Supporting Statement
CMS-10832 Data Collection ICR 6.29.22.docx
Generic Clearance for the Center for Clinical Standards and Quality IT Product and Support Teams (CMS-10706)
Supporting Statement
OMB: 0938-1397
Request for Approval under the “Generic Clearance for the Center for Clinical Standards and Quality IT Product and Support Teams” (OMB Control Number: 0938-1397)

TITLE OF INFORMATION COLLECTION: Chat/CCSQ Support Central – Basic information questions
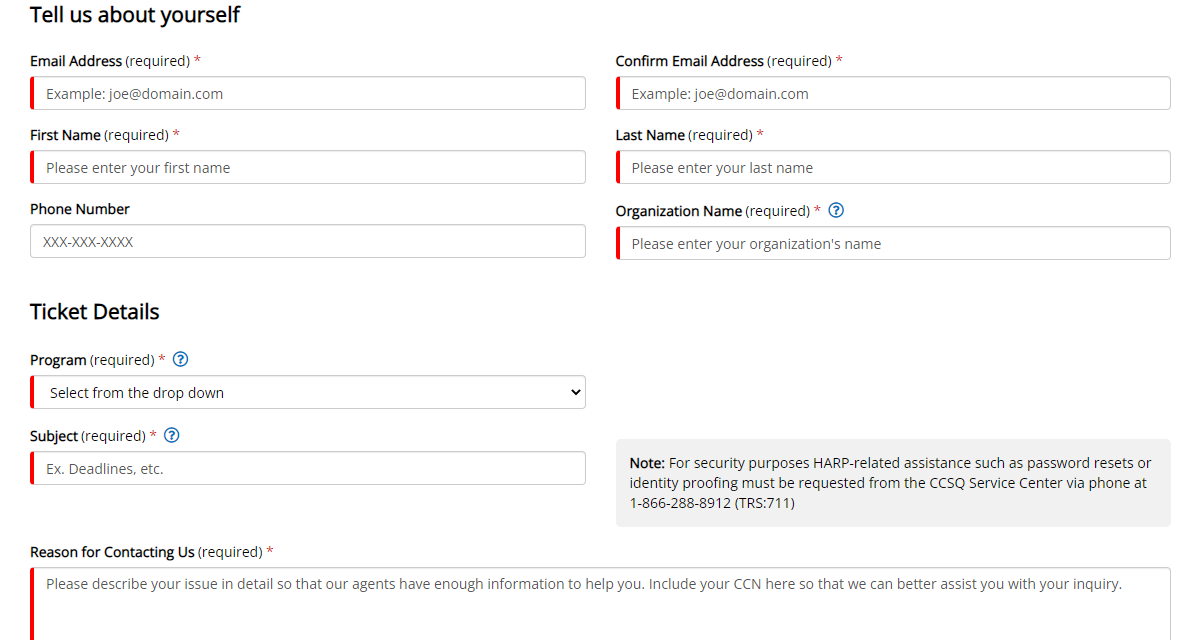
PURPOSE OF COLLECTION: In order to be able to assist our customers who use the “Chat” channel or submit a ticket from the “CCSQ Support Central” website, we need to obtain basic information from the customer to be able to assist them (See attachment and below)
Email address
First/Last name
Organization name
Phone number (optional)
Program (Line of business)
Subject (what do they need help with)
Reason for contacting us
This information will be used to create a ServiceNow ticket (ticketing system) in order to be able to assist and record the customer interaction. The Information will only be housed in ServiceNow which is a FedRAMP approved ticketing system.
TYPE OF COLLECTION: (Check one)
[ ] Card Sorting [ ] Cognitive Testing
[ ] Field Studies [ ] First Click Tests
[ ] Focus Groups [ ] Participatory Design
[ ] Survey [ ] Tree Testing
[ ] User Interviews [ ] Usability Testing
[ X] Other: ____Data collection for ticketing system____
CERTIFICATION:
I certify the following to be true:
The collection is voluntary.
The collection is low-burden for respondents and low-cost for the Federal Government.
The collection is non-controversial and does not raise issues of concern to other federal agencies.
The results are not intended to be disseminated to the public.
Information gathered will not be used for the purpose of substantially informing influential policy decisions.
The collection is targeted to the solicitation of opinions from respondents who have experience with the program or may have experience with the program in the future.
Name: ______Brett Carter________
To assist review, please provide answers to the following question:
PERSONALLY IDENTIFIABLE INFORMATION
Is personally identifiable information (PII) collected? [ X] Yes [ ] No
If Yes, will any information that is collected be included in records that are subject to the Privacy Act of 1974? [ ] Yes [X ] No
If Yes, has an up-to-date System of Records Notice (SORN) been published? [ ] Yes [ ] No
GIFTS OR PAYMENTS
Is an incentive (e.g., money or reimbursement of expenses, token of appreciation) provided to participants? [ ] Yes [ X ] No
If Yes, describe:
BURDEN HOURS
Category of Respondent |
No. of Respondents |
Participation Time |
Burden |
CCSQ website Customers |
7,812 |
3 min |
391 hrs |
Chat Customers |
2,343 |
3 min |
117 hrs |
Totals |
10,155 |
|
FEDERAL COST
The estimated annual cost to the Federal government is ______N/A – part of current contract work_
ACTIVITY DETAILS
How will you collect the information? (Check all that apply)
[ X] Web-based or other forms of social media
[ ] Telephone
[ ] In-person
[ ] Other, Explain.
Will interviewers or facilitators be used? [ ] Yes [X ] No
Who will you collect the information from?
The people who will be using the “Chat” feature or requesting assistance from the CCSQ Support Central website are people who would normally call or email the Service Center for assistance with one of the lines of business we support (EQRS, HQR, iQIES and QPP) By adding “Chat” and the customer support website “CCSQ Support Central”, our customers now have 2 additional channels to reach out to the Service Center for assistance. The basic questions we are requiring of them are questions we already require from them when they call or email us for assistance.
How will you ask a respondent to provide this information?
If a customer chooses the “Chat” option, they would be prompted to provide the basic information listed above to be connected to a live Service Center Representative so we can create a ServiceNow ticket for them.
If a customer is requesting assistance from the CCSQ Support Central website, they will be prompted to provide the basic information listed above as soon as they click on “Create Ticket”.
What will the activity look like?
Whether it be by Chat or the CCSQ Support Central website, the customer will be required to provide the basic information listed above in order to receive customer support from a Service Center Representative. Once the basic information is received a Service Center Representative will be able to live chat or chat bot with a customer or communicate by phone/email with a customer who submitted a ticket through the CCSQ Support Central website.
Please provide your question list.
PRA Disclosure Statement
According to the Paperwork Reduction Act of 1995, no persons are required to respond to a collection of information unless it displays a valid OMB control number. The valid OMB control number for this information collection is 0938-XXXX (Expires XX/XX/XXXX). This is a voluntary information collection. The time required to complete this information collection is estimated to average 3minutes per response, including the time to review instructions, search existing data resources, gather the data needed, and complete and review the information collection. If you have comments concerning the accuracy of the time estimate(s) or suggestions for improving this form, please write to: CMS, 7500 Security Boulevard, Attn: PRA Reports Clearance Officer, Mail Stop C4-26-05, Baltimore, Maryland 21244-1850. ****CMS Disclosure**** Please do not send applications, claims, payments, medical records or any documents containing sensitive information to the PRA Reports Clearance Office. Please note that any correspondence not pertaining to the information collection burden approved under the associated OMB control number listed on this form will not be reviewed, forwarded, or retained. If you have questions or concerns regarding where to submit your documents, please contact John Vancil – John.Vancil@cms.hhs.gov.
Please make sure that all instruments, instructions, and scripts are submitted with the request.
When will the activity happen?
Beginning sometime in Q4 2022
Instructions for completing Request for Approval under the “Generic Clearance for the Center for Clinical Standards and Quality IT Product and Support Teams”
TITLE OF INFORMATION COLLECTION: Provide the name of the collection that is the subject of the request (e.g. Comment card for soliciting feedback on xxxx).
PURPOSE: Provide a brief description of the purpose of this collection and how it will be used. If this is part of a larger study or effort, please include this in your explanation.
TYPE OF COLLECTION: Check one box. If you are requesting approval of other instruments under the generic, you must complete a form for each instrument.
CERTIFICATION: Please read the certification carefully. If you incorrectly certify, the collection will be returned as improperly submitted or it will be disapproved.
Personally Identifiable Information: Provide answers to the questions. Note: Agencies should only collect PII to the extent necessary, and they should only retain PII for the period that is necessary to achieve a specific objective.
Gifts or Payments: If you answer yes to the question, please describe the incentive, and provide a justification for the amount.
BURDEN HOURS:
Category of Respondents: Identify who you expect the respondents to be in terms of the following categories: (1) Individuals or Households; (2) Private Sector; (3) State, local, or tribal governments; or (4) Federal Government. Only one type of respondent can be selected per row.
No. of Respondents: Provide an estimate of the Number of respondents.
Participation Time: Provide an estimate of the amount of time required for a respondent to participate (e.g., fill out a survey or participate in a focus group).
Burden: Provide the Annual burden hours: Multiply the number of responses and the participation time and divide by 60.
FEDERAL COST: Provide an estimate of the annual cost to the Federal government.
ACTIVITY DETAILS: Complete each section as described.
If you are conducting a focus group, survey, or plan to employ statistical methods, please provide a description of how you plan to identify your potential group of respondents and how you will select them.
Submit all instruments, instructions, and scripts are submitted with the request.
| File Type | application/vnd.openxmlformats-officedocument.wordprocessingml.document |
| File Title | DOCUMENTATION FOR THE GENERIC CLEARANCE |
| Author | 558022 |
| File Modified | 0000-00-00 |
| File Created | 2024-07-29 |
© 2026 OMB.report | Privacy Policy