1240-0010 Request to be Selected as Rep Payee CM-910 Justification
Non-Sub Justification 910 2026.docx
Request to be Selected as Payee
1240-0010 Request to be Selected as Rep Payee CM-910 Justification
OMB: 1240-0010
NON- SUBSTANTIVE CHANGE REQUEST FOR THE REQUEST TO BE SELECTED AS PAYEE
OMB CONTROL NO. 1240-0010 (January 2026)
DCMWC is requesting a non-substantive change to the approved collection of information contained in the “Request to be Selected as Payee”.
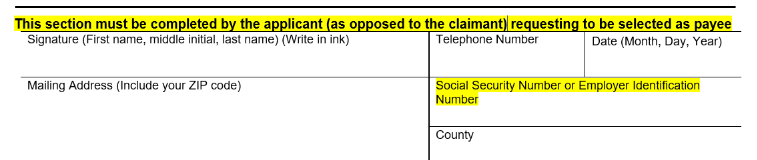
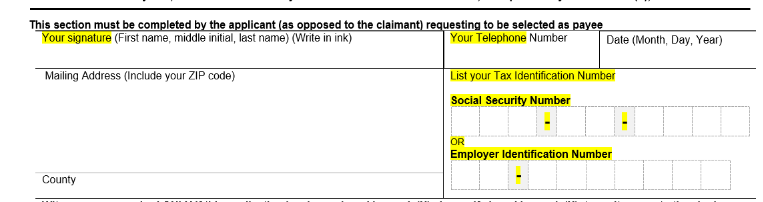
The current CM-910 form has a designated box for the Representative Payee applicants to provide their SSN. Roughly 60% of the applicants list the claimant's or miner's SSN instead of the applicants. A recent program data analysis revealed that we continue to have issues trying to capture the correct information. DCMWC is adding check boxes to help the applicant answer the questions easier as well as a new format control to identify which type of number is being provided (SSN or EIN). Additionally, we added the word “Your” before the Signature and the Telephone number to assist the responder.
Please see below the changes:
Old Form: Signature of Applicant
New Form language:
Other changes:
S# |
Question/Form Area/Controls |
Change Implemented |
1 |
Question 4b |
Options ___ replaced with Checkbox Spacing adjusted to increase space to enter Bank Name |
2 |
Question 5 |
Option |___| replaced with Checkbox |
3 |
Question 5a |
Option |___| replaced with Checkbox |
4 |
Public Burden Statement Area on Page 1 |
Adjust spacing to improve readability |
5 |
Question 6 |
Option |___| replaced with Checkbox |
6 |
Question 7 |
Option |___| replaced with Checkbox |
7 |
Question 8 |
Option |___| replaced with Checkbox |
8 |
Question 9 |
Option |___| replaced with Checkbox |
9 |
Question 10 |
Option |___| replaced with Checkbox |
10 |
Question 11 |
Option |___| replaced with Checkbox |
11 |
Question 12 |
Option |___| replaced with Checkbox |
12 |
Witnesses are required ONLY on Page 2 |
The statement now occupies the full length of the page |
It is the Program (DCMWC) discretion, to update the instructions on form to obtain the applicants’ SSN number or EIN number, in order to aid our course of business.
This change request does not affect the burden hours. The burden hours remain the same.
The revised form is attached to this change request.
| File Type | application/vnd.openxmlformats-officedocument.wordprocessingml.document |
| File Title | SUPPORTING STATEMENT FOR THE |
| Author | OSHA_User |
| File Modified | 0000-00-00 |
| File Created | 2026-01-13 |
© 2026 OMB.report | Privacy Policy