Anthropometric assessments (child, but accounting for parent's time)
The Community Choice Demonstration
Attachment O_The Obesity & Type II Diabetes Risk Assessment_Anthropometric Assessments_Child
Anthropometric assessments (child, but accounting for parent's time)
OMB: 2528-0337
OMB Clearance Number: 2528-0337
Expires: XX/XX/XXXX
Attachment O: The Obesity & Type II Diabetes Risk Assessment Anthropometric Assessments (Child)
If you require information to be presented in an accessible format or reasonable accommodations to participate in this study, please contact us with any specific requests by calling XXX-XXX-XXXX or emailing XXXX@XXXX.XXX. If you require language assistance to participate in this study, please contact us with any specific language assistance requests or needs.
Paperwork Reduction Act Burden Statement
This collection of information is voluntary and will be used to evaluate the US Department of Housing and Urban Development’s Community Choice Demonstration. Public reporting burden for this collection of information is estimated to average 10 minutes per response, including the time for reviewing instructions, gathering, and maintaining the data needed, and reviewing the collection of information. An agency may not conduct or sponsor, and a person is not required to respond to, a collection of information unless it displays a currently valid OMB control number. The OMB number for this collection is OMB 2528-0337 which expires on XX/XX/XXXX. Send comments regarding this burden estimate or any other aspect of this collection of information, including suggestions for reducing this burden to NAME at XXXX@XXXXX.XXX or call XXX-XXX-XXXX.
Privacy Act Statement
Authority: Section 502 of the Housing and Urban Development Act of 1970 (Public Law 91-609) (12 U.S.C. §§ 1701z-1; 1701z-2(d) and (g)).
Purpose: Evaluation of the Community Choice Demonstration (CCD).
Routine Use: The information will be used for the purpose set forth above and may be provided to Congress or other Federal, state, and local agencies, when determined necessary.
Disclosure: Records will be used for research and statistical analysis and will not be used to make decisions that affect the rights, benefits, or privileges of specific individuals.
SORN ID: Community Choice Demonstration Evaluation Data Files, HUD/PDR-09
Note:
Some
study activities are being funded by the National Institute of
Diabetes and Digestive and Kidney Diseases.
Purpose:
To
record child participant’s height, weight and waist
circumference When: Baseline & follow-up
By
whom: Staff |
1- Participant ID#: __ __ __ __ __ __ __ __
2- Date of visit: ___/___/____(mm/dd/yyyy)
Period: Baseline _____ Follow-up _____ |
Physical
Measure Form
Anthropometric Data
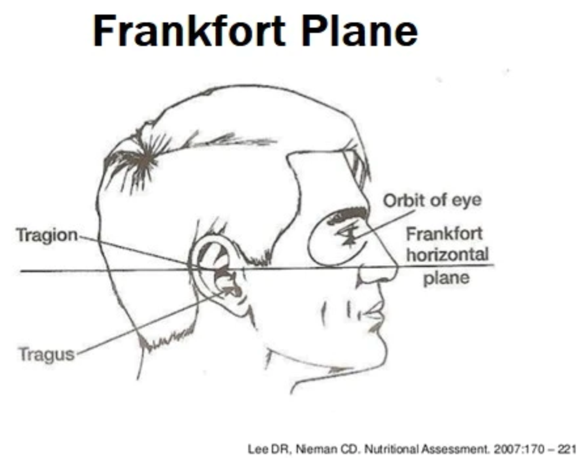
[INTERVIEWER INSTRUCTIONS: Ask the participant to remove their shoes and heavy clothing (if applicable). Ask the participant to stand straight with their back against the wall, head forward, shoulders relaxed. Using a ruler or other straight measurement tool, align the participant’s nose in an imaginary straight line with the tragion or pinna of their ear (see image below for reference). Lower the base of the height meter to the head. If there is a lot of hair, a little pressure should be applied so the height meter touches the head. Mark down the first heigh measurement below. Ask the participant to step off the stadiometer, then step back on and repeat the alignment process to take the second measurement. Do the same for the third measurement, then average the three measurements and mark on the tablet.]
Image
description:
Text at the top of the image reads "Frankfort Plane". Image
displays a diagram of a person's head turned so that the right
profile is visible. Text describes parts of head including Tragion,
orbit of eye, and Tragus and associated lines point to these parts'
location on the head. Text reading "Frankfort horizontal plane"
is placed at the end of a horizontal line which divides the head in
half. Citation reads Lee DR, Nieman CD, Nutritional Assessment,
2007:170 – 221.
Height
First height measurement: __ __ __.__ cm
Second height measurement: __ __ __.__ cm
Third height measurement: __ __ __.__ cm
**Repeat test if the three values
are not within 0.5cm of each other**
[INTERVIEWER
INSTRUCTIONS: Ask the
participant to remove their shoes and heavy clothing (if applicable).
Ask the participant to step on the digital scale and be as still as
possible. Once the measurement is presented on the screen, record the
number in the first weight measurement below. Ask the participant to
step of the scale. Recalibrate the scale to 0.0, then ask the
participant to step on the scale again. Repeat these steps to record
the next two measurements. Average all measurements together and mark
on tablet.]
Weight
First weight measurement: __ __ __._lbs.
Second weight measurement: __ __ __.__lbs.
Third weight measurement: __ __ __.__lbs.
**Repeat test if the three values
are not within 0.1lb of each**
[INTERVIEWER
INSTRUCTIONS: Using a
tension-sensitive, non-elastic tape measure, you will measure the
participant’s waist circumference. To do this, ask the
participant to remove any heavy clothing (if applicable) and breathe
normally. Wrap the tape measure around the participant’s body
just above the hipbones across the umbilicus (bellybutton). Keep the
tape measure snug around the waist, but do not compress the body
(i.e., do not squeeze the tape measure around the participant’s
body). Record the measurement in centimeters where the tape measure
crosses at the bellybutton. Remove the tape measure from the
participant’s body and repeat these steps for the second and
third measurement. Average the three measures together and mark on
the tablet.]
Waist circumference
First waist measurement: __ __ __.__ cm
Second waist measurement: __ __ __.__ cm
Third waist measurement: __ __ __.__ cm
**Repeat test if the three values
are not within 0.5cm of each other**
Entered by:
____________________________ ______________________ _______________________
Staff ID mm/dd/yyyy Signature
|
|
|
| File Type | application/vnd.openxmlformats-officedocument.wordprocessingml.document |
| Author | Ahmed Hassoon |
| File Modified | 0000-00-00 |
| File Created | 2024-10-27 |
© 2026 OMB.report | Privacy Policy