Questionnaire
Generic Clearance for Questionnaire Pretesting Research
NHIS Questionnaire (Attachment III)
National Health Interview Survey (NHIS) cognitive testing
OMB: 0607-0725
NHIS Cognitive Testing Questionnaire
Roster
INTRO - Welcome to the National Health Interview Survey. Please answer the following questions to determine who in your household will be selected for an interview.
VERADD – Your address is listed as:
[PROVIDE ADDRESS]
Is this your exact address?
Yes
No
RESCHECK – Do you live at this address?
Yes
No
AGECHECK - Are you at least 18 years old
Yes
No
NAME_FNAME – Including yourself, are the names of all the people living or staying at this address?
“Add person” button
The following people are listed as living at this address:
[NAME LIST]
MISPERS_MCHILD - Are there any babies or small children missing from this list?
Yes
No
If “Yes” to MISPERS_MCHILD, display the following below.
MISPERS_MCHILD_ADD-Enter the name(s) and then click Next.
![]()
“Add person” button
MISPERS_MSCHOOL - Are there any people who usually live here, but are away now at school or college?
[NAME LIST]
Yes
No
If “Yes” to MISPERS_MSCHOOL, display the following below.
MISPERS_MSCHOOL_ADD-Enter the name(s) and then click Next.
![]()
“Add person” button
MISPERS_MELSE - Are there any people who usually live here, including people who are not related to you or people who are away traveling?
[NAME LIST]
Yes
No
If “Yes” to MISPERS_MELSE, display the following below.
MISPERS_MELSE_ADD-Enter the name(s) and then click Next.
![]()
“Add person” button
USUALRES – Does everyone on this list usually live or stay at this address?
[NAME LIST]
Yes
No
IF “NO” TO USUALRES
USUALRES_NOT – Please select the individuals who do NOT usually stay or live at this address
Select all that apply
[NAMELIST] --- new list FINAL_NAMELIST generated after this question
HHRESP
From the list below, who would you say could answer questions about all members of this household? Select all the apply.
[NAMES]
[checkbox] No one on this list fits this description.
[Demographics --- For testing, we will cycle through the demographics by each person in the roster.]
SEX - Some of the questions in this survey are about topics like breast and prostate cancer, so it is important to know which questions apply. [Are you/Is NAME] male or female?
Male
Female
AGE – What is [your/NAME] age?
[UNIT] [PERIOD]
EDUC - What is the highest level of school [you have/NAME has] completed or the highest degree [you have/NAME has] received?
Never attended/kindergarten only
Grade 1-11
12th grade, no diploma
GED or equivalent
High school graduate
Some college, no degree
Associate degree: occupational, technical, or vocational program
Associate degree: academic program
Bachelor’s degree (Example: BA, AB, BS, BBA)
Master’s degree (Example: MA, MS, MEng, MEd, MBA)
Professional School degree (Example: MD, DDS, DVM, JD)
Doctoral degree (Example: PhD, EdD)
WHOPAR
[if person less than 18 in the household]
Which people living in this household are [NAME} parents?
Please include biological, step, adoptive, or foster parents or other relatives who may act as parents.
Select all that apply.
[NAME LIST]
No biological, step, adoptive, or foster parents
ALLFAM – You have been selected to participate in the National Health Interview Survey
Is everyone in the list above a member of the same family?
Yes
No [go to WHOFAM]
WHOFAM – Please select the individuals from the household who are members of your family.
Select all that apply.
[FINAL_NAMELIST]
Cardiovascular Conditions
Have you ever been told by a doctor or other health professional that you had…
|
Yes |
No |
|
|
|
|
|
|
|
|
|
|
|
|
Cancer
CANEV_A
Have you ever been told by a doctor or other health professional that you had cancer or a malignancy of any kind?
Yes
No
If yes, go to CANKIND1_A
If no, end section.
CANKIND1_A
What kind of cancer was it?
[drop down of answers of the following]
Bladder
Blood
Bone
Brain
Breast
Cervix/Cervical
Colon
Esophagus/Esophageal
Gallbladder
Kidney
Larynx-trachea
Leukemia
Liver
Lung
Lymphoma
Melanoma
Mouth/tongue/lip
Ovary/Ovarian
Pancreas/Pancreatic
Prostate
Rectum
Skin (melanoma)
Skin (non-melanoma)
Skin (don’t know kind)
Stomach
Testis/testicular
Throat-pharynx
Thyroid
Uterus/Uterine
Other (specify-[write in field])
All answers go to CANAGE1_A
CANAGE1_A
How old were you when a doctor or other health professional first told you that you had this cancer?
[range of values]
All answers go to CANKIND2_Part1_A
CANKIND2_Part1_A
Have you ever had any other kinds of cancer?
Yes
No
If yes, go to CANKIND2_Part2_A
CANKIND2_Part2_A
[drop down of answers of the following]
Bladder
Blood
Bone
Brain
Breast
Cervix/Cervical
Colon
Esophagus/Esophageal
Gallbladder
Kidney
Larynx-trachea
Leukemia
Liver
Lung
Lymphoma
Melanoma
Mouth/tongue/lip
Ovary/Ovarian
Pancreas/Pancreatic
Prostate
Rectum
Skin (melanoma)
Skin (non-melanoma)
Skin (don’t know kind)
Stomach
Testis/testicular
Throat-pharynx
Thyroid
Uterus/Uterine
Other (specify-[write in field])
Diabetes
PREDIB_A
Has a doctor or other health professional ever told you that you had prediabetes or borderline diabetes?
Yes
No
If female, go to GESDIB_A, else go to DIBEV_A
GESBIB_A
Has a doctor or other health professional EVER told you that you had gestational diabetes, a type of diabetes that occurs ONLY during pregnancy?
Gestational diabetes is diabetes that you did not have prior to being pregnant and goes away after you are pregnant. Pregnant women are usually screened for gestational diabetes during the 24th to 28th week of pregnancy.
Yes
No
All answers go to DIBEV_A
DIBEV_A
Has a doctor or other health professional EVER told you that you had diabetes?
Do not include gestational diabetes or prediabetes.
Yes
No
If yes, go to DIBAGE_A
If no, if PREDIB_A=yes, go to DIBPILL_A
Else if PREDIB_A=no, go to cancer section
DIBAGE_A
How old were you when a doctor or other health professional FIRST told you that you had diabetes? Do not include gestational diabetes or prediabetes.
[Enter value]
Goto DIBPILL_A
DIBPILL_A
Are you NOW taking diabetic pills to lower your blood sugar?
These are sometimes called oral agents or oral hypoglycemic agents.
Yes
No
All answers go to DIBINS_A
DIBINS_A
Are you NOW taking insulin?
Insulin can be taken by shot or pump.
Yes
No
DIBGLP_A_V1
[If DIBINS_A=”Yes”]
Other than insulin, are you now taking any injectable medications to lower your blood sugar or lose weight?
Yes
No
DIBGLP_A_V2
[If DIBINS_A=”No”]
Are you taking any injectable medications to lower your blood sugar or lose weight?
Yes
No
DIBTYPE_A
According to your doctor or other health professional, what type of diabetes do you have?
Type 1
Type 2
Other type of diabetes
Don’t remember
Other Chronic Conditions
Have you ever been told by a doctor or other health professional that you had…
|
Yes |
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Health Insurance
Color Key:
General Question and Probes/Single Service Plans
Medicare
Medicaid
Private Health Plan
State Sponsored Health Plan
Other Government Program
Military Health Care
Uninsurance

Name: HICOVKIND_A
Universe Description: Sample Adults 18+
Question Text:
.
What kinds of health insurance or health care coverage do you have, if any?
Include health insurance obtained through employment or purchased directly as well as government programs like Medicare, Medicaid, that provide medical care or help pay medical bills.
Select all that apply
1 Private health insurance
2 Medicare (including Medicare Advantage)
3 Medicare supplement (Medigap)
4 Medicaid
5 Military related health care: TRICARE (CHAMPUS) / VA health care / CHAMP-VA
_________________________________________________________________________________
6 Indian Health Service
7 State-sponsored health plan
8 Other government program
9 I do not have health insurance or health care coverage
Skip Instructions: If age is 65+ and HICOVKIND is not 2 or 3, ask MCAREPRB prior to HINOTYR; if age is <65 and HICOVKIND is not 4, ask MCAIDPRB prior to HINOTYR
Else [goto SINCOVDE_A]
Name: MCAREPRB_A
Universe Description: Sample Adults 65+ who have not indicated they had Medicare in HIKIND_A
Question Text:
Are you covered by Medicare?
1 Yes
2 No
Skip Instructions: <1,2,RF,DK> [goto SINCOVDE_A]
Name: MCAIDPRB_A
Universe Description: Sample Adults 18-64 who have indicated they are uninsured, refused, or don't know their type of health insurance
Question Text:
.
^STATEMA Are you covered by Medicaid?
Medicaid is a program that pays for health care for persons in need.
1 Yes
2 No
Skip Instructions: <1,2,RF,DK> [goto SINCOVDE_A]
Name: SINCOVDE_A, SINCOVVS_A, SINCOVRX_A
Universe Description: Sample Adults 18+
Question Text:
In addition to other plans selected, are you covered by a separate plan that only pays for any of the following?
Select all that apply.
Dental services
Vision services
Prescriptions
*.
Skip Instructions: <1-3,RF,DK> [go to applicable section]
Name: MCPART_A
Universe Description: Sample Adults 18+ with Medicare
Question Text:
What type of Medicare coverage do you have?
1 Part A- hospital only
2 Part B- medical only
3 Both Part A and Part B
Skip Instructions: <1> [goto MCPARTD_A]
<2-3,RF,DK> [goto MCCHOICE_A]
Name: MCCHOICE_A
Universe Description: Sample Adults 18+ with Medicare that have part B Medicare or don't know or refused if they have part B Medicare
Question Text:
Are you enrolled in a Medicare Advantage plan?
1 Yes
2 No
Skip Instructions: <1,2,RF,DK> [goto MCHMO_A]
Name: MCHMO_A
SAS Name: MCHMO_A
Universe Description: Sample Adults 18+ with Medicare that have part B Medicare or don't know or refused if they have part B Medicare
Question Text:
Are you under a Medicare managed care arrangement, such as a Health Maintenance Organization (HMO)?
1 Yes
2 No
Skip Instructions: <1> [goto MCANAME_A]
<2,RF,DK> if MCCHOICE_A=1 [goto MCANAME_A] elseif MCCHOICE_A IN (2,RF,DK) [goto MCPARTD_A]
Name: MCANAME_A
Universe Description: Sample Adults 18+ with a Medicare Advantage plan or a Medicare managed care
arrangement
Question Text: What is the name of your Medicare Advantage or Medicare HMO plan?
ADD IN TEXT FIELD HERE
Skip Instructions: <allow 80,RF,DK> [goto applicable section]
Name: MACHMN_A
Universe Description: Sample Adults 18+ with Medicaid coverage
Question Text:
What is the name of your Medicaid health plan?
ADD IN TEXT FIELD HERE
Skip Instructions: <allow 80,RF,DK> [goto MAXCHNG_A]
Name: MAXCHNG_A
Universe Description: Sample Adults 18+ with Medicaid coverage
Question Text:
Was your Medicaid obtained through Healthcare.gov or the Health Insurance Marketplace?
1 Yes
2 |
|
No |
Skip Instructions: <1,2,RF,DK> [goto MAPREM_A]
Name: MAPREM_A
Universe Description: Sample Adults 18+ with Medicaid coverage
Question Text:
Do you or a family member pay a premium for this Medicaid plan?
A health insurance premium is the amount you or a family member pay each month for health care coverage.
1 Yes
2 No
Skip Instructions: <1,2,RF,DK> [goto MADEDUC_A]
Name: MADEDUC_A
Universe Description: Sample Adults 18+ with Medicaid coverage
Question Text:
Does your Medicaid plan have an annual deductible?
A deductible is the amount you have to pay for health care before your health insurance or health coverage plan will start paying your medical bills.
1 |
|
Yes |
2 |
|
No |
Skip Instructions: <1> [goto MAHDHP_A]
<2,RF,DK> [goto next relevant section]
Name: MAHDHP_A
Universe Description: Sample Adults 18+ with Medicaid coverage who have a deductible
Question Text:
Is the annual deductible for medical care for this plan less than$1650 or $1650 or more?
If there is a separate deductible for prescriptions drugs, hospitalization, or out of network care, do not include those deductible amounts here.
__________________________________________________________________________________________
1 Less than $1650
2 $1650 or more
Skip Instructions: <1,2,RF,DK> [goto next relevant section]
else [goto HINOTYR_A]
Name: HIPNAM1_A
Universe Description: Sample Adults 18+ enrolled in a Medigap plan or private health insurance
Question Text:
What is the complete name of your private health insurance plan? .
Do NOT include plans that only provide extra cash while in the hospital or plans that pay for only one type of service such as long term care, accidents, or dental care.
ADD TEXT FIELD HERE
Skip Instructions: <allow 80,RF,DK> [goto MORPLAN_A]
Name: MORPLAN_A
Universe Description: Sample Adults 18+ enrolled in a private health plan where the name of the plan was given or don't know or refused or the sample adult only shared one private plan with the Sample Child.
Question Text:
Are you covered by any other private health insurance plans?
1 Yes
2 No
Skip Instructions: <1> [goto HIPNAM2_A]
<2,RF,DK> [goto next relevant plan]
else [goto HINOTYR_A]
Name: HIPNAM2_A
Universe Description: Sample Adults 18+ with a second private health insurance plan
Question Text:
What is the name of that private health insurance plan?
Read if necessary: Do you have a health
plan card or something with the plan name on it?
ADD TEXT FIELD HERE
Skip Instructions: <allow 80,RF,DK> [goto bPlan[1].POLHLD_A]
Name: POLHLD_A
Universe Description: Sample Adults 18+ with private health insurance coverage where a plan name was given or refused or don't know.
Question Text:
Are you the policyholder for this plan?
Health insurance plans are usually obtained in one person’s name even if other family members are covered by that plan. That person is called the policy holder.
___________________________________________________________________________________________
1 Yes
2 No
Skip Instructions: <1,RF,DK> [goto PRPLCOV_A]
<2> [goto PRPOLH_A]
Name: PRPLCOV_A
Universe Description: Sample Adults 18+ with private health insurance coverage where a plan name was given or refused or don't know and where the Sample Adult is the policyholder or refused or don't know
Question Text Does this plan cover someone other than yourself?
1 Yes
2 No
Skip Instructions: <1,2,RF,DK> [goto PLNWRK_A]
Name: PLNWRK_A
Universe Description: Sample Adults 18+ with private health insurance coverage where a plan name was given or refused or don't know
Question Text:
Which one of these categories best describes how this plan was obtained?
1 Through an employer, union, or professional association
2 Purchased directly
3 Through Healthcare.gov or the Affordable Care Act (Obamacare)
4 Through a state or local government or community program
5 Other, please specify: [write-in]
Skip Instructions: <1,3> [goto PLNPAY_A]
<2,4,RF,DK> [goto PLNEXCHG_A]
<5> [goto PLNWKSP_A]
Name: PLNEXCHG_A
Universe Description: Sample Adults 18+ with private health insurance coverage where a plan name was given or refused or don't know that is directly purchased, or obtained through a state, local, government or community program, or obtained another way, or refused/don't know how obtained
Question Text:
Was the plan obtained through Healthcare.gov or the Health Insurance Marketplace?
1 Yes
2 No
Skip Instructions: <1,2,RF,DK> [goto PLNPAY_A]
Name: PLNPAY_A
Universe Description: Sample Adults 18+ with private health insurance coverage where a plan name was given or refused or don't know.
Question Text: Who pays for this health insurance plan?
Select all that apply
1 |
|
Self or family (living in the household) |
2 |
|
Employer or union |
3 |
|
Someone outside the household |
4 |
|
Medicare |
5 |
|
Medicaid |
6 |
|
Other government program |
Skip Instructions: if <1> IN PLNPAY_A [goto HICOSTN_A]
else if <2-6> IN PLNPAY_A or PLNPAY_A IN (RF,DK)[goto PRDEDUC_A]
Name: HICOSTN_A
Universe Description: Sample Adults 18+ with private health insurance coverage where a plan name was given or refused or don't know who paid for by self or family
Question Text:
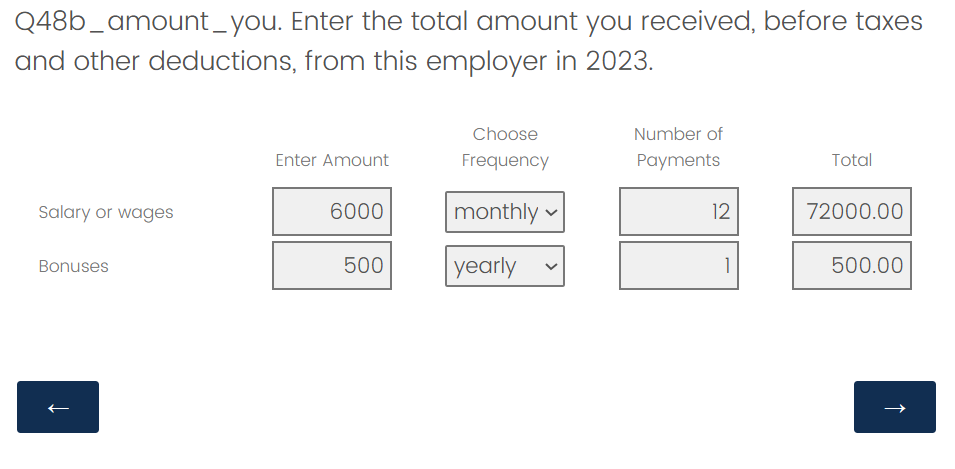
How much (Do you/Does your family) currently spend for health insurance premiums for (name of health insurance plan)? .
Please include payroll deductions for premiums.
ADD FILL-IN TABLE WITH DROP DOWNS FOR REPORTING:
Name of plan (Fill In)
Payment amount (Fill In)
Frequency (Drop down)
See example below (from CPS ASEC):
Skip Instructions: <20000-99995> [goto ERR1_HICOSTN_A]
<1-19999> [goto HICOSTT_A]
<RF,DK> [goto PRDEDUC_A]
Name: PRDEDUC_A
Universe Description: Sample Adults 18+ with private health insurance plans where a plan name was
given or refused or don't know.
Question Text:
Does this health plan have an annual deductible?
A deductible is the amount you have to pay for health care before your health insurance or health coverage plan will start paying your medical bills.
1 Yes
2 No
Skip Instructions: <1> [goto PRHDHP_A]
<2,RF,DK> [goto INTROCOV_A]
Name: PRHDHP_A
Universe Description: Sample Adults 18+ with private health insurance coverage where a plan name was given or refused or don't know with a deductible
Question Text:
Is the annual deductible for medical care for [NAME OF PLAN]:.
If there is a separate deductible for prescription drugs, hospitalization, or out-of-network care, do not include those deductible amounts here.
1 Less than ($1650/$3300)
2 ($1650/$3300) or more
Skip Instructions: <1> [goto INTROCOV_A]
<2,RF,DK> [goto HSAHRA_A]
Name: HSAHRA_A
Universe Description: Sample Adults 18+ with private health insurance coverage where a plan name was given or refused or don't know with a high deductible
Question Text:
Does this plan include any special accounts or funds that can be used to pay for medical expenses, not including Flexible Spending Accounts (FSAs)?
These special accounts or funds are sometimes referred to as Health Savings Accounts (HSAs), Health Reimbursement Accounts (HRAs), Personal Care accounts, Personal Medical funds, or Choice funds.
1 Yes
2 No
Skip Instructions: <1,2,RF,DK> [goto INTROCOV_A]
Name: INTROCOV_A
Universe Description: Sample Adults 18+ with private health insurance coverage where the name of the plan was given or refused or don't know
Question Text: Does this plan pay for any of the following?
Select all that apply (even if only some costs are covered)
Medications prescribed by a doctor or other health professional?
Dental care?
Routine vision care, such as glasses and contact lenses?
Skip Instructions: <1-3,RF,DK> [goto next relevant type of health insurance]
else [goto HINOTYR_A]
Name: OPNAME_A
Universe Description: Sample Adults 18+ with a state-sponsored plan
Question Text:
What is the name of the state-sponsored plan you are covered by?
ADD TEXT FIELD HERE
Skip Instructions: <allow 80,RF,DK> [goto OPXCHNG_A]
Name: OPXCHNG_A
Universe Description: Sample Adults 18+ with a state-sponsored plan
Question Text:
Was your state-sponsored plan obtained through Healthcare.gov or the
Health Insurance Marketplace?
_______________________________
1 Yes
2 No
Skip Instructions: <1,2,RF,DK> [goto OPPREM_A]
Name: OPPREM_A
Universe Description: Sample Adults 18+ with a state-sponsored plan
Question Text:
Do you or a family member pay a health insurance premium for this state-sponsored plan?
A health insurance premium is the amount you or a family member pay each month for health care coverage.
1 Yes
2 No
Skip Instructions: <1,2,RF,DK> [goto OPDEDUC_A]
Name: OPDEDUC_A
Universe Description: Sample Adults 18+ with a state-sponsored plan
Question Text:
Does your state-sponsored plan have an annual deductible?
A deductible is the amount you have to pay for health care before your health insurance or health coverage plan will start paying your medical bills.
1 |
|
Yes |
2 |
|
No |
Skip Instructions: <1>[goto OPHDHP_A]
<2,RF,DK> [go to next relevant health insurance plan]
else [goto HINOTYR_A]
Name: OPHDHP_A
Universe Description: Sample Adults 18+ with a state-sponsored plan with a deductible
Question Text:
Is the annual deductible for medical care for this state-sponsored plan:
If there is a separate deductible for prescription drugs, hospitalization, or out-of-network care, do not include those deductible amounts here.
1 Less than $1650
2 $1650 or more
Skip Instructions: <1,2,RF,DK> [goto next relevant health insurance plan]
else [goto HINOTYR_A]
Name: OGNAME_A
Universe Description: Sample Adults 18+ who have an other government plan
Question Text:
What is the name of the other government plan that you are covered by?
ADD TEXT FIELD HERE
Skip Instructions: <allow 80,RF,DK> [goto OGXCHNG_A]
Name: OGXCHNG_A
Universe Description: Sample Adults 18+ who have an other government plan
Question Text:
Was your other government plan obtained through Healthcare.gov or the
Health Insurance Marketplace?
1 Yes
2 No
Skip Instructions: <1,2,RF,DK> [goto OGPREM_A]
Name: OGPREM_A
Universe Description: Sample Adults 18+ who have an other government plan
Question Text:
Do you or a family member pay a premium for your other government plan?
A health insurance premium is the amount you or a family member pays each month for health care coverage.
1 Yes
2 No
Skip Instructions: <1,2,RF,DK> [goto OGDEDUC_A]
Name: OGDEDUC_A
Universe Description: Sample Adults 18+ with an other government plan
Question Text:
Do you or a family member pay an annual deductible for this other government plan?
A deductible is the amount you have to pay for health care before your health insurance or health coverage plan will start paying your medical bills.
1 Yes
2 No
Skip Instructions: <1> [goto OGHDHP_A]
<2,RF,DK> [goto next relevant health insurance plan]
else [goto HINOTYR_A]
Name: OGHDHP_A
Universe Description: Sample Adults 18+ with an other government plan with a deductible
Question Text:
Is the annual deductible for medical care for this other government plan:
If there is a separate deductible for prescription drugs, hospitalization, or out-of-network care, do not include those deductible amounts here.
1 Less than $1650
2 $1650 or more
Skip Instructions: <1,2,RF,DK> [goto next relevant health insurance plan] else [goto HINOTYR_A]
Name: MILSPC_A
Universe Description: Sample Adults 18+ with military related health care
Question Text:
What types of military related health care are you covered by?
Select all that apply
1 |
|
VA health care |
2 |
|
TRICARE (CHAMPUS) |
3 |
|
CHAMP-VA (do not include CHAMPUS) |
Skip Instructions: <1-3,RF,DK> [goto HINOTYR_A]
Name: HILAST_A
Universe Description: Sample Adults 18+ without known health insurance and answered no, refused
ordon't know to the Medicaid probe or the Medicare probe.
Question Text: About how long has it been since you last had health care coverage that paid for doctor's
visits or hospital stays?
1 |
|
Less than 12 months ago |
2 |
|
1 year ago or more, but less than 2 years ago |
3 |
|
2 years ago or more but less than 3 years ago |
4 |
|
3 years ago or more but less than 5 years ago |
5 |
|
5 years ago or more but less than 10 years ago |
6 |
|
10 years ago or more |
7 |
|
Never have had this type of health care coverage. |
Skip Instructions: <1> [goto HILASTMY_A]
<2,3> [goto HISTOPJOB_A]
<4,5,6,0,RF,DK> [goto RSNHICOST_A]
Name: HILASTMY_A
Universe Description: Sample Adults 18+ without known health insurance who last had insurance at some time within the last 12 months
Question Text: In the past 12 months, how many months were you without coverage?
.
If less than 1 month, enter ‘1’.
ADD TEXT FIELD HERE
Skip Instructions: <1-12,RF,DK> [goto HISTOPJOB_A]
Name: HISTOPJOB_A, HISTOPMISS_A, HISTOPAGE_A, HISTOPCOST_A, HISTOPELIG_A
Universe Description: Sample Adults 18+ who have been uninsured for less than 3 years
Question Text: What are the reasons your last health care coverage ended?
Select all that apply
I (or the policyholder) retired, lost a job, or changed employers.
I missed a deadline for signing up or paying for the coverage.
I became ineligible because of my age or because I left school.
The cost for my coverage increased.
I had Medicaid or other public coverage, but was no longer eligible.
Other, please specify: [text field]
Skip Instructions: <1-5,RF,DK> [goto RSNHICOST_A]
__________________________________________________________________________________________
Name: RSNHICOST_A
Universe Description: Sample Adults 18+ without known health insurance and answered no, refused or don't know to the Medicare probe or the Medicaid probe.
Question Text: If HILAST_A IN (1,2,3) fill: Are you currently uninsured for any of the following reasons?
Select all that apply
Coverage is not affordable
I do not need or want coverage.
The process of signing up for coverage is too difficult or confusing.
I cannot find a plan that meets my needs.
I have applied for coverage, but it has not started yet.
Other, please specify [write-in field]
<1,2,RF,DK> [goto RSNHIWANT_A]
___________________________________________________________________________________________
Name: HINOTYR_A
Universe Description: Sample Adults 18+ with known health insurance coverage or responded yes to the medicare probe or medicaid probe
Question Text: In the past 12 months, was there any time when you did NOT have health insurance or coverage?
1 Yes
2 No
Skip Instructions: <1> [goto HINOTMYR_A]
<2,RF,DK> [goto FINISH_A]
Name: HINOTMYR_A
Universe Description: Sample Adults 18+ with known health insurance coverage and did not have health insurance for some period of time in the past 12 months
Question Text: In the past 12 months, about how many months were you without coverage?
If less than 1 month, enter ‘1’.
ADD TEXT FIELD HERE.
Skip Instructions: <1-12,RF,DK> [goto next section]
Utilization
LASTDR_A
Not including dental care, about how long has it been since you last saw a doctor or other health professional in person about your health?
Include doctors seen if you were a patient in a hospital.
Less than 12 months ago
1 year ago or more but less than 2 years ago
2 years ago or more but less than 3 years ago
3 years ago or more but less than 5 years ago
5 years ago or more but less than 10 years ago
10 years ago or more
Never have seen a doctor or other health professional about my health in person.
WELLNESS_A
(Direct here if LASTDR_A != “NEVER”)
Was this a wellness visit, physical, or general purpose check-up?
Yes
No
WELLVIS_A
(Direct here if WELLNESS_A = “NO”)
About how long has it been since you last saw a doctor or other health professional for a wellness visit, physical, or general purpose check-up?
Less than 12 months ago
1 year ago or more but less than 2 years ago
2 years ago or more but less than 3 years ago
3 years ago or more but less than 5 years ago
5 years ago or more but less than 10 years ago
10 years ago or more
Never have seen a doctor or other health professional for a wellness visit, physical, or general purpose check-up.
USUALPL_A
Is there a place that you usually go to if you are sick and need health care?
Yes, there is a single place.
Yes, there is more than one place
No, there is no place
USPLKIND_A_V1
[Direct here if USUALPL_A=”Yes, there is a single place”]
What kind of place is this?
A doctor’s office or health center
Urgent care center or clinic in a drug store or grocery store
Hospital emergency room
A VA Medical Center or VA outpatient clinic
Some other place
USPLKIND_A_V2
[Direct here if USUALPL_A=”Yes, there is more than one place”]
What kind of places do you go to most often?
Select all that apply.
A doctor’s office or health center
Urgent care center or clinic in a drug store or grocery store
Hospital emergency room
A VA Medical Center or VA outpatient clinic
Some other place
RETAILHC12M_A
During the past 12 months, how many times have you gone to a retail health clinic about your health?
Retail health clinics are located in a pharmacy, grocery store, or supercenter.
Range of values 0-96
URGCC12M_A
During the past 12 months, how many times have you gone to an urgent care center about your health?
This is different from a hospital emergency room.
Range of values 0-96
EMERGE12M_A
During the past 12 months, how many times have you gone to a hospital emergency room about your health?
Range of values 0-96
HOSPONGT_A
During the past 12 months, have you been hospitalized overnight?
Do not include an overnight stay in the emergency room.
Yes
No
MEDDL12M_A
During the past 12 months, have you delayed getting medical care because of the cost?
Yes
No
MEDNG12M_A
During the past 12 months, was there any time when you needed medical care, but did not get it because of the cost?
Yes
No
VIRAPP12M_A
During the past 12 months, have you had an appointment with a doctor, nurse, or other health professional by video or by phone?
Yes
No
Immunization
SHTFLU12M_A
During the past 12 months, have you had a flu vaccination, include either a shot or a spray, mist, or drop in the nose?
Yes
No
SHTFLUM_A
[If SHTFLU12M_A=”Yes”]
During what month and year did you receive your most recent flu vaccine?
[DROP DOWN OF MONTHS] [DROP DOWN OF YEARS]
Cigarettes and e-cigarettes
SMKEV_A
Have you smoked at least 100 cigarettes in your entire life?
Do not include using e-cigarettes.
Yes
No
SMKAGE_A
(Direct here if SMKEV_A = Yes)
How old were you when you first started to smoke fairly regularly?
Range of values
SMKNOW_A
(Direct here if SMKEV_A = Yes)
How often do you now smoke cigarettes?
Every day
Some days
Not at all
CIGNOW_A
On average, about how many cigarettes do you now smoke a day?
Range of values 0-95
SMK30D_A
On how many of the past 30 days did you smoke a cigarette?
Range of values 0-30
CIG30D_A
(Direct here if SMK30D_A != 0)
On average, when you smoked during the past 30 days, about how many cigarettes did you smoke a day?
Range of values 1-95
ECIGEV_A
Not including marijuana use, have you ever used an e-cigarette or other electronic vaping product, even just one time, in your entire life?
Yes
No
ECIGNOW_A
(Direct here if ECIGEV_A = Yes)
How often do you now use e-cigarettes or other electronic vaping products?
Every day
Some days
Not at all
Marital Status
MARITAL_A
Which of the following best describes you now?
Married
Living with a partner together as an unmarried couple
Neither
SPOUSLIV_A [IF MARITAL_A = “Married”]
Does your spouse live at this address?
Yes
No
SPOUSEP_A [IF SPOUSLIV_A = “No”]
Does your spouse not live at this address because you and your spouse are legally separated?
Yes
No
SPOUSWHO_A [IF SPOUSLIV_A = “Yes”]
From the list of names below, which person is your spouse?
[NAME LIST INCLUDING EVERYONE 16+]
My spouse isn’t on this list.
PARTNERWHO_A [IF MARITAL_A = “Living with a partner together as an unmarried couple”]
From the list of names below, which person is your partner?
[NAME LIST INCLUDING EVERYONE 16+]
My partner isn’t on this list.
EVRMARRIED_A [IF MARITAL_A = “Neither”]
Have you ever been married?
Yes
No
LEGALSTAT_A [IF EVERMARRIED_A = “Yes” & MARITAL_A = “Living with a partner together as an unmarried couple”]
What is your current legal marital status?
Married
Widowed
Divorced
Separated
WIDIVSEP_A [IF EVERMARRIED_A = “Yes” & MARITAL_A = “Neither]
What is your current legal marital status?
Widowed
Divorced
Separated
| File Type | application/vnd.openxmlformats-officedocument.wordprocessingml.document |
| File Title | NHIS Questionnaire (Attachment III) |
| Author | Jonathan M Katz (CENSUS/CBSM FED) |
| File Modified | 0000-00-00 |
| File Created | 2025-08-12 |
© 2026 OMB.report | Privacy Policy