3. 1 cup
4. 1 ½ cups
5. 2 cups
None
1 cup
2 cups
3 cups
6. 2 ½ cups
7. 3 cups or more
How many days during the past week did your child eat more than one kind of vegetable each day? Do not include vegetable juice. (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
During the past week, how many cups of vegetables did your child eat each day? Do not include vegetable juice. (Circle one.)
1. None
2. 1/2 cup
3. 1 cup
4. 1 ½ cups
5. 2 cups
None
1 cup
2 cups
3 cups
6. 2 ½ cups
7. 3 cups or more
During the past week, did your child eat any meals or snacks that were provided by his or her school or day care? (Circle all that apply.)
1. Yes, breakfast
2. Yes, lunch
3. Yes, snacks
4. No, did not eat breakfast, lunch, or snacks provided by school or day care
Is your child willing to try a new kind of fruit? (Circle one.)
1. No
2. Maybe
3. Yes
How many days during the past week you give your child fruit as a snack? (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
How many days during the past week did your child ask or help himself or herself to fruit for a snack? (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
How many days during the past week did you give your child fruit at dinner? (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
Is your child willing to try a new kind of vegetable? (Circle one.)
1. No
2. Maybe
3. Yes
How many days during the past week did you give your child a vegetable as a snack? (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
How many days during the past week did your child ask or help himself or herself to vegetables for a snack? (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
How many days during the past week did you give your child a vegetable at dinner? (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
Questions on the Dairy Products Your Child Eats
Did your child drink milk or use milk on his or her cereal at home during the past week? (Circle one.)
1. Yes
2. No [Go to Question 17]
What kind of milk did your child drink or use on his or her cereal at home during the past week? (Circle one.)
1. Regular whole milk
2. 2% milk
3. 1% milk
4. Skim or fat-free milk
5. Other type of milk (for example, soy or rice milk)
How many days during the past week did your child eat low-fat or fat-free yogurt at home? (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
How many days during the past week did your child eat regular-fat yogurt at home? (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
Questions on Your Child’s Eating Habits
How many days during the past week did your child help you make or cook a meal? For example, did your child wash fruits or vegetables? (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
How many days during the past week did you make your child eat everything on his or her dinner plate? (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
How much do you agree or disagree with the following statement? “If my child eats healthy, he or she will be healthier when he or she gets older.” (Circle one.)
1. Strongly agree
2. Agree
3. Disagree
4. Strongly disagree
How much do you agree or disagree with the following statement? “I am a good role model for my child by eating healthy foods.” (Circle one.)
1. Strongly agree
2. Agree
3. Disagree
4. Strongly disagree
Thank
you for completing our survey.
Please return the survey in the
enclosed envelope.
OMB No. 0584-NEW
Expiration date: XX/XXXX
What
Does Your Child Eat?
Telephone Questionnaire for Nonrespondents
(Pre- and Post-surveys, Intervention and Control Groups)
Instrument for NYSDOH Impact Evaluation
To begin the survey, I’m going to read a list of foods. For each food, please tell me if it was available in your home during the past week? Please include fresh, frozen, canned, and dried foods. Answer yes or no for each food. The first food is…
a. Bananas |
Yes |
No |
DK |
RF |
b. Apples |
Yes |
No |
DK |
RF |
c. Grapes |
Yes |
No |
DK |
RF |
d. Melons (for example, cantaloupe, honeydew, or watermelon) |
Yes |
No |
DK |
RF |
e. Strawberries |
Yes |
No |
DK |
RF |
f. Carrots |
Yes |
No |
DK |
RF |
g. Potato chips, nacho chips, or corn chips |
Yes |
No |
DK |
RF |
h. Regular soft drinks or sodas |
Yes |
No |
DK |
RF |
i. Diet or low calorie soft drinks or sodas |
Yes |
No |
DK |
RF |
j. Regular whole or 2% milk |
Yes |
No |
DK |
RF |
k. 1% or skim milk |
Yes |
No |
DK |
RF |
For the next questions think about what your child ate during the past week, or the past 7 days. Do not include school or day care time.
How many days during the past week did your child eat more than one kind of fruit each day? Do not include fruit juice. Would you say…? SELECT ONE.
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
-4. DON’T KNOW
-7. REFUSAL
During the past week, how many cups of fruit did your child eat each day? Do not include fruit juice. Would you say your child had…? SELECT ONE.
1. No fruit
2. ½ cup
3. 1 cup
4. 1 ½ cups
5. 2 cups
6. 2 ½ cups
7. 3 cups or more
-4. DON’T KNOW
-7. REFUSAL
How many days during the past week did your child eat more than one kind of vegetable each day? Do not include vegetable juice. Would you say…? SELECT ONE.
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
-4. DON’T KNOW
-7. REFUSAL
During the past week, how many cups of vegetables did your child eat each day? Do not include vegetable juice. Would you say your child had…? SELECT ONE.
1. No vegetables
2. ½ cup
3. 1 cup
4. 1 ½ cups
5. 2 cups
6. 2 ½ cups
7. 3 cups or more
-4. DON’T KNOW
-7. REFUSAL
During the past week, did your child eat any meals or snacks that were provided by his or her school or day care? Would you say…? SELECT ALL THAT APPLY.
1. Yes, breakfast
2. Yes, lunch
3. Yes, snacks
4. No, did not eat breakfast, lunch, or snacks provided by school or day care
-4. DON’T KNOW
-7. REFUSAL
Is your child willing to try a new kind of fruit? Would you say…? SELECT ONE.
1. No
2. Maybe
3. Yes
-4. DON’T KNOW
-7. REFUSAL
How many days during the past week did you give your child fruit as a snack? Would you say…? SELECT ONE.
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
-4. DON’T KNOW
-7. REFUSAL
How many days during the past week did your child ask or help himself or herself to fruit for a snack? Would you say…? SELECT ONE.
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
-4. DON’T KNOW
-7. REFUSAL
How many days during the past week did you give your child fruit at dinner? Would you say…? SELECT ONE.
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
-4. DON’T KNOW
-7. REFUSAL
Is your child willing to try a new kind of vegetable? Would you say…? SELECT ONE.
1. No
2. Maybe
3. Yes
-4. DON’T KNOW
-7. REFUSAL
How many days during the past week did you give your child a vegetable as a snack? Would you say…? SELECT ONE.
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
-4. DON’T KNOW
-7. REFUSAL
How many days during the past week did your child ask or help himself or herself to vegetables for a snack? Would you say…? SELECT ONE.
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
-4. DON’T KNOW
-7. REFUSAL
How many days during the past week did you give your child a vegetable at dinner? Would you say…? SELECT ONE.
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
-4. DON’T KNOW
-7. REFUSAL
Did your child drink milk or use milk on his or her cereal at home during the past week? Would you say…? SELECT ONE.
1. Yes
2. No [Go to Question 17]
-4. DON’T KNOW [Go to Question 17]
-7. REFUSAL [Go to Question 17]
What kind of milk did your child drink or use on his or her cereal at home during the past week? Would you say…? SELECT ONE.
1. Regular whole milk
2. 2% milk
3. 1% milk
4. Skim or fat-free milk
5. Other type of milk (for example, soy or rice milk)
-4. DON’T KNOW
-7. REFUSAL
How many days during the past week did your child eat low-fat or fat-free yogurt at home? Would you say…? SELECT ONE.
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
-4. DON’T KNOW
-7. REFUSAL
How many days during the past week did your child eat regular-fat yogurt at home? Would you say…? SELECT ONE.
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
-4. DON’T KNOW
-7. REFUSAL
How many days during the past week did your child help you make or cook a meal? For example, did your child wash fruits or vegetables? Would you say…? SELECT ONE.
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
-4. DON’T KNOW
-7. REFUSAL
How many days during the past week did you make your child eat everything on his or her dinner plate? Would you say…? SELECT ONE.
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
-4. DON’T KNOW
-7. REFUSAL
For the next two questions, I’m going to read a statement. For each statement, please tell me if you strongly agree, agree, disagree, or strongly disagree with the statement.
How much do you agree or disagree with the following statement? “If my child eats healthy, he or she will be healthier when he or she gets older.” Would you say…? SELECT ONE.
1. Strongly agree
2. Agree
3. Disagree
4. Strongly disagree
-4. DON’T KNOW
-7. REFUSAL
How much do you agree or disagree with the following statement? “I am a good role model for my child by eating healthy foods.” Would you say…? SELECT ONE.
1. Strongly agree
2. Agree
3. Disagree
4. Strongly disagree
-4. DON’T KNOW
-7. REFUSAL
[IF ADMINISTRATION IS PRE-SURVEY/BASELINE, BOTH INTERVENTION AND CONTROL GROUPS GO TO Q35.]
[IF ADMINISTRATION IS POST-SURVEY, CONTROL GROUP THEN GO TO Q43] The last set of questions asks about materials your child got at day care and may have brought home.
Your child’s teacher sent home a handout about eating vegetables. Did you or someone else in your household do the handout with your child? SELECT ONE.
1. YES
2. NO
3. DID NOT GET HANDOUT
-4. DON’T KNOW
-7. REFUSAL
Your child’s teacher sent home a handout about eating fruit. Did you or someone else in your household do the handout with your child? SELECT ONE.
1. YES
2. NO
3. DID NOT GET HANDOUT
-4. DON’T KNOW
-7. REFUSAL
Your child’s teacher sent home a handout about drinking and eating low-fat dairy products. Did you or someone else in your household do the handout with your child? SELECT ONE.
1. YES
2. NO
3. DID NOT GET HANDOUT
-4. DON’T KNOW
-7. REFUSAL
Your child’s teacher sent home several “Parent Pages” with tips on healthy eating and healthy recipes. Did you or someone else in your household read the “Parent Pages”? Would you say…? SELECT ONE.
1. Yes, all or most of them
2. Yes, some of them
3. No
4. DID NOT GET THE “PARENT PAGES”
-4. DON’T KNOW
-7. REFUSAL
How easy was it to understand the handouts, the “Parent Pages,” and other materials sent home with your child? Would you say…? SELECT ONE.
1. Very easy
2. Easy
3. Somewhat easy
4. Not very easy
5. Not at all easy
6. DID NOT GET OR READ THE HANDOUTS, THE “PARENT PAGES,” AND OTHER MATERIALS [Go to Question 29.]
-4. DON’T KNOW
-7. REFUSAL
How useful were the handouts, the “Parent Pages,” and other materials sent home with your child in helping you to get your child to eat healthier? Would you say…? SELECT ONE.
1. Very useful
2. Useful
3. Somewhat useful
4. Not very useful
5. Not at all useful
6. DID NOT GET OR READ THE HANDOUTS, THE “PARENT PAGES,” AND OTHER MATERIALS
-4. DON’T KNOW
-7. REFUSAL
During the past two months, six classes for parents were conducted by a registered dietitian at your child care facility on why it is important to eat healthy and be physically active. Did you or someone else in your household go to any of these classes? SELECT ONE.
1. YES
2. N0 [Go to Question 33]
-4. DON’T KNOW [Go to Question 33]
-7. REFUSAL [Go to Question 33]
Of these six classes on healthy eating and physical activity, how many did you or someone else in your household attend? SELECT ONE.
1. One
2. Two
3. Three
4. Four
5. Five
6. Six [Go to Question 32]
-4. DON’T KNOW [Go to Question 32]
-7. REFUSAL [Go to Question 32]
Why did you decide not to go to all of the classes? Was it because…? SELECT ALL THAT APPLY.
1. You did not know about the other classes
2. The classes were offered at times that did not work for you
3. You did not think the classes would be useful
4. You do not like to go to classes like this
5. Other reason (SPECIFY):
-4. DON’T KNOW
-7. REFUSAL
How useful were the classes in helping you to get your child to eat healthier? Would you say…? SELECT ONE.
1. Very useful
2. Useful
3. Somewhat useful
4. Not very useful
5. Not at all useful
-4. DON’T KNOW
-7. REFUSAL
[ALL GO TO Q34.]
Why did you decide not to go to any of the classes? Was it because…? SELECT ALL THAT APPLY.
1. You did not know about the classes
2. The classes were offered at times that did work for you
3. You did not think the classes would be useful
4. You do not like to go to classes like this
5. Other reason (SPECIFY):
-4. DON’T KNOW
-7. REFUSAL
Please share any comments about the handouts, “Parent Pages,” and classes.
[ALL GO TO Q43.]
During the past year, how often did you run out of food before the end of the month? SELECT ONE.
1. Did not run out of food
2. Seldom
3. Sometimes
4. Most of the time
5. Almost always
-4. DON’T KNOW
-7. REFUSAL
How many people under 18 years of age live in your household?
____
-4. DON’T KNOW
-7. REFUSAL
Including yourself, how many people 18 years of age or older live in your household?
____
-4. DON’T KNOW
-7. REFUSAL
Which of the following categories best describes your age? SELECT ONE.
1. 18 to 24
2. 25 to 34
3. 35 to 44
4. 45 to 54
5. 55 to 64
6. 65 to 74
7. Over 74
-4. DON’T KNOW
-7. REFUSAL
What is your gender? SELECT ONE.
1. MALE
2. FEMALE
-4. DON’T KNOW
-7. REFUSAL
Are you Hispanic or Latino? SELECT ONE.
1. YES
2. NO
-4. DON’T KNOW
-7. REFUSAL
What is your race? SELECT ALL THAT APPLY.
1. American Indian or Alaska Native
2. Asian
3. Black or African American
4. Native Hawaiian or other Pacific Islander
5. White
-4. DON’T KNOW
-7. REFUSAL
Does your family speak English at home? Would you say you… SELECT ONE.
1. Speak English all of the time at home.
2. Speak English some of the time at home and speak another language some of the time.
3. Never speak English at home. We speak another language.
-4. DON’T KNOW
-7. REFUSAL
43. That is all the questions I have. Thank you for completing our survey. Before saying goodbye, I’d like to confirm that I have your correct name and address for sending your cash incentive in appreciation for completing this survey. I have [RESPONDENT NAME] spelled _____________________. Is this correct?
1. YES
2. CORRECT NAME [PROGRAMMER – SET UP TO ENTER CORRECTIONS]
-7. REFUSAL
44. For your street address, I have [RESPONDENT STREET ADDRESS] Is this correct?
1. YES
2. NO [PROGRAMMER – SET UP TO ENTER CORRECT ADDRESS]
-7 REFUSAL
45. For your city, state, and zip code, I have [RESPONDENT CITY, STATE, ZIP CODE] Is this correct?
1. YES
2. CORRECT CITY
3. CORRECT STATE
4. CORRECT ZIPCODE [PROGRAMMER – SET UP TO ALLOW FOR GENERATION OF ADDRESS LABELS FOR INCENTIVE LETTERS]
-7. REFUSAL
Thank you again. Have a nice (day/evening).
Spanish Version
Impact Evaluation Instrument for NYSDOH
For the NYSDOH project, we will survey parents/caregivers of preschool children at pre- and post-intervention using a mail/telephone survey approach. We provide the following four versions of the instrument:
1. mail questionnaire (pre-survey - intervention and control groups),
2. mail questionnaire (post-survey - intervention group),
3. mail questionnaire (post-survey - control group), and
4. telephone questionnaire for nonrespondents to mail survey (pre- and post-surveys - intervention and control groups).
OMB No. 0584-NEW
Fecha de expiración: XX/XXXX
Ver la declaración OMB en la parte interior de la portada
¿Qué come su niño?
|
|
¡Gracias por participar en este importante estudio!
Por favor, complete y devuelva la encuesta en el sobre adjunto a más tardar la próxima semana. Si tiene alguna pregunta sobre el estudio ¿Qué come su niño?, por favor envíe un mensaje por correo electrónico a xxxx@rti.org o llame al número gratuito 1-800-xxx-xxxx.
Se calcula que el tiempo aproximado que le tomará a cada participante en dar esta información será de 15 minutos, incluyendo el tiempo para repasar las instrucciones, buscar las fuentes de información existentes, juntar y mantener los datos requeridos, así como completar y revisar la recopilación de datos.
Ninguna agencia está autorizada a realizar o patrocinar ninguna recopilación de datos o información sin presentar un número actual de control OMB válido, ni está obligada ninguna persona a participar en una recopilación de datos si no existe dicho número.
Envíe sus comentarios acerca de este cálculo de tiempo o cualquier otro aspecto relacionado con esta recolección de datos, incluyendo sugerencias para reducir el tiempo, a: U.S. Department of Agriculture, Food and Nutrition Services, Office of Research and Analysis, Room 1014, Alexandria, VA 22302. ATTN: PRA (0584-xxxx*). No envíe el cuestionario con sus respuestas a esta dirección.
Si tiene preguntas sobre sus derechos como participante en un estudio, puede comunicarse con la Oficina de RTI para la Protección de Participantes en Estudios al número gratuito 1-866-214-2043.
What Does Your Child Eat?
(¿Qué come su niño?)
Mail Questionnaire
(Pre-survey, Intervention and Control Groups)
Instrument for NYSDOH Impact Evaluation
Esta encuesta pregunta sobre lo que come su niño(a). Este estudio está patrocinado por el Servicio de Alimentos y Nutrición del Departamento de Agricultura de los Estados Unidos y lo realiza RTI International, una organización sin fines de lucro que realiza estudios sobre la salud. La encuesta tomará entre 10 y 15 minutos en completarse. Usted recibirá $10 dólares por completar esta encuesta y $15 dólares por completar una segunda encuesta que le enviaremos por correo en aproximadamente 2 meses.
Todas sus respuestas a la encuesta se mantendrán privadas. Nosotros no compartiremos sus respuestas con nadie. Usted puede dejar de contestar cualquier pregunta que no desee contestar. Si tiene alguna pregunta, por favor llame a xxxx xxxx en RTI International al 1-800-xxx-xxxx.
Preguntas sobre la disponibilidad de ciertos alimentos en el hogar
1. ¿Estuvieron disponibles algunos de los siguientes alimentos en su hogar durante la semana pasada? Incluya alimentos frescos, congelados, enlatados y secos. (Marque con un círculo la respuesta Sí o No por cada alimento).
a. Plátanos |
Sí |
No |
b. Manzanas |
Sí |
No |
c. Uvas |
Sí |
No |
d. Melones (por ejemplo, melón amarillo, melón verde o sandía) |
Sí |
No |
e. Fresas |
Sí |
No |
f. Zanahorias |
Sí |
No |
g. Papas fritas en bolsa, nachos u hojuelas de maíz ‘corn chips’ |
Sí |
No |
h. Gaseosas o sodas regulares |
Sí |
No |
i. Gaseosas o sodas de dieta o de bajas calorías |
Sí |
No |
j. Leche regular entera o de 2% de grasa |
Sí |
No |
k. Leche de 1% de grasa o leche sin grasa |
Sí |
No |
Preguntas sobre las frutas y vegetales que come su niño(a)
Para las siguientes preguntas, piense en lo que su niño(a) comió durante la semana pasada o en los últimos 7 días. No incluya el tiempo en la escuela o la guardería infantil.
2. ¿Cuántos días durante la semana pasada comió su niño(a) más de un tipo de fruta cada día? No incluya jugo de frutas. (Marque una respuesta con un círculo).
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
3. Durante la semana pasada, ¿cuántas tazas de fruta comió su niño(a) cada día? No incluya jugo de frutas. (Marque una respuesta con un círculo).
1. Ninguna |
|
||||||
2. 1/2 taza |
|||||||
3. 1 taza |
|||||||
4. 1 ½ tazas |
|||||||
5. 2 tazas |
Ninguna |
|
1 taza |
|
2 tazas |
|
3 tazas |
6. 2 ½ tazas |
|
|
|
|
|
||
7. 3 tazas o más |
|
||||||
¿Cuántos días durante la semana pasada comió su niño(a) más de un tipo de vegetal cada día? No incluya jugo de vegetales. (Marque una respuesta con un círculo).
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
Durante la semana pasada, ¿cuántas tazas de vegetales comió su niño(a) cada día? No incluya jugo de vegetales. (Marque una respuesta con un círculo).
1. Ninguna
2. 1/2 taza
3. 1 taza
4. 1 ½ tazas
5. 2 tazas
Ninguna
1 taza
2 tazas
3 tazas
6. 2 ½ tazas
7. 3 tazas o más
Durante la semana pasada, ¿comió su niño(a) algún alimento o merienda o ‘snack’ que fue proporcionado por su escuela o guardería infantil? (Marque con un círculo todas las respuestas que correspondan).
1. Sí, en el desayuno
2. Sí, en el almuerzo
3. Sí, comió meriendas o ‘snacks’
4. No, no comió desayuno, almuerzo, ni meriendas o ‘snacks’ proporcionados por la escuela o guardería infantil.
¿Está su niño(a) dispuesto a probar un nuevo tipo de fruta? (Marque una respuesta con un círculo).
1. No
2. Quizás
3. Sí
¿Cuántos días durante la semana pasada le dio usted fruta a su niño(a) como merienda o ‘snack’? (Marque una respuesta con un círculo).
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
¿Cuántos días durante la semana pasada le pidió su niño(a) o se sirvió él o ella por sí mismo(a) fruta como merienda o ‘snack’? (Marque una respuesta con un círculo).
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
¿Cuántos días durante la semana pasada le dio a su niño(a) fruta en la cena? (Marque una respuesta con un círculo).
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
¿Está su niño(a) dispuesto(a) a probar un nuevo tipo de vegetal? (Marque una respuesta con un círculo).
1. No
2. Quizás
3. Sí
¿Cuántos días durante la semana pasada le dio vegetales a su niño(a) como merienda o ‘snack’? (Marque una respuesta con un círculo).
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
¿Cuántos días durante la semana pasada le pidió su niño(a) o se sirvió él o ella por sí mismo(a) vegetales como merienda o ‘snack’? (Marque una respuesta con un círculo).
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
¿Cuántos días durante la semana pasada le dio a su niño(a) vegetales en la cena? (Marque una respuesta con un círculo).
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
Preguntas sobre los productos lácteos que toma o come su niño(a)
¿Tomó su niño(a) leche o usó leche con su cereal en el hogar durante la semana pasada? (Marque una respuesta con un círculo).
1. Sí
2. No [Vaya a la pregunta 17]
¿Qué tipo de leche tomó o usó su niño(a) con su cereal en el hogar durante la semana pasada? (Marque una respuesta con un círculo).
1. Leche regular entera
2. Leche de 2% de grasa
3. Leche de 1% de grasa
4. Leche sin grasa
5. Otro tipo de leche (por ejemplo, leche de soya o de arroz)
¿Cuántos días durante la semana pasada comió su niño(a) yogurt bajo de grasa o sin grasa en el hogar? (Marque una respuesta con un círculo).
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
¿Cuántos días durante la semana pasada comió su niño(a) yogurt regular con grasa en el hogar? (Marque una respuesta con un círculo).
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
Preguntas sobre los hábitos alimenticios de su niño(a)
¿Cuántos días durante la semana pasada le ayudó su niño(a) a preparar o cocinar una comida? Por ejemplo, ¿lavó su niño(a) las frutas o vegetales? (Marque una respuesta con un círculo).
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
¿Cuántos días durante la semana pasada hizo usted que su niño(a) comiera todo lo que estaba en su plato de comida? (Marque una respuesta con un círculo).
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
¿Qué tan de acuerdo o en desacuerdo está usted con la siguiente declaración? “Si mi niño(a) come de manera saludable, él o ella será más saludable cuando tenga más edad”. (Marque una respuesta con un círculo).
1. Muy de acuerdo
2. De acuerdo
3. En desacuerdo
4. Muy en desacuerdo
¿Qué tan de acuerdo o en desacuerdo está usted con la siguiente declaración? “Yo soy un buen ejemplo para mi niño(a) al comer alimentos saludables”. (Marque una respuesta con un círculo).
1. Muy de acuerdo
2. De acuerdo
3. En desacuerdo
4. Muy en desacuerdo
Preguntas sobre usted y su hogar
Durante el año pasado, ¿con qué frecuencia se le acabó la comida antes de fin de mes? (Marque una respuesta con un círculo).
1. No se acabó la comida
2. Rara vez
3. Algunas veces
4. La mayor parte del tiempo
5. Casi siempre
¿Cuántas personas menores de 18 años de edad viven en su hogar?
____
Incluyéndose usted, ¿cuántas personas de 18 años de edad o más viven en su hogar?
____
¿Cuál de las siguientes categorías describe mejor su edad? (Marque una respuesta con un círculo).
1. De 18 a 24
2. De 25 a 34
3. De 35 a 44
4. De 45 a 54
5. De 55 a 64
6. De 65 a 74
7. Más de 74
¿Es usted hombre o mujer? (Marque una respuesta con un círculo).
1. Hombre
2. Mujer
¿Es usted hispano(a) o latino(a)? (Marque una respuesta con un círculo).
1. Sí
2. No
¿Cuál es su raza? (Marque una respuesta con un círculo).
1. India Americana o nativa de Alaska
2. Asiática
3. Negra o africana americana
4. Nativa de Hawai o de alguna otra isla del Pacífico
5. Blanca
¿Habla su familia inglés en el hogar? (Marque una respuesta con un círculo).
1. Hablamos inglés todo el tiempo en el hogar.
2. Hablamos inglés algunas veces en el hogar y también hablamos otro idioma algunas veces.
3. Nunca hablamos inglés en el hogar. Hablamos otro idioma.
Gracias
por completar la encuesta.
Por
favor, devuelva la encuesta en el sobre adjunto.
OMB No. 0584-NEW
Fecha de expiración: XX/XXXX
Ver la declaración OMB en la parte interior de la portada
¿Qué come su niño?
|
|
¡Gracias por participar en este importante estudio!
Por favor, complete y devuelva la encuesta en el sobre adjunto a más tardar la próxima semana. Si tiene alguna pregunta sobre el estudio ¿Qué come su niño?, por favor envíe un mensaje por correo electrónico a xxxx@rti.org o llame al número gratuito 1-800-xxx-xxxx.
Se calcula que el tiempo aproximado que le tomará a cada participante en dar esta información será de 15 minutos, incluyendo el tiempo para repasar las instrucciones, buscar las fuentes de información existentes, juntar y mantener los datos requeridos, así como completar y revisar la recopilación de datos.
Ninguna agencia está autorizada a realizar o patrocinar ninguna recopilación de datos o información sin presentar un número actual de control OMB válido, ni está obligada ninguna persona a participar en una recopilación de datos si no existe dicho número.
Envíe sus comentarios acerca de este cálculo de tiempo o cualquier otro aspecto relacionado con esta recolección de datos, incluyendo sugerencias para reducir el tiempo, a: U.S. Department of Agriculture, Food and Nutrition Services, Office of Research and Analysis, Room 1014, Alexandria, VA 22302. ATTN: PRA (0584-xxxx*). No envíe el cuestionario con sus respuestas a esta dirección.
Si tiene preguntas sobre sus derechos como participante en un estudio, puede comunicarse con la Oficina de RTI para la Protección de Participantes en Estudios al número gratuito 1-866-214-2043.
What Does Your Child Eat?
(¿Qué come su niño?)
Mail Questionnaire
(Post-survey, Intervention Group)
Instrument for NYSDOH Impact Evaluation
Esta encuesta pregunta sobre lo que come su niño(a). Este estudio está patrocinado por el Servicio de Alimentos y Nutrición del Departamento de Agricultura de los Estados Unidos y lo realiza RTI International, una organización sin fines de lucro que realiza estudios sobre la salud. La encuesta tomará entre 15 y 20 minutos en completarse. Usted recibirá $15 dólares por completar la entrevista.
Todas sus respuestas a la encuesta se mantendrán privadas. Nosotros no compartiremos sus respuestas con nadie. Usted puede dejar de contestar cualquier pregunta que no desee contestar. Si tiene alguna pregunta, por favor llame a xxxx xxxx en RTI International al 1-800-xxx-xxxx.
Preguntas sobre la disponibilidad de ciertos alimentos en el hogar
¿Estuvieron disponibles algunos de los siguientes alimentos en su hogar durante la semana pasada? Incluya alimentos frescos, congelados, enlatados y secos. (Marque con un círculo la respuesta Sí o No por cada alimento).
a. Plátanos |
Sí |
No |
b. Manzanas |
Sí |
No |
c. Uvas |
Sí |
No |
d. Melones (por ejemplo, melón amarillo, melón verde o sandía) |
Sí |
No |
e. Fresas |
Sí |
No |
f. Zanahorias |
Sí |
No |
g. Papas fritas en bolsa, nachos u hojuelas de maíz ‘corn chips’ |
Sí |
No |
h. Gaseosas o sodas regulares |
Sí |
No |
i. Gaseosas o sodas de dieta o de bajas calorías |
Sí |
No |
j. Leche regular entera o de 2% de grasa |
Sí |
No |
k. Leche de 1% de grasa o leche sin grasa |
Sí |
No |
Preguntas sobre las frutas y vegetales que come su niño(a)
Para las siguientes preguntas, piense en lo que su niño(a) comió durante la semana pasada o en los últimos 7 días. No incluya el tiempo en la escuela o la guardería infantil.
2. ¿Cuántos días durante la semana pasada comió su niño(a) más de un tipo de fruta cada día? No incluya jugo de frutas. (Marque una respuesta con un círculo).
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
3. Durante la semana pasada, ¿cuántas tazas de fruta comió su niño(a) cada día? No incluya jugo de frutas. (Marque una respuesta con un círculo).
1. Ninguna |
|
||||||
2. 1/2 taza |
|||||||
3. 1 taza |
|||||||
4. 1 ½ tazas |
|||||||
5. 2 tazas |
Ninguna |
|
1 taza |
|
2 tazas |
|
3 tazas |
6. 2 ½ tazas |
|
|
|
|
|
||
7. 3 tazas o más |
|
||||||
4. ¿Cuántos días durante la semana pasada comió su niño(a) más de un tipo de vegetal cada día? No incluya jugo de vegetales. (Marque una respuesta con un círculo).
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
5. Durante la semana pasada, ¿cuántas tazas de vegetales comió su niño(a) cada día? No incluya jugo de vegetales. (Marque una respuesta con un círculo).
1. Ninguna |
|
||||||
2. 1/2 taza |
|||||||
3. 1 taza |
|||||||
4. 1 ½ tazas |
|||||||
5. 2 tazas |
Ninguna |
|
1 taza |
|
2 tazas |
|
3 tazas |
6. 2 ½ tazas |
|
|
|
|
|
||
7. 3 tazas o más |
|
||||||
Durante la semana pasada, ¿comió su niño(a) algún alimento o merienda o ‘snack’ que fue proporcionado por su escuela o guardería infantil? (Marque con un círculo todas las respuestas que correspondan).
1. Sí, en el desayuno
2. Sí, en el almuerzo
3. Sí, comió meriendas o ‘snacks’
4. No, no comió desayuno, almuerzo, ni meriendas o ‘snacks’ proporcionados por la escuela o guardería infantil.
¿Está su niño(a) dispuesto a probar un nuevo tipo de fruta? (Marque una respuesta con un círculo).
1. No
2. Quizás
3. Sí
¿Cuántos días durante la semana pasada le dio usted fruta a su niño(a) como merienda o ‘snack’? (Marque una respuesta con un círculo).
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
¿Cuántos días durante la semana pasada le pidió su niño(a) o se sirvió él o ella por sí mismo(a) fruta como merienda o ‘snack’? (Marque una respuesta con un círculo).
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
¿Cuántos días durante la semana pasada le dio a su niño(a) fruta en la cena? (Marque una respuesta con un círculo).
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
¿Está su niño(a) dispuesto(a) a probar un nuevo tipo de vegetal? (Marque una respuesta con un círculo).
1. No
2. Quizás
3. Sí
¿Cuántos días durante la semana pasada le dio vegetales a su niño(a) como merienda o ‘snack’? (Marque una respuesta con un círculo).
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
¿Cuántos días durante la semana pasada le pidió su niño(a) o se sirvió él o ella por sí mismo(a) vegetales como merienda o ‘snack’? (Marque una respuesta con un círculo).
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
¿Cuántos días durante la semana pasada le dio a su niño(a) vegetales en la cena? (Marque una respuesta con un círculo).
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
Preguntas sobre los productos lácteos que toma o come su niño(a)
¿Tomó su niño(a) leche o usó leche con su cereal en el hogar durante la semana pasada? (Marque una respuesta con un círculo).
1. Sí
2. No [Vaya a la pregunta 17]
¿Qué tipo de leche tomó o usó su niño(a) con su cereal en el hogar durante la semana pasada? (Marque una respuesta con un círculo).
1. Leche regular entera
2. Leche de 2% de grasa
3. Leche de 1% de grasa
4. Leche sin grasa
5. Otro tipo de leche (por ejemplo, leche de soya o de arroz)
¿Cuántos días durante la semana pasada comió su niño(a) yogurt bajo de grasa o sin grasa en el hogar? (Marque una respuesta con un círculo).
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
¿Cuántos días durante la semana pasada comió su niño(a) yogurt regular con grasa en el hogar? (Marque una respuesta con un círculo).
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
Preguntas sobre los hábitos alimenticios de su niño(a)
¿Cuántos días durante la semana pasada le ayudó su niño(a) a preparar o cocinar una comida? Por ejemplo, ¿lavó su niño(a) las frutas o vegetales? (Marque una respuesta con un círculo).
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
¿Cuántos días durante la semana pasada hizo usted que su niño(a) comiera todo lo que estaba en su plato de comida? (Marque una respuesta con un círculo).
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
¿Qué tan de acuerdo o en desacuerdo está usted con la siguiente declaración? “Si mi niño(a) come de manera saludable, él o ella será más saludable cuando tenga más edad”. (Marque una respuesta con un círculo).
1. Muy de acuerdo
2. De acuerdo
3. En desacuerdo
4. Muy en desacuerdo
¿Qué tan de acuerdo o en desacuerdo está usted con la siguiente declaración? “Yo soy un buen ejemplo para mi niño(a) al comer alimentos saludables”. (Marque una respuesta con un círculo).
1. Muy de acuerdo
2. De acuerdo
3. En desacuerdo
4. Muy en desacuerdo
Preguntas sobre materiales que su niño(a) recibió en la guardería infantil
El/La maestro(a) de su niño(a) envió al hogar una hoja informativa sobre el comer vegetales. ¿Usó usted o alguien más en su hogar la hoja informativa con su niño(a)? (Marque una respuesta con un círculo).
1. Sí
2. No
3. No recibí la hoja informativa
El/La maestro(a) de su niño(a) envió al hogar una hoja informativa sobre el comer frutas. ¿Usó usted o alguien más en su hogar la hoja informativa con su niño(a)? (Marque una respuesta con un círculo).
1. Sí
2. No
3. No recibí la hoja informativa
El/La maestro(a) de su niño(a) envió al hogar una hoja informativa sobre el tomar y comer productos lácteos bajos en grasa. ¿Usó usted o alguien más en su hogar la hoja informativa con su niño(a)? (Marque una respuesta con un círculo).
1. Sí
2. No
3. No recibí la hoja informativa
El/La maestro(a) de su niño(a) envió al hogar varias “Hojas informativas para los padres” con consejos sobre el comer de manera saludable y preparar recetas saludables. ¿Leyó usted o alguien más en su hogar las “Hojas informativas para los padres”? (Marque una respuesta con un círculo).
1. Sí, leí todas las hojas o la mayoría de ellas
2. Sí, leí algunas de las hojas
3. No
4. No recibí las “Hojas informativas para los padres”
¿Qué tan fácil fue entender las hojas informativas sobre el comer vegetales, frutas y productos lácteos bajos en grasa, las “Hojas informativas para los padres” y otros materiales que se enviaron al hogar con su niño(a)? (Marque una respuesta con un círculo).
1. Muy fácil
2. Fácil
3. Algo fácil
4. No muy fácil
5. Nada fácil
6. No recibí o leí las hojas informativas sobre el comer vegetales, frutas y productos lácteos bajos en grasa, las “Hojas informativas para los padres” y otros materiales
¿Qué tan útil fueron las hojas informativas sobre el comer vegetales, frutas y productos lácteos bajos en grasa, las “Hojas informativas para los padres” y otros materiales que se enviaron al hogar con su niño(a) para ayudarlo(a) a usted a hacer que su niño(a) coma de manera más saludable? (Marque una respuesta con un círculo).
1. Muy fácil
2. Fácil
3. Algo fácil
4. No muy fácil
5. Nada fácil
6. No recibí o leí las hojas informativas sobre el comer vegetales, frutas y productos lácteos bajos en grasa, las “Hojas informativas para los padres” y otros materiales
Durante los últimos dos meses, se ofrecieron seis clases para los padres por una dietista certificada en la guardería infantil de su niño(a) sobre la importancia de comer de manera saludable y de ser activo(a) físicamente. ¿Asistió usted o alguien más en su hogar a alguna de estas clases? (Marque una respuesta con un círculo).
1. Sí
2. No [Vaya a la pregunta 33]
De estas seis clases sobre el comer de manera saludable y la actividad física, ¿a cuántas de ellas asistió usted o alguien más en su hogar? (Marque una respuesta con un círculo).
1. Una
2. Dos
3. Tres
4. Cuatro
5. Cinco
6. Seis [Vaya a la pregunta 32]
¿Por qué decidió no ir a todas las clases? (Marque una respuesta con un círculo).
1. No sabía de las otras clases
2. Las clases se ofrecían a horas que no eran convenientes para mí
3. No pensé que las clases serían de utilidad
4. No me gusta ir a clases de este tipo
5. Otra razón (especifique):
¿Qué tan útiles fueron las clases para ayudarlo(a) a usted a hacer que su niño(a) coma de manera más saludable? (Marque una respuesta con un círculo). [Vaya a la pregunta 34 después de contestar esta pregunta.]
1. Muy útil
2. Útil
3. Algo útil
4. No muy útil
5. Nada útil
¿Por qué decidió no ir a ninguna de las clases? (Marque con un círculo todas las respuestas que correspondan.)
1. No sabía de las otras clases
2. Las clases se ofrecían a horas que no eran convenientes para mí
3. No pensé que las clases serían de utilidad
4. No me gusta ir a clases de este tipo
5. Otra razón (especifique):
Por favor, comparta cualquier comentario que tenga acerca de las hojas informativas sobre el comer vegetales, frutas y productos lácteos bajos en grasa, las “Hojas informativas para los padres” y las clases.
Gracias por completar nuestra encuesta.
Por favor,
devuelva la encuesta en el sobre adjunto.
OMB No. 0584-NEW
Fecha de expiración: XX/XXXX
Ver la declaración OMB en la parte interior de la portada
¿Qué come su niño?
|
|
¡Gracias por participar en este importante estudio!
Por favor, complete y devuelva la encuesta en el sobre adjunto a más tardar la próxima semana. Si tiene alguna pregunta sobre el estudio ¿Qué come su niño?, por favor envíe un mensaje por correo electrónico a xxxx@rti.org o llame al número gratuito 1-800-xxx-xxxx.
Se calcula que el tiempo aproximado que le tomará a cada participante en dar esta información será de 15 minutos, incluyendo el tiempo para repasar las instrucciones, buscar las fuentes de información existentes, juntar y mantener los datos requeridos, así como completar y revisar la recopilación de datos.
Ninguna agencia está autorizada a realizar o patrocinar ninguna recopilación de datos o información sin presentar un número actual de control OMB válido, ni está obligada ninguna persona a participar en una recopilación de datos si no existe dicho número.
Envíe sus comentarios acerca de este cálculo de tiempo o cualquier otro aspecto relacionado con esta recolección de datos, incluyendo sugerencias para reducir el tiempo, a: U.S. Department of Agriculture, Food and Nutrition Services, Office of Research and Analysis, Room 1014, Alexandria, VA 22302. ATTN: PRA (0584-xxxx*). No envíe el cuestionario con sus respuestas a esta dirección.
Si tiene preguntas sobre sus derechos como participante en un estudio, puede comunicarse con la Oficina de RTI para la Protección de Participantes en Estudios al número gratuito 1-866-214-2043.
What
Does Your Child Eat? (¿Qué
come su niño?)
Mail
Questionnaire (Post-survey, Control Group)
Instrument for NYSDOH Impact Evaluation
Esta encuesta pregunta sobre lo que come su niño(a). Este estudio está patrocinado por el Servicio de Alimentos y Nutrición del Departamento de Agricultura de los Estados Unidos y lo realiza RTI International, una organización sin fines de lucro que realiza estudios sobre la salud. La encuesta tomará entre 15 y 20 minutos en completarse. Usted recibirá $15 dólares por completar la entrevista.
Todas sus respuestas a la encuesta se mantendrán privadas. Nosotros no compartiremos sus respuestas con nadie. Usted puede dejar de contestar cualquier pregunta que no desee contestar. Si tiene alguna pregunta, por favor llame a xxxx xxxx en RTI International al 1-800-xxx-xxxx.
Preguntas sobre la disponibilidad de ciertos alimentos en el hogar
1. ¿Estuvieron disponibles algunos de los siguientes alimentos en su hogar durante la semana pasada? Incluya alimentos frescos, congelados, enlatados y secos. (Marque con un círculo la respuesta Sí o No por cada alimento).
a. Plátanos |
Sí |
No |
b. Manzanas |
Sí |
No |
c. Uvas |
Sí |
No |
d. Melones (por ejemplo, melón amarillo, melón verde o sandía) |
Sí |
No |
e. Fresas |
Sí |
No |
f. Zanahorias |
Sí |
No |
g. Papas fritas en bolsa, nachos u hojuelas de maíz ‘corn chips’ |
Sí |
No |
h. Gaseosas o sodas regulares |
Sí |
No |
i. Gaseosas o sodas de dieta o de bajas calorías |
Sí |
No |
j. Leche regular entera o de 2% de grasa |
Sí |
No |
k. Leche de 1% de grasa o leche sin grasa |
Sí |
No |
Preguntas sobre las frutas y vegetales que come su niño(a)
Para las siguientes preguntas, piense en lo que su niño(a) comió durante la semana pasada o en los últimos 7 días. No incluya el tiempo en la escuela o la guardería infantil.
2. ¿Cuántos días durante la semana pasada comió su niño(a) más de un tipo de fruta cada día? No incluya jugo de frutas. (Marque una respuesta con un círculo).
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
3. Durante la semana pasada, ¿cuántas tazas de fruta comió su niño(a) cada día? No incluya jugo de frutas. (Marque una respuesta con un círculo).
1. Ninguna |
|
||||||
2. 1/2 taza |
|||||||
3. 1 taza |
|||||||
4. 1 ½ tazas |
|||||||
5. 2 tazas |
Ninguna |
|
1 taza |
|
2 tazas |
|
3 tazas |
6. 2 ½ tazas |
|
|
|
|
|
||
7. 3 tazas o más |
|
||||||
4. ¿Cuántos días durante la semana pasada comió su niño(a) más de un tipo de vegetal cada día? No incluya jugo de vegetales. (Marque una respuesta con un círculo).
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
5. Durante la semana pasada, ¿cuántas tazas de vegetales comió su niño(a) cada día? No incluya jugo de vegetales. (Marque una respuesta con un círculo).
1. Ninguna |
|
||||||
2. 1/2 taza |
|||||||
3. 1 taza |
|||||||
4. 1 ½ tazas |
|||||||
5. 2 tazas |
Ninguna |
|
1 taza |
|
2 tazas |
|
3 tazas |
6. 2 ½ tazas |
|
|
|
|
|
||
7. 3 tazas o más |
|
||||||
6. Durante la semana pasada, ¿comió su niño(a) algún alimento o merienda o ‘snack’ que fue proporcionado por su escuela o guardería infantil? (Marque con un círculo todas las respuestas que correspondan).
1. Sí, en el desayuno
2. Sí, en el almuerzo
3. Sí, comió meriendas o ‘snacks’
4. No, no comió desayuno, almuerzo, ni meriendas o ‘snacks’ proporcionados por la escuela o guardería infantil.
7. ¿Está su niño(a) dispuesto a probar un nuevo tipo de fruta? (Marque una respuesta con un círculo).
1. No
2. Quizás
3. Sí
8. ¿Cuántos días durante la semana pasada le dio usted fruta a su niño(a) como merienda o ‘snack’? (Marque una respuesta con un círculo).
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
9. ¿Cuántos días durante la semana pasada le pidió su niño(a) o se sirvió él o ella por sí mismo(a) fruta como merienda o ‘snack’? (Marque una respuesta con un círculo).
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
10. ¿Cuántos días durante la semana pasada le dio a su niño(a) fruta en la cena? (Marque una respuesta con un círculo).
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
11. ¿Está su niño(a) dispuesto(a) a probar un nuevo tipo de vegetal? (Marque una respuesta con un círculo).
1. No
2. Quizás
3. Sí
12. ¿Cuántos días durante la semana pasada le dio vegetales a su niño(a) como merienda o ‘snack’? (Marque una respuesta con un círculo).
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
13. ¿Cuántos días durante la semana pasada le pidió su niño(a) o se sirvió él o ella por sí mismo(a) vegetales como merienda o ‘snack’? (Marque una respuesta con un círculo).
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
14. ¿Cuántos días durante la semana pasada le dio a su niño(a) vegetales en la cena? (Marque una respuesta con un círculo).
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
Preguntas sobre los productos lácteos que toma o come su niño(a)
15. ¿Tomó su niño(a) leche o usó leche con su cereal en el hogar durante la semana pasada? (Marque una respuesta con un círculo).
1. Sí
2. No [Vaya a la pregunta 17]
16. ¿Qué tipo de leche tomó o usó su niño(a) con su cereal en el hogar durante la semana pasada? (Marque una respuesta con un círculo).
1. Leche regular entera
2. Leche de 2% de grasa
3. Leche de 1% de grasa
4. Leche sin grasa
5. Otro tipo de leche (por ejemplo, leche de soya o de arroz)
17. ¿Cuántos días durante la semana pasada comió su niño(a) yogurt bajo de grasa o sin grasa en el hogar? (Marque una respuesta con un círculo).
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
18. ¿Cuántos días durante la semana pasada comió su niño(a) yogurt regular con grasa en el hogar? (Marque una respuesta con un círculo).
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
Preguntas sobre los hábitos alimenticios de su niño(a)
19. ¿Cuántos días durante la semana pasada le ayudó su niño(a) a preparar o cocinar una comida? Por ejemplo, ¿lavó su niño(a) las frutas o vegetales? (Marque una respuesta con un círculo).
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
20. ¿Cuántos días durante la semana pasada hizo usted que su niño(a) comiera todo lo que estaba en su plato de comida? (Marque una respuesta con un círculo).
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
21. ¿Qué tan de acuerdo o en desacuerdo está usted con la siguiente declaración? “Si mi niño(a) come de manera saludable, él o ella será más saludable cuando tenga más edad”. (Marque una respuesta con un círculo).
1. Muy de acuerdo
2. De acuerdo
3. En desacuerdo
4. Muy en desacuerdo
22. ¿Qué tan de acuerdo o en desacuerdo está usted con la siguiente declaración? “Yo soy un buen ejemplo para mi niño(a) al comer alimentos saludables”. (Marque una respuesta con un círculo).
1. Muy de acuerdo
2. De acuerdo
3. En desacuerdo
4. Muy en desacuerdo
Gracias por completar nuestra encuesta.
Por favor,
devuelva la encuesta en el sobre adjunto.
OMB No. 0584-NEW
Fecha de expiración: XX/XXXX
What Does Your Child Eat?
(¿Qué come su niño?)
Telephone
Questionnaire for Nonrespondents
(Pre- and Post-surveys, Intervention and Control Groups)
Instrument for NYSDOH Impact Evaluation
1. Para comenzar esta encuesta, le voy a leer una lista de alimentos. Por cada uno de ellos, dígame por favor si estuvo disponible ese alimento en su hogar durante la semana pasada. Por favor, incluya alimentos frescos, congelados, enlatados y secos. Responda sí o no por cada alimento. El primer alimento es…
a. Plátanos |
Sí |
No |
DK |
RF |
b. Manzanas |
Sí |
No |
DK |
RF |
c. Uvas |
Sí |
No |
DK |
RF |
d. Melones (por ejemplo, melón amarillo, melón verde o sandía) |
Sí |
No |
DK |
RF |
e. Fresas |
Sí |
No |
DK |
RF |
f. Zanahorias |
Sí |
No |
DK |
RF |
g. Papas fritas en bolsa, nachos u hojuelas de maíz ‘corn chips’ |
Sí |
No |
DK |
RF |
h. Gaseosas o sodas regulares |
Sí |
No |
DK |
RF |
i. Gaseosas o sodas de dieta o de bajas calorías |
Sí |
No |
DK |
RF |
j. Leche regular entera o de 2% de grasa |
Sí |
No |
DK |
RF |
k. Leche de 1% de grasa o leche sin grasa |
Sí |
No |
DK |
RF |
Para las siguientes preguntas, piense sobre lo que su niño(a) comió durante la semana pasada o en los últimos 7 días. No incluya el tiempo en la escuela o la guardería infantil.
2. ¿Cuántos días durante la semana pasada comió su niño(a) más de un tipo de fruta cada día? No incluya jugo de frutas. ¿Diría usted… SELECT ONE.
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
-4. DON’T KNOW
-7. REFUSAL
3. Durante la semana pasada, ¿cuántas tazas de fruta comió su niño(a) cada día? No incluya jugo de frutas. ¿Diría que su niño(a) comió…? GIVE RESPONDENT PICTURE OF CUPS. SELECT ONE.
1. Ninguna fruta
2. ½ taza
3. 1 taza
4. 1 ½ tazas
5. 2 tazas
6. 2 ½ tazas
7. 3 tazas o más
-4. DON’T KNOW
-7. REFUSAL
4. ¿Cuántos días durante la semana pasada comió su niño(a) más de un tipo de vegetal cada día? No incluya jugo de vegetales. ¿Diría usted…? SELECT ONE.
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
-4. DON’T KNOW
-7. REFUSAL
5. Durante la semana pasada, ¿cuántas tazas de vegetales comió su niño(a) cada día? No incluya jugo de vegetales. ¿Diría usted que su niño(a) comió…? SELECT ONE.
1. Ningún vegetal
2. ½ taza
3. 1 taza
4. 1 ½ tazas
5. 2 tazas
6. 2 ½ tazas
7. 3 tazas o más
-4. DON’T KNOW
-7. REFUSAL
6. Durante la semana pasada, ¿comió su niño(a) algún alimento o merienda o ‘snack’ que fue proporcionado en su escuela o guardería infantil? ¿Diría usted que…? SELECT ALL THAT APPLY.
1. Sí, en el desayuno
2. Sí, en el almuerzo
3. Sí, comió meriendas o ‘snacks’
4. No, no comió en el desayuno, almuerzo, ni meriendas o ‘snacks’ proporcionados por la escuela o guardería infantil
-4. DON’T KNOW
-7. REFUSAL
7. ¿Está su niño(a) dispuesto(a) a probar un nuevo tipo de fruta? ¿Diría usted…? SELECT ONE.
1. No
2. Quizás
3. Sí
-4. DON’T KNOW
-7. REFUSAL
8. ¿Cuántos días durante la semana pasada le dio usted fruta a su niño(a) como merienda o ‘snack’? ¿Diría usted…? SELECT ONE.
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
-4. DON’T KNOW
-7. REFUSAL
9. ¿Cuántos días durante la semana pasada le pidió su niño(a) o se sirvió él o ella por sí mismo(a) fruta como merienda o ‘snack’? ¿Diría usted…? SELECT ONE.
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
-4. DON’T KNOW
-7. REFUSAL
10. ¿Cuántos días durante la semana pasada le dio a su niño(a) fruta en la cena? ¿Diría usted…? SELECT ONE.
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
-4. DON’T KNOW
-7. REFUSAL
11. ¿Estaría su niño(a) dispuesto(a) a probar un nuevo tipo de vegetal? ¿Diría usted…? SELECT ONE.
1. No
2. Quizás
3. Sí
-4. DON’T KNOW
-7. REFUSAL
12. ¿Cuántos días durante la semana pasada le dio vegetales a su niño(a) como merienda o ‘snack’? ¿Diría usted…? SELECT ONE.
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
-4. DON’T KNOW
-7. REFUSAL
13. ¿Cuántos días durante la semana pasada le pidió su niño(a) o se sirvió él o ella por sí mismo(a) vegetales como merienda o ‘snack’? ¿Diría usted…? SELECT ONE.
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
-4. DON’T KNOW
-7. REFUSAL
14. ¿Cuántos días durante la semana pasada le dio a su niño(a) vegetales en la cena? ¿Diría usted…? SELECT ONE.
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
-4. DON’T KNOW
-7. REFUSAL
15. ¿Tomó su niño(a) leche o usó leche con su cereal en el hogar durante la semana pasada? ¿Diría usted…? SELECT ONE.
1. Sí
2. No [Go to Question 17]
-4. DON’T KNOW [Go to Question 17]
-7. REFUSAL [Go to Question 17]
16. ¿Qué tipo de leche tomó o usó su niño(a) con su cereal en el hogar durante la semana pasada? ¿Diría usted…? SELECT ONE.
1. Leche regular entera
2. Leche de 2% de grasa
3. Leche de 1% de grasa
4. Leche sin grasa
5. Otro tipo de leche (por ejemplo, leche de soya o de arroz)
-4. DON’T KNOW
-7. REFUSAL
17. ¿Cuántos días durante la semana pasada comió su niño(a) yogurt bajo de grasa o sin grasa en el hogar? ¿Diría usted…? SELECT ONE.
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
-4. DON’T KNOW
-7. REFUSAL
18. ¿Cuántos días durante la semana pasada comió su niño(a) yogurt regular con grasa en el hogar? ¿Diría usted…? SELECT ONE.
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
-4. DON’T KNOW
-7. REFUSAL
19. ¿Cuántos días durante la semana pasada le ayudó su niño(a) a preparar o cocinar una comida? Por ejemplo, ¿lavó su niño(a) las frutas o vegetales?¿Diría usted…? SELECT ONE.
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
-4. DON’T KNOW
-7. REFUSAL
20. ¿Cuántos días durante la semana pasada hizo usted que su niño(a) comiera todo lo que estaba en su plato de comida? ¿Diría usted…? SELECT ONE.
1. Ninguno
2. De 1 a 2 días
3. De 3 a 4 días
4. De 5 a 6 días
5. Todos los días
-4. DON’T KNOW
-7. REFUSAL
Para las siguientes dos preguntas, le voy a leer una declaración. Por cada declaración, dígame por favor si usted está muy de acuerdo, de acuerdo, en desacuerdo o muy en desacuerdo con la declaración.
21. ¿Qué tan de acuerdo o en desacuerdo está usted con la siguiente declaración? “Si mi niño(a) come de manera saludable, él o ella será más saludable cuando tenga más edad”. ¿Diría usted…? SELECT ONE.
1. Muy de acuerdo
2. De acuerdo
3. En desacuerdo
4. Muy en desacuerdo
-4. DON’T KNOW
-7. REFUSAL
22. ¿Qué tan de acuerdo o en desacuerdo está usted con la siguiente declaración? “Yo soy un buen ejemplo para mi niño(a) al comer alimentos saludables”. ¿Diría usted…? SELECT ONE.
1. Muy de acuerdo
2. De acuerdo
3. En desacuerdo
4. Muy en desacuerdo
-4. DON’T KNOW
-7. REFUSAL
[IF ADMINISTRATION IS PRE-SURVEY/BASELINE, BOTH INTERVENTION AND CONTROL GROUPS GO TO Q 35.]
[IF ADMINISTRATION IS POST-SURVEY, CONTROL GROUP THEN GO TO Q43]
El último grupo de preguntas son acerca de los materiales que recibió su niño(a) en la escuela y que puede haber llevado al hogar.
23. El/La maestro(a) de su niño(a) envió al hogar una hoja informativa sobre el comer vegetales. ¿Usó usted o alguien más en su hogar la hoja informativa con su niño(a)? (Marque una respuesta con un círculo). SELECT ONE.
1. YES
2. NO
3. DID NOT GET HANDOUT
-4. DON’T KNOW
-7. REFUSAL
24. El/La maestro(a) de su niño(a) envió al hogar una hoja informativa sobre el comer frutas. ¿Usó usted o alguien más en su hogar la hoja informativa con su niño(a)? SELECT ONE.
1. YES
2. NO
3. DID NOT GET HANDOUT
-4. DON’T KNOW
-7. REFUSAL
25. El/La maestro(a) de su niño(a) envió al hogar una hoja informativa sobre el tomar y comer productos lácteos bajos en grasa. ¿Usó usted o alguien más en su hogar la hoja informativa con su niño(a)? SELECT ONE.
1. YES
2. NO
3. DID NOT GET HANDOUT
-4. DON’T KNOW
-7. REFUSAL
26. El/La maestro(a) de su niño(a) envió al hogar varias “Hojas informativas para los padres” con consejos sobre el comer de manera saludable y preparar recetas saludables. ¿Leyó usted o alguien más en su hogar las “Hojas informativas para los padres”? ¿Diría usted…? SELECT ONE.
1. Sí, leyó todas las hojas o la mayoría de ellas
2. Sí, leyó algunas de las hojas
3. No
4. DID NOT GET THE “HOJAS INFORMATIVAS PARA LOS PADRES”
-4. DON’T KNOW
-7. REFUSAL
27. ¿Qué tan fácil fue entender las hojas informativas sobre el comer vegetales, frutas y productos lácteos bajos en grasa, las “Hojas informativas para los padres” y otros materiales que se enviaron al hogar con su niño(a)? ¿Diría usted…? SELECT ONE.
1. Muy fácil
2. Fácil
3. Algo fácil
4. No muy fácil
5. Nada fácil
6. No recibió o leyó las hojas informativas sobre el comer vegetales, frutas y productos lácteos bajos en grasa, las “Hojas informativas para los padres” y otros materiales [Go to Question 29.]
-4. DON’T KNOW
-7. REFUSAL
28. ¿Qué tan útil fueron las hojas informativas sobre el comer vegetales, frutas y productos lácteos bajos en grasa, las “Hojas informativas para los padres” y otros materiales que se enviaron al hogar con su niño(a) para ayudarlo(a) a usted a hacer que su niño(a) coma de manera más saludable? ¿Diría usted…? SELECT ONE.
1. Muy fácil
2. Fácil
3. Algo fácil
4. No muy fácil
5. Nada fácil
6. [Don’t read] No recibió o leyó las hojas informativas sobre el comer vegetales, frutas y productos lácteos bajos en grasa, las “Hojas informativas para los padres” y otros materiales
-4. DON’T KNOW
-7. REFUSAL
29. Durante los últimos dos meses, se ofrecieron seis clases para los padres por una dietista certificada en la guardería infantil de su niño(a) sobre la importancia de comer de manera saludable y de ser activo(a) físicamente. ¿Asistió usted o alguien más en su hogar a alguna de estas clases? SELECT ONE.
1. YES
2. N0 [Go to Question 33]
-4. DON’T KNOW [Go to Question 33]
-7. REFUSAL [Go to Question 33]
30. De estas seis clases sobre el comer de manera saludable y la actividad física, ¿a cuántas de ellas asistió usted o alguien más en su hogar? SELECT ONE.
1. Una
2. Dos
3. Tres
4. Cuatro
5. Cinco
6. Seis [Go to Question 32]
-4. DON’T KNOW [Go to Question 32]
-7. REFUSAL [Go to Question 32]
31. ¿Por qué decidió no ir a todas las clases? ¿Fue porque…? SELECT ALL THAT APPLY.
1. No sabía de las otras clases
2. Las clases se ofrecían a horas que no eran convenientes para usted
3. No pensó que las clases serían de utilidad
4. No le gusta ir a clases de este tipo
5. Otra razón (SPECIFY):
-4. DON’T KNOW
-7. REFUSAL
32. ¿Qué tan útiles fueron las clases para ayudarlo(a) a usted a hacer que su niño(a) coma de manera más saludable? ¿Diría usted…? SELECT ONE.
1. Muy útil
2. Útil
3. Algo útil
4. No muy útil
5. Nada útil
-4. DON’T KNOW
-7. REFUSAL
[ALL GO TO Q34.]
33. ¿Por qué decidió no ir a todas las clases? ¿Fue porque…? SELECT ALL THAT APPLY.
1. No sabía de las otras clases
2. Las clases se ofrecían a horas que no eran convenientes para usted
3. No pensó que las clases serían de utilidad
4. No le gusta ir a clases de este tipo
5. Otra razón (SPECIFY):
-4. DON’T KNOW
-7. REFUSAL
34. Por favor, comparta cualquier comentario que tenga acerca de las hojas informativas sobre el comer vegetales, frutas y productos lácteos bajos en grasa, las “Hojas informativas para los padres” y las clases.
[ALL GO TO Q43.]
35. Durante el año pasado, ¿con qué frecuencia se le acabó la comida antes de fin de mes? SELECT ONE.
1. No se acabó la comida
2. Rara vez
3. Algunas veces
4. La mayor parte del tiempo
5. Casi siempre
-4. DON’T KNOW
-7. REFUSAL
36. ¿Cuántas personas menores de 18 años de edad viven en su hogar?
____
-4. DON’T KNOW
-7. REFUSAL
37. Incluyéndose usted, ¿cuántas personas de 18 años de edad o más viven en su hogar?
____
-4. DON’T KNOW
-7. REFUSAL
38. ¿Cuál de las siguientes categorías describe mejor su edad? SELECT ONE.
1. De 18 a 24
2. De 25 a 34
3. De 35 a 44
4. De 45 a 54
5. De 55 a 64
6. De 65 a 74
7. Más de 74
-4. DON’T KNOW
-7. REFUSAL
39. ¿Es usted hombre o mujer? SELECT ONE.
1. HOMBRE
2. MUJER
-4. DON’T KNOW
-7. REFUSAL
40. ¿Es usted hispano(a) o latino(a)? SELECT ONE.
1. YES
2. NO
-4. DON’T KNOW
-7. REFUSAL
41. ¿Cuál es su raza? SELECT ALL THAT APPLY.
1. India Americana o nativa de Alaska
2. Asiática
3. Negra o africana americana
4. Nativa de Hawai o de alguna otra isla del Pacífico
5. Blanca
-4. DON’T KNOW
-7. REFUSAL
42. ¿Habla su familia inglés en el hogar? ¿Diría usted que…? SELECT ONE.
1. Hablan inglés todo el tiempo en el hogar.
2. Hablan inglés algunas veces en el hogar y también hablan otro idioma algunas veces.
3. Nunca hablan inglés en el hogar. Hablan otro idioma.
-4. DON’T KNOW
-7. REFUSAL
43. Estas son todas las preguntas. Gracias por completar nuestra encuesta. Antes de despedirme, me gustaría confirmar que tengo su nombre y dirección correctos para enviarle el incentivo en efectivo como agradecimiento por haber completado esta encuesta. Tengo aquí que su nombre es [RESPONDENT NAME] y se escribe _____________________. ¿Es correcto?
1. YES
2. CORRECT NAME [PROGRAMMER –SET UP TO ENTER CORRECTIONS]
-7. REFUSAL
44. Tengo aquí que su dirección es [RESPONDENT STREET ADDRESS] ¿Es correcto?
1. YES
2. NO [PROGRAMMER –SET UP TO ENTER CORRECT ADDRESS]
-7. REFUSAL
45. Tengo aquí que la ciudad, estado y código postal donde vive es [RESPONDENT CITY, STATE, ZIP CODE] ¿Es correcto?
1. YES
2. CORRECT CITY
3. CORRECT STATE
4. CORRECT ZIPCODE [PROGRAMMER –SET UP TO ENTER ALLOW FOR GENERATION OF ADDRESS LABELS FOR INCENTIVE LETTERS]
-7. REFUSAL
Gracias
nuevamente. Qué pase un buen día/una buena noche.
Impact Evaluation Instrument for PSU
For the PSU project, we will survey participants via the Internet at pre- and post‑intervention, with nonrespondents to the post-survey contacted by mail/telephone. We provide the following six versions of the instrument:
Internet questionnaire (pre-survey - intervention and control groups),
Internet questionnaire (post-survey - intervention and control groups),
mail questionnaire for nonrespondents to Internet survey (post-survey - intervention group),
mail questionnaire for program dropouts (post-survey - intervention group),
mail questionnaire for nonrespondents to Internet survey (post-survey - control group), and
telephone questionnaire for nonrespondents to Internet survey (post-survey - intervention and control groups).
OMB No. 0584-NEW
Expiration date: XX/XXXX
Survey
on What You Eat
Internet Questionnaire (Pre-survey, Intervention
and Control Groups)
Instrument for PSU Impact Evaluation
[The FNS survey will be integrated with the PSU survey. The PSU instrument will contain the introductory text and information about informed consent. The screen will also include the following statement regarding respondent burden.]
Public reporting burden for this collection of information is estimated to average 15 minutes per response, including the time for reviewing instructions, searching existing data sources, gathering and maintaining the data needed, and completing and reviewing the collection of information.
An agency may not conduct or sponsor, and a person is not required to respond to, a collection of information unless it displays a currently valid OMB control number.
Send comments regarding this burden estimate or any other aspect of this collection of information, including suggestions for reducing this burden, to: U.S. Department of Agriculture, Food and Nutrition Services, Office of Research and Analysis, Room 1014, Alexandria, VA 22302 ATTN: PRA (0584-xxxx*).
If you have questions regarding your rights as a research participant, you may contact RTI’s Office of Research Protection toll-free at 866-214-2043.
Questions on Whether Certain Foods Are Available At Home
Were any of the following foods available in your home during the past week? Include fresh, frozen, canned, and dried foods. (Select yes or no for each food.)
a. Bananas |
Yes |
No |
b. Apples |
Yes |
No |
c. Grapes |
Yes |
No |
d. Carrots |
Yes |
No |
e. Potato chips, nacho chips, or corn chips |
Yes |
No |
f. Regular soft drinks or sodas |
Yes |
No |
g. Diet soft drinks or sodas |
Yes |
No |
h. Regular whole or 2% milk |
Yes |
No |
i. 1% or skim milk |
Yes |
No |
Questions on Foods You Like or Dislike
How much would you say you like or dislike the following foods? (Select one for each food.)
|
Extremely Dislike |
|
|
|
Neither Like or Dislike |
|
|
|
Extremely Like |
|
|
a. Apples |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
b. Oranges |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
c. Orange juice |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
d. Green beans |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
e. Peas |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
f. Raw tomatoes |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
g. Broccoli |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
h. Cauliflower |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
i. Raw carrots |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
j. Tossed green salads |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
k. White bread |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
l. Whole-wheat bread |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
m. Whole milk |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
n. Skim or non-fat milk |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
Questions on Your Eating Habits
Do you take the skin off of chicken? (Select one.)
1. No
2. Yes, often
3. Yes, sometimes
4. Yes, everyday
How would you rate your eating habits? (Select one.)
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
10 |
poor |
|
|
fair |
|
|
good |
|
|
excellent |
Questions on the “About Eating” Program
How did you hear about the “About Eating” program? (Select all that apply.)
1. Sign posted at local job services office
2. Sign posted at local laundromat or store
3. Sign posted at County Assistance Office
4. Received email about the program
5. Received post card about the program
6. Other (specify):
.
7. Don’t remember
Why are you participating in the “About Eating” program? (Select all that apply.)
1. To lose weight
2. To eat healthier
3. To improve my health
4. To cook healthier for my family
5. To manage my food budget better
6. To receive the cash for being in the study
7. Other reason (specify):
.
Questions about You and Your Household
How many people under 18 years of age live in your household?
____
Including yourself, how many people 18 years of age or older live in your household?
____
How do you usually get on the Internet or Web? (Select one.)
1. Home
2. Work
3. Friend’s or neighbor’s home
4. Family member’s home
5. Library or community center
6. Other (specify):
.
How often do you get on the Internet or Web? (Select one.)
1. At least once per day
2. A few times per week
3. A few times per month
4. A few times per year
Which of the following categories best describes your age? (Select one.)
1. 18 to 24
2. 25 to 34
3. 35 to 45
Are you Hispanic or Latino? (Select one.)
1. Yes
2. No
What is your race? (Select all that apply.)
1. American Indian or Alaska Native
2. Asian
3. Black or African American
4. Native Hawaiian or other Pacific Islander
5. White
What is the highest level of schooling you have completed? (Select one.)
1. Did not complete high school
2. High school graduate or GED
3. Some college or 2-year degree
4. College degree
What is your marital status? (Select one.)
1. Married or living with a partner
2. Separate or divorced
3. Widowed
4. Never married
Thank you for completing our survey.
OMB No. 0584-NEW
Expiration date: XX/XXXX
Survey
on What You Eat
Internet Questionnaire (Post-survey,
Intervention and Control Groups)
Instrument for PSU Impact Evaluation
[The FNS survey will be integrated with the PSU survey. The PSU instrument will contain the introductory text and information about informed consent. The screen will also include the following statement regarding respondent burden.]
Public reporting burden for this collection of information is estimated to average 15 minutes per response, including the time for reviewing instructions, searching existing data sources, gathering and maintaining the data needed, and completing and reviewing the collection of information.
An agency may not conduct or sponsor, and a person is not required to respond to, a collection of information unless it displays a currently valid OMB control number.
Send comments regarding this burden estimate or any other aspect of this collection of information, including suggestions for reducing this burden, to: U.S. Department of Agriculture, Food and Nutrition Services, Office of Research and Analysis, Room 1014, Alexandria, VA 22302 ATTN: PRA (0584-xxxx*).
If you have questions regarding your rights as a research participant, you may contact RTI’s Office of Research Protection toll-free at 866-214-2043.
Questions on Whether Certain Foods Are Available At Home
Were any of the following foods available in your home during the past week? Include fresh, frozen, canned, and dried foods. (Select yes or no for each food.)
a. Bananas |
Yes |
No |
b. Apples |
Yes |
No |
c. Grapes |
Yes |
No |
d. Carrots |
Yes |
No |
e. Potato chips, nacho chips, or corn chips |
Yes |
No |
f. Regular soft drinks or sodas |
Yes |
No |
g. Diet soft drinks or sodas |
Yes |
No |
h. Regular whole or 2% milk |
Yes |
No |
i. 1% or skim milk |
Yes |
No |
Questions on Foods You Like or Dislike
How much would you say you like or dislike the following foods? (Select one answer for each food.)
|
Extremely Dislike |
|
|
|
Neither Like or Dislike |
|
|
|
Extremely Like |
|
|
a. Apples |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
b. Oranges |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
c. Orange juice |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
d. Green beans |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
e. Peas |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
f. Raw tomatoes |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
g. Broccoli |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
h. Cauliflower |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
i. Raw carrots |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
j. Tossed green salads |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
k. White bread |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
l. Whole-wheat bread |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
m. Whole milk |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
n. Skim or non-fat milk |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
Questions on the Fruits and Vegetables You Eat
For the next questions think about what you actually ate during the past week, or the past 7 days. Do not tell us what you think you should be eating or what you typically eat.
How many days during the past week did you eat fruit or vegetables as snacks? (Select one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
How many days during the past week did you eat more than one kind of fruit each day? Do not include fruit juice. (Select one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
During the past week, how many cups of fruit did you eat each day? Do not include fruit juice.
_____ cups per day (drop-down box with none, ½ cup, 1 cup, 1 ½ cups, 2 cups, 2 ½ cups, and 3 cups or more)
None
1 cup
2 cups
3 cups
How many days during the past week did you eat more than one kind of vegetable each day? Do not include vegetable juice. (Select one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
During the past week, how many cups of vegetables did you eat each day? Do not include vegetable juice.
_____ cups per day (drop-down box with none, ½ cup, 1 cup, 1 ½ cups, 2 cups, 2 ½ cups, and 3 cups or more) |
|
||||||
None |
|
1 cup |
|
2 cups |
|
3 cups |
|
|
|
|
|
|
|||
Questions on the Dairy Products You Eat
Did you drink milk or use milk on cereal during the past week? (Select one.)
1. Yes
2. No [GO TO QUESTION 10]
What kind of milk did you usually drink or use on cereal during the past week? (Select one.)
1. Regular whole milk
2. 2% milk
3. 1% milk
4. Skim on non-fat milk
5. Other type of milk (for example, soy or rice)
Other Questions on Your Eating Habits
Do you take the skin off of chicken? (Select one.)
1. No
2. Yes, often
3. Yes, sometimes
4. Yes, everyday
How would you rate your eating habits? (Select one.)
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
10 |
poor |
|
|
fair |
|
|
good |
|
|
excellent |
Questions on the “About Eating” Program (Intervention only)
How much do you agree or disagree with the following statements? (Select one answer for each statement.)
Strongly Agree
Agree
Disagree
Strongly Disagree
It is easy for me to get on the Internet or Web.
1
2
3
4
It was easy for me to move around the web site.
1
2
3
4
The directions for each lesson were clear.
1
2
3
4
I was able to jump to links of interest.
1
2
3
4
The information provided on the web site was easy to read.
1
2
3
4
The information provided on the web site was easy to understand.
1
2
3
4
The “About Eating” program made me feel self-conscious.
1
2
3
4
The “About Eating” program was designed for someone like me.
1
2
3
4
I thought the information provided on the web site was interesting.
1
2
3
4
I thought the information provided on the web site was factual.
1
2
3
4
I found the material in the lessons to be repetitive.
1
2
3
4
I was able to print resources, such as the Food Shopping List, from the web site.
1
2
3
4
I prefer to learn about nutrition and eating online instead of in-person with a nutritionist.
1
2
3
4
I would have preferred to go through the lessons on the web site at my own pace.
1
2
3
4
I would participate in a program like this again even if I did not receive the cash for being in the study
1
2
3
4
What do you think about the amount of time it took to complete the “About Eating” lessons? (Select one.)
1. Too long
2. Too short
3. Just right
Please rank the “About Eating” lessons in the order of how much you liked them, with 1 = “I liked the most” and 5 = “I liked the least.”
_____ The lesson on eating different kinds of food
_____ The lesson on enjoying your food
_____ The lesson on how to know when you are hungry or full
_____ The lesson on eating and feeding your family
_____ The lesson on physical activity
Please share any comments on the “About Eating” web site.
Thank you for completing our survey.
(Intervention only)
If you would be willing to talk to us in more detail about your experience with the “About Eating” program for an additional incentive of $15, please provide your name and telephone number, and we will get in touch with you within the next week, or call us at [INSERT 1-800#] at your earliest convenience.”
Name:
Telephone Number:
OMB No. 0584-NEW
Expiration date: XX/XXXX
See OMB statement on inside cover
Survey on What You Eat
|
|

Thank you for taking part in this important study!
Please fill out and return the survey in the enclosed envelope within the next week.
If you have any questions about the Survey on What You Eat, please send an e-mail to xxxx@rti.org or call toll-free at 1-800-xxx-xxxx.
Public reporting burden for this collection of information is estimated to average 15 minutes per response, including the time for reviewing instructions, searching existing data sources, gathering and maintaining the data needed, and completing and reviewing the collection of information.
An agency may not conduct or sponsor, and a person is not required to respond to, a collection of information unless it displays a currently valid OMB control number.
Send comments regarding this burden estimate or any other aspect of this collection of information, including suggestions for reducing this burden, to: U.S. Department of Agriculture, Food and Nutrition Services, Office of Research and Analysis, Room 1014, Alexandria, VA 22302 ATTN: PRA (0584-xxxx*). Do not return the completed form to this address.
If you have questions regarding your rights as a research participant, you may contact RTI’s Office of Research Protection toll-free at 866-214-2043.
Survey
on What You Eat
Mail Questionnaire for Nonrespondents to
Internet Survey
(Post-survey, Intervention Group)
Instrument for PSU Impact Evaluation
This survey asks about what you eat. This study is being sponsored by the U.S. Department of Agriculture’s Food & Nutrition Service and conducted by RTI International, a non-profit research organization. The survey will take about 10 to 15 minutes to complete. You will receive $15 for completing this survey.
All of your answers to the survey will be kept private. We will not share your answers with anyone. You may skip any questions you do not want to answer. If you have any questions, please call xxx xxxx at RTI International at 1-800-xxx-xxxx.
Questions on Whether Certain Foods Are Available At Home
Were any of the following foods available in your home during the past week? Include fresh, frozen, canned, and dried foods. (Circle yes or no for each food.)
a. Bananas |
Yes |
No |
b. Apples |
Yes |
No |
c. Grapes |
Yes |
No |
d. Carrots |
Yes |
No |
e. Potato chips, nacho chips, or corn chips |
Yes |
No |
f. Regular soft drinks or sodas |
Yes |
No |
g. Diet soft drinks or sodas |
Yes |
No |
h. Regular whole or 2% milk |
Yes |
No |
i. 1% or skim milk |
Yes |
No |
Questions on Foods You Like or Dislike
How much would you say you like or dislike the following foods? (Circle one answer for each food.)
|
Extremely Dislike |
|
|
|
Neither Like or Dislike |
|
|
|
Extremely Like |
|
|
a. Apples |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
b. Oranges |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
c. Orange juice |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
d. Green beans |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
e. Peas |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
f. Raw tomatoes |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
g. Broccoli |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
h. Cauliflower |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
i. Raw carrots |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
j. Tossed green salads |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
k. White bread |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
l. Whole-wheat bread |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
m. Whole milk |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
n. Skim or non-fat milk |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
Questions on the Fruits and Vegetables You Eat
For the next questions think about what you actually ate during the past week, or the past 7 days. Do not tell us what you think you should be eating or what you typically eat.
How many days during the past week did you eat fruit or vegetables as snacks? (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
How many days during the past week did you eat more than one kind of fruit each day? Do not include fruit juice. (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
During the past week, how many cups of fruit did you eat each day? Do not include fruit juice. (Circle one.)
1. None
2. 1/2 cup
3. 1 cup
4. 1 ½ cups
5. 2 cups
None
1 cup
2 cups
3 cups
6. 2 ½ cups
7. 3 cups or more
How many days during the past week did you eat more than one kind of vegetable each day? Do not include vegetable juice. (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
During the past week, how many cups of vegetables did you eat each day? Do not include vegetable juice. (Circle one.)
1. None |
|
||||||
2. 1/2 cup |
|||||||
3. 1 cup |
|||||||
4. 1 ½ cups |
|||||||
5. 2 cups |
None |
|
1 cup |
|
2 cups |
|
3 cups |
6. 2 ½ cups |
|
|
|
|
|
||
7. 3 cups or more |
|
||||||
Questions on the Dairy Products You Eat
Did you drink milk or use milk on cereal during the past week? (Circle one.)
1. Yes
2. No [GO TO QUESTION 10]
What kind of milk did you usually drink or use on cereal during the past week? (Circle one.)
1. Regular whole milk
2. 2% milk
3. 1% milk
4. Skim on non-fat milk
5. Other type of milk (for example, soy or rice)
Other Questions on Your Eating Habits
Do you take the skin off of chicken? (Circle one.)
1. No
2. Yes, often
3. Yes, sometimes
4. Yes, everyday
How would you rate your eating habits? (Circle one.)
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
10 |
poor |
|
|
fair |
|
|
good |
|
|
excellent |
Questions on the “About Eating” Program
Several weeks ago, you agreed to take part in a study being conducted by the Pennsylvania State University. As part of this study, you were asked to go to the web site called, “About Eating” and complete lessons on eating and exercise. The next questions ask about the “About Eating” program.
How much do you agree or disagree with the following statements? (Circle one answer for each statement.)
Strongly Agree
Agree
Disagree
Strongly Disagree
It is easy for me to get on the Internet or Web.
1
2
3
4
It was easy for me to move around the web site.
1
2
3
4
The directions for each lesson were clear.
1
2
3
4
I was able to jump to links of interest.
1
2
3
4
The information provided on the web site was easy to read.
1
2
3
4
The information provided on the web site was easy to understand.
1
2
3
4
The “About Eating” program made me feel self-conscious.
1
2
3
4
The “About Eating” program was designed for someone like me.
1
2
3
4
I thought the information provided on the web site was interesting.
1
2
3
4
I thought the information provided on the web site was factual.
1
2
3
4
I found the material in the lessons to be repetitive.
1
2
3
4
I was able to print resources, such as the Food Shopping List, from the web site.
1
2
3
4
I prefer to learn about nutrition and eating online instead of in-person with a nutritionist.
1
2
3
4
I would have preferred to go through the lessons on the web site at my own pace.
1
2
3
4
I would participate in a program like this again even if I did not receive the cash for being in the study
1
2
3
4
What do you think about the amount of time it took to complete the “About Eating” lessons? (Circle one.)
1. Too long
2. Too short
3. Just right
Please rank the “About Eating” lessons in the order of how much you liked them, with 1 = “I liked the most” and 5 = “I liked the least.”
_____ The lesson on eating different kinds of food
_____ The lesson on enjoying your food
_____ The lesson on how to know when you are hungry or full
_____ The lesson on eating and feeding your family
_____ The lesson on physical activity
Please share any comments on the “About Eating” web site.
Thank you for completing our survey.
Please return the survey in the enclosed envelope.
If you would be willing to talk to us in more detail about your experience with the “About Eating” program for an additional incentive of $15, please provide your name and telephone number, and we will get in touch with you within the next week, or call us at [INSERT 1-800#] at your earliest convenience.”
Name:
Telephone Number:
OMB No. 0584-NEW
Expiration date: XX/XXXX
See OMB statement on inside cover
Survey on What You Eat
|
|
Thank you for taking part in this important study!
Please fill out and return the survey in the enclosed envelope within the next week.
If you have any questions about the Survey on What You Eat, please send an e-mail to xxxx@rti.org or call toll-free at 1-800-xxx-xxxx.
Public reporting burden for this collection of information is estimated to average 15 minutes per response, including the time for reviewing instructions, searching existing data sources, gathering and maintaining the data needed, and completing and reviewing the collection of information.
An agency may not conduct or sponsor, and a person is not required to respond to, a collection of information unless it displays a currently valid OMB control number.
Send comments regarding this burden estimate or any other aspect of this collection of information, including suggestions for reducing this burden, to: U.S. Department of Agriculture, Food and Nutrition Services, Office of Research and Analysis, Room 1014, Alexandria, VA 22302 ATTN: PRA (0584-xxxx*). Do not return the completed form to this address.
If you have questions regarding your rights as a research participant, you may contact RTI’s Office of Research Protection toll-free at 866-214-2043.
Survey
on What You Eat
Mail Questionnaire for Program Dropouts
(Post-survey, Intervention Group)
Instrument for PSU Impact Evaluation
This survey asks about what you eat. This study is being sponsored by the U.S. Department of Agriculture’s Food & Nutrition Service and conducted by RTI International, a non-profit research organization. The survey will take about 10 to 15 minutes to complete. You will receive $15 for completing this survey.
All of your answers to the survey will be kept private. We will not share your answers with anyone. You may skip any questions you do not want to answer. If you have any questions, please call xxx xxxx at RTI International at 1-800-xxx-xxxx.
Questions on Whether Certain Foods Are Available At Home
Were any of the following foods available in your home during the past week? Include fresh, frozen, canned, and dried foods. (Circle yes or no for each food.)
a. Bananas |
Yes |
No |
b. Apples |
Yes |
No |
c. Grapes |
Yes |
No |
d. Carrots |
Yes |
No |
e. Potato chips, nacho chips, or corn chips |
Yes |
No |
f. Regular soft drinks or sodas |
Yes |
No |
g. Diet soft drinks or sodas |
Yes |
No |
h. Regular whole or 2% milk |
Yes |
No |
i. 1% or skim milk |
Yes |
No |
Questions on Foods You Like or Dislike
How much would you say you like or dislike the following foods? (Circle one answer for each food.)
|
Extremely Dislike |
|
|
|
Neither Like or Dislike |
|
|
|
Extremely Like |
|
|
a. Apples |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
b. Oranges |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
c. Orange juice |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
d. Green beans |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
e. Peas |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
f. Raw tomatoes |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
g. Broccoli |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
h. Cauliflower |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
i. Raw carrots |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
j. Tossed green salads |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
k. White bread |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
l. Whole-wheat bread |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
m. Whole milk |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
n. Skim or non-fat milk |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
Questions on the Fruits and Vegetables You Eat
For the next questions think about what you actually ate during the past week, or the past 7 days. Do not tell us what you think you should be eating or what you typically eat.
How many days during the past week did you eat fruit or vegetables as snacks? (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
How many days during the past week did you eat more than one kind of fruit each day? Do not include fruit juice. (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
During the past week, how many cups of fruit did you eat each day? Do not include fruit juice. (Circle one.)
1. None
2. 1/2 cup
3. 1 cup
4. 1 ½ cups
5. 2 cups
None
1 cup
2 cups
3 cups
6. 2 ½ cups
7. 3 cups or more
How many days during the past week did you eat more than one kind of vegetable each day? Do not include vegetable juice. (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
During the past week, how many cups of vegetables did you eat each day? Do not include vegetable juice. (Circle one.)
1. None |
|
||||||
2. 1/2 cup |
|||||||
3. 1 cup |
|||||||
4. 1 ½ cups |
|||||||
5. 2 cups |
None |
|
1 cup |
|
2 cups |
|
3 cups |
6. 2 ½ cups |
|
|
|
|
|
||
7. 3 cups or more |
|
||||||
Questions on the Dairy Products You Eat
Did you drink milk or use milk on cereal during the past week? (Circle one.)
1. Yes
2. No [GO TO QUESTION 10]
What kind of milk did you usually drink or use on cereal during the past week? (Circle one.)
1. Regular whole milk
2. 2% milk
3. 1% milk
4. Skim on non-fat milk
5. Other type of milk (for example, soy or rice)
Other Questions on Your Eating Habits
Do you take the skin off of chicken? (Circle one.)
1. No
2. Yes, often
3. Yes, sometimes
4. Yes, everyday
How would you rate your eating habits? (Circle one.)
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
10 |
poor |
|
|
fair |
|
|
good |
|
|
excellent |
Questions on the “About Eating” Program
Several weeks ago, you agreed to take part in a study being conducted by the Pennsylvania State University. As part of this study, you were asked to go to the web site called, “About Eating” and complete lessons on eating and exercise. The next questions ask about the “About Eating” program.
Which lesson(s) did you complete on the “About Eating” web site? (Circle all that apply.)
1. The lesson on eating different kinds of food
2. The lesson on enjoying your food
3. The lesson on how to know when you are hungry or full
4. The lesson on eating and feeding your family
5. The lesson on physical activity
6. I did not complete any of the lessons
7. I do not remember which lesson(s) I completed
Why did you decide not to complete all of the “About Eating” lessons? (Circle all that apply.)
1. The lessons were not useful
2. The lessons were not interesting
3. The lessons were difficult to read and understand
4. It was difficult to move around the web site
5. The lessons were too long
6. Too busy with other activities, like work or family
7. Limited access to Internet/Web or a computer
8. Other reason (specify):
14. How much do you agree or disagree with the following statements? (Circle one answer for each statement.)
|
Strongly Agree |
Agree |
Disagree |
Strongly Disagree |
No Opinion |
|
1 |
2 |
3 |
4 |
-5 |
|
1 |
2 |
3 |
4 |
-5 |
|
1 |
2 |
3 |
4 |
-5 |
|
1 |
2 |
3 |
4 |
-5 |
|
1 |
2 |
3 |
4 |
-5 |
|
1 |
2 |
3 |
4 |
-5 |
|
1 |
2 |
3 |
4 |
-5 |
|
1 |
2 |
3 |
4 |
-5 |
|
1 |
2 |
3 |
4 |
-5 |
|
1 |
2 |
3 |
4 |
-5 |
|
1 |
2 |
3 |
4 |
-5 |
|
1 |
2 |
3 |
4 |
-5 |
|
1 |
2 |
3 |
4 |
-5 |
|
1 |
2 |
3 |
4 |
-5 |
|
1 |
2 |
3 |
4 |
-5 |
15. What do you think about the amount of time it took to complete the “About Eating” lessons? (Circle one.)
1. Too long
2. Too short
3. Just right
Please share any comments on the “About Eating” web site.
Thank you for completing our survey.
Please return survey in the enclosed envelope.
OMB No. 0584-NEW
Expiration date: XX/XXXX
See OMB statement on inside cover
Survey on What You Eat
|
|
Thank you for taking part in this important study!
Please fill out and return the survey in the enclosed envelope within the next week.
If you have any questions about the Survey on What You Eat, please send an e-mail to xxxx@rti.org or call toll-free at 1-800-xxx-xxxx.
Public reporting burden for this collection of information is estimated to average 15 minutes per response, including the time for reviewing instructions, searching existing data sources, gathering and maintaining the data needed, and completing and reviewing the collection of information.
An agency may not conduct or sponsor, and a person is not required to respond to, a collection of information unless it displays a currently valid OMB control number.
Send comments regarding this burden estimate or any other aspect of this collection of information, including suggestions for reducing this burden, to: U.S. Department of Agriculture, Food and Nutrition Services, Office of Research and Analysis, Room 1014, Alexandria, VA 22302 ATTN: PRA (0584-xxxx*). Do not return the completed form to this address.
If you have questions regarding your rights as a research participant, you may contact RTI’s Office of Research Protection toll-free at 866-214-2043.
Survey
on What You Eat
Mail Questionnaire for Nonrespondents to
Internet Survey
(Post-survey, Control Group)
Instrument for PSU Impact Evaluation
This survey asks about what you eat. This study is being sponsored by the U.S. Department of Agriculture’s Food & Nutrition Service and conducted by RTI International, a non-profit research organization. The survey will take about 10 to 15 minutes to complete. You will receive $15 for completing this survey.
All of your answers to the survey will be kept private. We will not share your answers with anyone. You may skip any questions you do not want to answer. If you have any questions, please call xxx xxxx at RTI International at 1-800-xxx-xxxx.
Questions on Whether Certain Foods Are Available At Home
Were any of the following foods available in your home during the past week? Include fresh, frozen, canned, and dried foods. (Circle yes or no for each food.)
a. Bananas |
Yes |
No |
b. Apples |
Yes |
No |
c. Grapes |
Yes |
No |
d. Carrots |
Yes |
No |
e. Potato chips, nacho chips, or corn chips |
Yes |
No |
f. Regular soft drinks or sodas |
Yes |
No |
g. Diet soft drinks or sodas |
Yes |
No |
h. Regular whole or 2% milk |
Yes |
No |
i. 1% or skim milk |
Yes |
No |
Questions on Foods You Like or Dislike
How much would you say you like or dislike the following foods? (Circle one answer for each food.)
|
Extremely Dislike |
|
|
|
Neither Like or Dislike |
|
|
|
Extremely Like |
|
|
a. Apples |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
b. Oranges |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
c. Orange juice |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
d. Green beans |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
e. Peas |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
f. Raw tomatoes |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
g. Broccoli |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
h. Cauliflower |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
i. Raw carrots |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
j. Tossed green salads |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
k. White bread |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
l. Whole-wheat bread |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
m. Whole milk |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
n. Skim or non-fat milk |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
Questions the Fruits and Vegetables You Eat
For the next questions think about what you actually ate during the past week, or the past 7 days. Do not tell us what you think you should be eating or what you typically eat.
How many days during the past week did you eat fruit or vegetables as snacks? (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
How many days during the past week did you eat more than one kind of fruit each day? Do not include fruit juice. (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
During the past week, how many cups of fruit did you eat each day? Do not include fruit juice. (Circle one.)
1. None
2. 1/2 cup
3. 1 cup
4. 1 ½ cups
5. 2 cups
None
1 cup
2 cups
3 cups
6. 2 ½ cups
7. 3 cups or more
How many days during the past week did you eat more than one kind of vegetable each day? Do not include vegetable juice. (Circle one.)
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
During the past week, how many cups of vegetables did you eat each day? Do not include vegetable juice. (Circle one.)
1. None |
|
||||||
2. 1/2 cup |
|||||||
3. 1 cup |
|||||||
4. 1 ½ cups |
|||||||
5. 2 cups |
None |
|
1 cup |
|
2 cups |
|
3 cups |
6. 2 ½ cups |
|
|
|
|
|
||
7. 3 cups or more |
|
||||||
Questions on the Dairy Products You Eat
Did you drink milk or use milk on cereal during the past week? (Circle one.)
1. Yes
2. No [GO TO QUESTION 10]
What kind of milk did you usually drink or use on cereal during the past week? (Circle one.)
1. Regular whole milk
2. 2% milk
3. 1% milk
4. Skim on non-fat milk
5. Other type of milk (for example, soy or rice)
Other Questions on Your Eating Habits
Do you take the skin off of chicken? (Circle one.)
1. No
2. Yes, often
3. Yes, sometimes
4. Yes, everyday
How would you rate your eating habits? (Circle one.)
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
10 |
poor |
|
|
fair |
|
|
good |
|
|
excellent |
Thank you for completing our survey.
Please return survey in the enclosed envelope.
OMB No. 0584-NEW
Expiration date: XX/XXXX
Survey on What You Eat
Telephone Questionnaire for Nonrespondents to Internet Survey
(Intervention
and Control Groups)
Instrument for PSU Impact Evaluation
To begin the survey, I’m going to read a list of foods. For each food, please tell me if it was available in your home during the past week. Please include fresh, frozen, canned, and dried foods. Answer yes or no for each food. The first food is…
a. Bananas |
YES |
NO |
DK |
RF |
b. Apples |
YES |
NO |
DK |
RF |
c. Grapes |
YES |
NO |
DK |
RF |
d. Carrots |
YES |
NO |
DK |
RF |
e. Potato chips, nacho chips, or corn chips |
YES |
NO |
DK |
RF |
f. Regular soft drinks or sodas |
YES |
NO |
DK |
RF |
g. Diet soft drinks or sodas |
YES |
NO |
DK |
RF |
h. Regular whole or 2% milk |
YES |
NO |
DK |
RF |
i. 1% or skim milk |
YES |
NO |
DK |
RF |
Next, I’m going to read another list of foods. For each food, please tell how much you like or dislike the food using a scale from 1 to 9, where 1 is “extremely dislike,” 5 is “neither like or dislike,” and 9 is “extremely like.” If you have never tried the food or would not try it, please tell me. The first food is… SELECT ONE ANSWER FOR EACH FOOD. REPEAT SCALE IF NECESSARY.
|
Extremely Dislike |
|
|
|
Neither Like or Dislike |
|
|
|
Extremely Like |
|
|
|
|
a. Apples |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
DK |
RF |
b. Oranges |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
DK |
RF |
c. Orange juice |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
DK |
RF |
d. Green beans |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
DK |
RF |
e. Peas |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
DK |
RF |
f. Raw tomatoes |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
DK |
RF |
g. Broccoli |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
DK |
RF |
h. Cauliflower |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
DK |
RF |
i. Raw carrots |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
DK |
RF |
j. Tossed green salads |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
DK |
RF |
k. White bread |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
DK |
RF |
l. Whole-wheat bread |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
DK |
RF |
m. Whole milk |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
DK |
RF |
n. Skim or non-fat milk |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
Never Tried |
Would Not Try |
DK |
RF |
For the next questions think about what you actually ate during the past week, or the past 7 days. Do not tell us what you think you should be eating or what you typically eat.
How many days during the past week did you eat fruit or vegetables as snacks? Would you say…? SELECT ONE.
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
-4. DON’T KNOW
-7. REFUSAL
How many days during the past week did you eat more than one kind of fruit each day? Do not include fruit juice. Would you say…? SELECT ONE.
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
-4. DON’T KNOW
-7. REFUSAL
During the past week, how many cups of fruit did you eat each day? Do not include fruit juice. Would you say you had…? SELECT ONE.
1. No fruit
2. ½ cup
3. 1 cup
4. 1 ½ cups
5. 2 cups
6. 2 ½ cups
7. 3 cups or more
-4. DON’T KNOW
-7. REFUSAL
How many days during the past week did you eat more than one kind of vegetable each day? Do not include vegetable juice. Would you say…? SELECT ONE.
1. None
2. 1 to 2 days
3. 3 to 4 days
4. 5 to 6 days
5. Everyday
-4. DON’T KNOW
-7. REFUSAL
During the past week, how many cups of vegetables did you eat each day? Do not include vegetable juice. Would you say you had…? SELECT ONE.
1. No vegetables
2. ½ cup
3. 1 cup
4. 1 ½ cups
5. 2 cups
6. 2 ½ cups
7. 3 cups or more
-4. DON’T KNOW
-7. REFUSAL
Did you drink milk or use milk on cereal during the past week? SELECT ONE.
1. Yes
2. No [GO TO QUESTION 10]
-4. DON’T KNOW [GO TO QUESTION 10]
-7. REFUSAL [GO TO QUESTION 10]
What kind of milk did you usually drink or use on cereal during the past week? SELECT ONE.
1. Regular whole milk
2. 2% milk
3. 1% milk
4. Skim on non-fat milk
5. Other type of milk (for example, soy or rice)
-4. DON’T KNOW
-7. REFUSAL
Do you take the skin off of chicken? Would you say…? SELECT ONE.
1. No
2. Yes, often
3. Yes, sometimes
4. Yes, everyday
-4. DON’T KNOW
-7. REFUSAL
How would you rate your eating habits using a scale from 1 to 10, where 1 is “poor,” 4 is “fair,” 7 is “good,” and 10 is “excellent?” SELECT ONE.
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
10 |
poor |
|
|
fair |
|
|
good |
|
|
excellent |
-4. DON’T KNOW
-7. REFUSAL
[IF ADMINISTRATION IS CONTROL GROUP THEN GO TO Q21.]
[IF ADMINISTRATION IS INTERVENTION GROUP THEN COMPLETE 12A–15A THEN GO TO Q21.]
[IF ADMINISTRATION IS DROP OUT GROUP THEN COMPLETE 16A–Q23.]
12A. Several weeks ago, you agreed to take part in a study being conducted by the Pennsylvania State University. As part of this study, you were asked to go to the web site called, “About Eating” and complete lessons on eating and exercise. The next questions ask about the “About Eating” program.
The next questions ask about your experience with the “About Eating” program. I’m going to read a list of statements. For each statement, please tell me whether you strongly agree, agree, disagree, or strongly disagree with the statements. The first statement is... SELECT ONE FOR EACH STATEMENT. REPEAT SCALE IF NECESSARY.
|
Strongly Agree |
Agree |
Disagree |
Strongly Disagree |
DK |
RF |
|
1 |
2 |
3 |
4 |
-4 |
-7 |
|
1 |
2 |
3 |
4 |
-4 |
-7 |
|
1 |
2 |
3 |
4 |
-4 |
-7 |
|
1 |
2 |
3 |
4 |
-4 |
-7 |
|
1 |
2 |
3 |
4 |
-4 |
-7 |
|
1 |
2 |
3 |
4 |
-4 |
-7 |
|
1 |
2 |
3 |
4 |
-4 |
-7 |
|
1 |
2 |
3 |
4 |
-4 |
-7 |
|
1 |
2 |
3 |
4 |
-4 |
-7 |
|
1 |
2 |
3 |
4 |
-4 |
-7 |
|
1 |
2 |
3 |
4 |
-4 |
-7 |
|
1 |
2 |
3 |
4 |
-4 |
-7 |
|
1 |
2 |
3 |
4 |
-4 |
-7 |
|
1 |
2 |
3 |
4 |
-4 |
-7 |
|
1 |
2 |
3 |
4 |
-4 |
-7 |
What do you think about the amount of time it took to complete the “About Eating” lessons? Would you say…? SELECT ONE.
1. Too long
2. Too short
3. Just right
-4. DON’T KNOW
-7. REFUSAL
There were a total of five “About Eating” lessons. Please tell me which lesson was your most favorite and which lesson was your least favorite. There was a lesson on… READ LIST. Which lesson was your most favorite? SELECT ONE AND ENTER 1. Which lesson was your least favorite? SELECT ONE AND ENTER 5.
_____ eating different kinds of food
_____ enjoying your food
_____ how to know when you are hungry or full
_____ eating and feeding your family
_____ physical activity
-4. DON’T KNOW
-7. REFUSAL
Please share any comments on the “About Eating” web site.
15A. If you would be willing to talk to us in more detail about your experience with the About Eating program for an additional incentive of $15, please provide your name and telephone number, and we will get in touch with you within the next week, or call us at [INSERT 1-800#] at your earliest convenience.”
Name:
Telephone Number:
[ALL GO TO Q21.]
16A. Several weeks ago, you agreed to take part in a study being conducted by the Pennsylvania State University. As part of this study, you were asked to go to the web site called, “About Eating” and complete lessons on eating and exercise. The next questions ask about the “About Eating” program.
Which lesson(s) did you complete on the “About Eating” web site? READ LIST AND SELECT ALL THAT APPLY.
1. The lesson on eating different kinds of food
2. The lesson on enjoying your food
3. The lesson on how to know when you are hungry or full
4. The lesson on eating and feeding your family
5. The lesson on physical activity
6. I DID NOT COMPLETE ANY OF THE LESSONS
7. I DO NOT REMEMBER WHICH LESSON(S) I COMPLETED
-4. DON’T KNOW
-7. REFUSAL
Why did you decide not to complete all of the lessons? Was it because…? SELECT ALL THAT APPLY.
1. The lessons were not useful
2. The lessons were not interesting
3. The lessons were difficult to read and understand
4. It was difficult to move around the web site
5. The lessons were too long
6. You were too busy with other activities, like work or family
7. You had limited access to Internet/Web or a computer
8. Some other reason (SPECIFY):
-4. DON’T KNOW
-7. REFUSAL
18. The next questions ask about your experience with the “About Eating” program. I’m going to read a list of statements. For each statement, please tell me whether you strongly agree, agree, disagree, or strongly disagree with the statements. The first statement is… SELECT ONE FOR EACH STATEMENT.
|
Strongly Agree |
Agree |
Disagree |
Strongly Disagree |
DK |
RF |
|
1 |
2 |
3 |
4 |
-4 |
-7 |
|
1 |
2 |
3 |
4 |
-4 |
-7 |
|
1 |
2 |
3 |
4 |
-4 |
-7 |
|
1 |
2 |
3 |
4 |
-4 |
-7 |
|
1 |
2 |
3 |
4 |
-4 |
-7 |
|
1 |
2 |
3 |
4 |
-4 |
-7 |
|
1 |
2 |
3 |
4 |
-4 |
-7 |
|
1 |
2 |
3 |
4 |
-4 |
-7 |
|
1 |
2 |
3 |
4 |
-4 |
-7 |
|
1 |
2 |
3 |
4 |
-4 |
-7 |
|
1 |
2 |
3 |
4 |
-4 |
-7 |
|
1 |
2 |
3 |
4 |
-4 |
-7 |
|
1 |
2 |
3 |
4 |
-4 |
-7 |
|
1 |
2 |
3 |
4 |
-4 |
-7 |
|
1 |
2 |
3 |
4 |
-4 |
-7 |
19. What do you think about the amount of time it took to complete the “About Eating” lessons? Would you say…? SELECT ONE.
1. Too long
2. Too short
3. Just right
-4. DON’T KNOW
-7. REFUSAL
20. Please share any comments on the “About Eating” web site.
21. That is all the questions I have. Thank you for completing our survey. Before saying goodbye, I’d like to confirm that I have your correct name and address for sending your cash incentive in appreciation for completing this survey. I have [RESPONDENT NAME] spelled _____________________. Is this correct?
YES
CORRECT NAME [PROGRAMMER – SET UP TO ENTER CORRECTIONS]
-7. REFUSAL
22. For your street address, I have [RESPONDENT STREET ADDRESS] Is this correct?
YES
NO [PROGRAMMER – SET UP TO ENTER CORRECT ADDRESS]
-7. REFUSAL
23. For your city, state, and zip code, I have [RESPONDENT CITY, STATE, ZIP CODE] Is this correct?
YES
CORRECT CITY
CORRECT STATE
CORRECT ZIPCODE [PROGRAMMER – SET UP TO ALLOW FOR GENERATION OF ADDRESS LABELS FOR INCENTIVE LETTERS]
-7. REFUSAL
Thank you again. Have a nice (day/evening).
| File Type | application/msword |
| File Title | This attachment provides the instruments for the impact evaluation of the four demonstration projects |
| Author | scc |
| Last Modified By | rgreene |
| File Modified | 2009-10-26 |
| File Created | 2009-10-26 |
© 2026 OMB.report | Privacy Policy