GAOS HCP Post-Campaign Web Survey
[NCEZID] Assessment for the Get Ahead of Sepsis Consumer and Healthcare Professional Campaign
GAOS HCP Post-Campaign Web Survey - HCPs
GAOS HCP Post-Campaign Web Survey - HCPs
OMB: 0920-1384

Centers for Disease Control and Prevention
Division of Healthcare Quality Promotion
Get Ahead of Sepsis (GAOS)
HCP Posttest Survey
Prepared for DHQP by CATMEDIA
Table of Contents
classification of Respondents based on their responses to the screener questions 2
SCREENER Ineligibility Message 3
GAOS HCP Screener Begins Here 3
Screener Survey Introduction 5
General Instructions for Programmer 7
End of Survey Message for posttest 7
Frequency and Channel of Exposure [EXPOSED ONLY] 8
Attitudes and Beliefs [ALL] 15
Behavior [ALL EXCEPT EMS PERSONNEL] 17
Behavior [EMS PERSONNEL ONLY] 20
Use of Campaign Materials [EXPOSED ONLY] 23
Media Use and Habits (UNEXPOSED ONLY) 27
Demographic Characteristics [ALL] 30
HCP Intended Audiences
Nurse practitioners (NPs) and physician assistants (PAs) who work at urgent care clinics.
Emergency department triage nurses.
General medical ward staff.
Primary care physicians (PCPs).
Long-Term care (LTC) nurses.
LTC medical technicians and sitters.
Priority markets
classification of Respondents based on their responses to the screener questions
Respondents should be classified as “Emergency Medical Services (EMS) personnel” if their response(s) to
Q9 = Emergency Medical Services (EMS) personnel AND
Q10 = Ambulances and/or medical transport services companies
Respondents should be classified as “NPs/PAs who work at urgent care clinics” if their response(s) to
Q9 = Nurse Practitioner (NP) or Physician Assistant (PA) AND
Q10 = Urgent care medical clinic
Respondents should be classified as “Emergency Department Triage Nurses” if their response(s) to
Q9 = Registered Nurse (RN), Licensed Professional Nurse (LPN), or Licensed Vocational Nurse (LVN) AND
Q10 = Emergency room and/or department AND
Q12 = Yes
Respondents should be classified as “General Medical Ward Staff” if their response(s) to
Q9 = ANY of the options except “EMS,” AND
Q10 = Hospital AND
Q11 = No
Respondents should be classified as “PCPs” if their response(s) to
Q9 = Physician (MD or DO) AND
Q10=All except “Emergency room and/or department,” “Ambulances and/or medical transport services companies” AND
Q11 = Yes
Respondents should be classified as “LTC Nurses” if their response(s) to
Q9 = Nurse practitioner (NP), Registered Nurse (RN), Licensed Professional
Nurse (LPN), or Licensed Vocational Nurse (LVN)
Q10 = Long-term care setting
Respondents should be classified as “LTC Medical Technicians and Sitters” if their response(s) to
Q9 = Medical Technician or Medical Sitter
Q10 = Long-term care setting
Tallgrass: Do not send a survey link to participants who did not fall under any intended audience group.
End of screener Message
Programmer: Present this message to participants who completed the screener.
Thank you for answering the screening questions. If you are eligible to participate, you will receive an email with a copy of your signed informed consent and the link to take the survey. The incentive described in the informed consent will be available upon completion of the survey. If you have any questions or concerns, please contact Julie Overby at j.o@tallgrassmarketresearch.com or call phone number 253-238-7787 or 360-942-8466.
SCREENER Ineligibility Message
Programmer: Present this message to participants who do not give their consent and respondents who provide a response that makes them ineligible to continue with the survey.
Thank you for your willingness to participate in this survey. Unfortunately, you are not eligible to proceed with the survey. If you have any questions, please contact Julie Overby at j.o@tallgrassmarketresearch.com or call phone number 253-238-7787 or 360-942-8466.
Thank you for your time.
GAOS HCP Screener Begins Here
INFORMED CONSENT TO PARTICIPATE IN AN ONLINE SURVEY
On behalf of the Centers for Disease Control and Prevention (CDC), CATMEDIA, an Atlanta-based program management, training, and creative services company, is conducting an online survey with adults to gather feedback on educational materials related to sepsis. We hope to use what we learn from these survey results to improve these materials and/or how and where we promote them to raise awareness within your community. This is the screener. After you are determined as eligible to participate, you will only be asked to complete the survey once. We expect this survey to take about 20 minutes.
Your participation in this survey is completely voluntary. You may choose to skip questions that you do not want to answer and/or stop the survey at any time for any reason. Refusal to participate will not result in any penalties.
If you choose to participate in this survey, we will keep your answers private and will not share your personal information with anyone outside of the survey team.
At the end of the survey, you will receive $75 through Venmo or PayPal, or a $75 gift card as a token of our appreciation for your time. You should receive it within 7 business days.
If you have questions or need a copy of the informed consent, please email Julie Overby at j.o@tallgrassmarketresearch.com or call 253-238-7787 or 360-942-8466.
Please answer the question below and print a copy for your records before proceeding to the next page. If you select “Yes,” it means you understand the information in this consent form and that you agree to take the survey.
All questions with an asterisk [*] require a response.
* Do you agree to participate in this survey?
Yes
No
Programmer: If the respondent selects “Yes” to the question, “Do you agree to participate in this survey” present the next page for the respondent to enter their name as an electronic signature and date of consent.
If the respondent selects “No” terminate the survey and present the INELIGIBILITY MESSAGE.
* Enter your full name here.

* Enter today’s date here. (MM/DD/YYYY)
Programmer: If the respondent enters their name as an electronic signature and date of consent, do not terminate the survey.
Screener Survey Introduction
Programmer: Include one question per page. Screener should terminate as soon as the respondent selects an option that deems him/her ineligible.
Thank you for participating in this survey. The results of this survey will help the Centers for Disease Control and Prevention (CDC) refine and improve its ongoing campaign promoting early recognition and timely treatment of sepsis.
OMB Statement
Form
Form Approved
OMB No. 0920-1384
Expiration Date: 03/31/2026
Public reporting burden of this collection of information is estimated to average 20 minutes per response, including the time for reviewing instructions, searching existing data sources, gathering, and maintaining the data needed, and completing and reviewing the collection of information. An agency may not conduct or sponsor, and a person is not required to respond to a collection of information unless it displays a currently valid OMB Control Number. Send comments regarding this burden estimate or any other aspect of this collection of information, including suggestions for reducing this burden to CDC/ATSDR Reports Clearance Officer, 1600 Clifton Road NE, MS D-74, Atlanta, Georgia 30333; ATTN: PRA 0920-22CB
* May we ask you some questions to see if you are eligible to take this survey?
Yes
No [INELIGIBLE/TERMINATE]
Programmer: If “No” to Q4, TERMINATE else proceed with survey.
How old are you? _ _ years
Prefer not to answer [INELIGIBLE]
If the respondent is under 18 years of age, TERMINATE and present the INELIGIBILITY message.
If “prefer not to answer,” TERMINATE.
If the respondent is eligible based on age, proceed to Q6.
Are you a healthcare professional (e.g., doctor, physician assistant, nurse, emergency medical services personnel, medical technician, or medical sitter)?
Yes
No [INELIGIBLE]
In what State do you perform the majority of your work? _____________________
Programmer: Create a dropdown option with all U.S. States and options for “Prefer not to answer” and “I cannot find my State.”
In what ZIP Code do you perform the majority of your work? _____________________
Programmer: Create a dropdown option with Approved ZIP Codes and options for “Prefer not to answer” and “I cannot find my ZIP Code.”
Programmer: Priority markets include New York (NY), Illinois (IL), and/or Louisiana (LA).
Programmer: If not within one of the priority markets and approved ZIP Codes, TERMINATE, otherwise, proceed with survey.
What type of healthcare professional are you? Select all that apply.
Physician (MD or DO)
Nurse Practitioner (NP)
Physician Assistant (PA)
Registered Nurse (RN)
Licensed Professional Nurse (LPN)
Licensed Vocational Nurse (LVN)
Certified Medical Technician (CMT)
Certified Nursing Assistant (CNA)
Medical Technician or Medical Sitter
Emergency Medical Services (EMS) personnel
None of the above [INELIGIBLE]
In what type of setting do you work? Select all that apply.
Ambulances and/or medical transport services companies
Emergency room and/or department
Hospital
Intensive care unit
Urgent care medical clinic
Private practice
Community-based clinic or Federally Qualified Health Center
Managed care medical clinic (e.g., Kaiser)
Long-term care setting (e.g., nursing home, skilled nursing facility, assisted living, residential care community, long-term acute care center, congregate day program)
None of the above [INELIGIBLE]
Do you provide primary care to adults and/or children?
Programmer: Show this question to respondents who select “Physician (MD or DO)” to Q9, else skip it.
Yes
No
Are you an emergency department triage nurse?
Programmer: Show this question to respondents who select “Registered Nurse (RN),” “Licensed Professional Nurse (LPN),” or “Licensed Vocational Nurse (LVN)” to Q9 AND “Emergency room and/or department” to Q10, else skip it.
Yes
No
General Instructions for Programmer
Hide all subheadings of sections and questions from respondents.
Hide all programmer’s instructions from respondents.
Terminate also means ineligible.
Terminate all ineligible respondents immediately.
Present the “Ineligibility Message” whenever a response terminates the survey.
RECRUITER: Terminate after quota for each category, audience, and/or group is met.
RECRUITER: Assign participants to only one intended audience group.
Ineligibility Message
Thank you for your willingness to participate in this survey. Unfortunately, you are not eligible to proceed with the survey. If you have any questions, please contact Julie Overby at j.o@tallgrassmarketresearch.com or call phone number 253-238-7787 or 360-942-8466.
Thank you for your time.
End of Survey Message for posttest
Programmer: Place this message in the collector’s page for custom thank you.
Thank you for taking the time to participate in this important survey!
Exposure to Campaign [ALL]
Programmer: Place this link in the collector’s page for custom URL to redirect all respondents to this link.
Link: https://www.cdc.gov/sepsis/
Programmer: Include one question per page.
Now we would like to ask you about a CDC campaign to raise awareness about a medical condition called sepsis that you may or may not have seen or heard about in the past 2-3 months.
Please indicate below whether you have seen or heard any of the following campaign names or slogans in the past 2-3 months.
Programmer: Rotate (a - e), the column named “Campaigns” among respondents.
-
Campaigns
Yes
No
Do not know/cannot recall
Be Smart. Beat Sepsis.
Be Sepsis Aware
Health is Precious. Don’t Get Sepsis.
Get Ahead of Sepsis
Know the Threat. Prevent Sepsis.
I
 n
the past 2-3 months, have you heard this slogan and/or seen this
logo?
n
the past 2-3 months, have you heard this slogan and/or seen this
logo?
Yes
No
Do not know/cannot recall
Programmer: Categorize respondents as “UNEXPOSED” only If the respondent selects “No,” “Do not know/cannot recall” or did not respond to Q1d and Q2, then proceed to the KNOWLEDGE section.
Respondents with any other combination should be “EXPOSED,” then proceed to FREQUENCY AND CHANNEL OF EXPOSURE section.
Frequency and Channel of Exposure [EXPOSED ONLY]
Programmer: Include one question per page.
You indicated that you had seen or heard the campaign name, Get Ahead of Sepsis, or seen the campaign logo in the past 2-3 months.
In the past 2-3 months, approximately how often did you see or hear CDC’s Get Ahead of Sepsis campaign messages, campaign name, or logo in …?
Programmer: Rotate the media options (Poster, Fact sheet, Brochure, etc.). Leave “Other” response last.
-
Printed Media
1-2 times a day
Once a week
1-3 times a month
Less than once a month
Never
Do not know/ cannot recall
Poster
Fact sheet
Brochure
Graphic
Newspaper/magazine advertisement
Flyer
Other print media, please specify below:
In the past 2-3 months, approximately how often did you see or hear CDC’s Get Ahead of Sepsis campaign messages, campaign name, or logo in …?
Programmer: Rotate the media options (Facebook, Instagram, Twitter, etc.). Leave “Other” response last.
-
Social Media
1-2 times a day
Once a week
1-3 times a month
Less than once a month
Never
Do not know/ cannot recall
Facebook
Instagram
Twitter
LinkedIn
Doximity
Sermo
YouTube
Other social media, please specify below:
In the past 2-3 months, approximately how often did you see or hear CDC’s Get Ahead of Sepsis campaign messages, campaign name, or logo in …?
Rotate the media options (Online/Internet Media). Leave “Other” response last.
-
Online/Internet Media
1-2 times a day
Once a week
1-3 times a month
Less than once a month
Never
Do not know/ cannot recall
Health websites/resources (WebMD, Mayo clinic)
Video conferencing background screen
Website advertisements
Online news articles
Streaming TV/video services (e.g., Hulu, Netflix, [Amazon] Prime Video)
Streaming Internet radio
Blogs
Advertisements on mobile phone (including mobile apps)
Search engines (e.g., Google)
Other websites, please specify below:
In the past 2-3 months, approximately how often did you see or hear CDC’s Get Ahead of Sepsis campaign messages, campaign name, or logo in …?
Programmer: Rotate the media options (TV and Radio Media). Leave “Other” response last.
-
TV and Radio
1-2 times a day
Once a week
1-3 times a month
Less than once a month
Never
Do not know/ cannot recall
Television (cable, satellite, or antenna)
Broadcast radio
Other media formats, please specify below:
In the past 2-3 months, approximately how often did you see or hear CDC’s Get Ahead of Sepsis campaign messages, campaign name, or logo in …?
Programmer: Rotate the media options (Public Places). Leave “Other” response last.
-
Public Places
1-2 times a day
Once a week
1-3 times a month
Less than once a month
Never
Do not know/ cannot recall
Billboards
Bus, train, or subway stations
buses or taxi cabs
Advertisement in a mall
Advertisement in a grocery store
Advertisement in a store pharmacy
Advertisement at a shopping center or parking lot
Other public places, please specify below:
In the past 2-3 months, did you see or hear CDC’s Get Ahead of Sepsis campaign messages, campaign name, or logo at your workplace (including at your home workplace for telework)?
Yes, I personally placed or shared CDC’s Get Ahead of Sepsis campaign materials at my workplace in the past 2-3 months.
Yes, I saw CDC’s Get Ahead of Sepsis campaign at my workplace in the past 2-3 months, but I was not responsible for placing or sharing it.
No, but I saw materials from another sepsis campaign at my workplace in the past 2-3 months.
No, I have not seen any materials about sepsis at my workplace in the past 2-3 months.
Programmer: If the respondent selects “Yes” to the question above, proceed to the next question, else skip it.
In the past 2-3 months, where did you see or hear CDC’s Get Ahead of Sepsis campaign messages, campaign name, or logo at your workplace (including your home workplace for telework)? Select all that apply.
Printed material(s) designed to educate patients about sepsis
Printed material(s) designed to improve sepsis fast recognition and treatment by healthcare professionals
Digital material(s) designed to educate patients about sepsis
Digital material(s) designed to improve sepsis fast recognition and treatment by healthcare professionals
Video displays in patient waiting rooms/areas
Workplace website or internal email/newsletter
Email or e-newsletter from external organization, such as a state or local public health agency or professional society or association
Webcasts or webinars
Live events
Other, please specify below:
Do not know/cannot recall [Programmer: Lock response.]
Programmer: If the respondent is presented the question above, after responding or if they choose to skip, proceed to “KNOWLEDGE” section.
You indicated that you saw or heard the campaign name, Get Ahead of Sepsis or saw the campaign logo in the past 2-3 months. Where did you see or hear it? [Open-ended response] _______________________________________
Programmer: If the respondent leaves the above open-ended question blank, reclassify these respondents as “Unexposed” and proceed to “KNOWLEDGE” section.
Knowledge [ALL]
Programmer: Include one question per page. ACCURATE/INACCURATE responses have been indicated but do not disclose to respondents.
Thinking about your knowledge and awareness of sepsis, please indicate which statements you believe to be true or false.
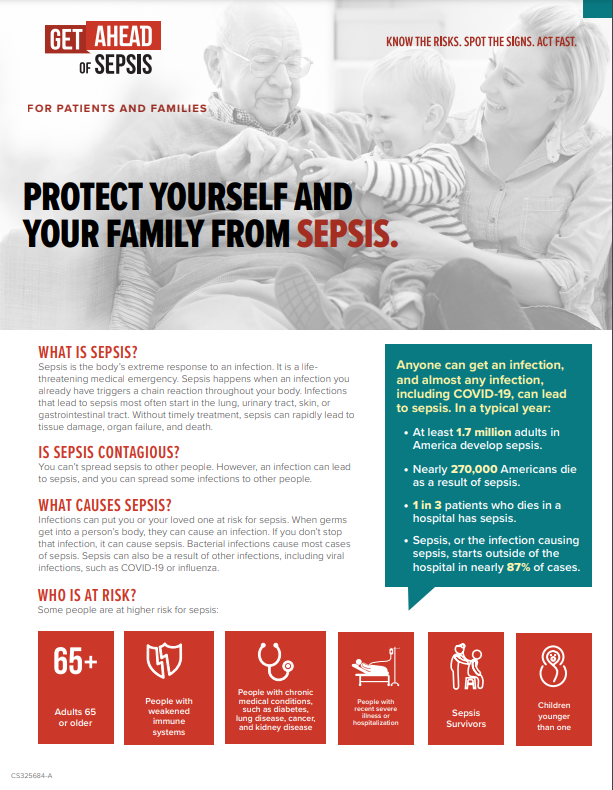
About 1 in 3 patients who dies in a hospital had sepsis during that hospitalization.
TRUE [ACCURATE]
FALSE [INACCURATE]
Anyone can get an infection, and almost any infection including COVID-19, can lead to sepsis.
TRUE [ACCURATE]
FALSE [INACCURATE]
Sepsis is defined as the following:
A chronic condition that primarily affects kidney function. [INACCURATE]
The body’s extreme response to an infection. [ACCURATE]
A neurological disorder resulting from the flu. [INACCURATE]
A Contagious illness that commonly peaks in the winter. [INACCURATE]
All of the above [INACCURATE]
None of the above [INACCURATE]
Do not know [INACCURATE] [Programmer: Lock response.]
Which of the following types of infections, if any, are OFTEN linked with sepsis? Select all that apply.
Ear [INACCURATE]
Skin [ACCURATE]
Lung [ACCURATE]
Eye [INACCURATE]
Urinary tract [ACCURATE]
Nail [INACCURATE]
Gastrointestinal tract [ACCURATE]
Severe COVID-19 [ACCURATE]
Do not know [INACCURATE] [Programmer: Lock response.]
If your patient and/or resident is healthy, an infection is not anything you need to worry about.
TRUE [INACCURATE]
FALSE [ACCURATE]
Which of the following, if any, are the most frequently identified pathogens that cause infections that can develop into sepsis? Select all that apply.
Staphylococcus aureus [ACCURATE]
Bordetella pertussis [INACCURATE]
Helicobacter pylori [INACCURATE]
Escherichia coli [ACCURATE]
Clostridium botulinum [INACCURATE]
Some types of streptococci [ACCURATE]
Do not know [INACCURATE] [Programmer: Lock response.]
With fast recognition and treatment of sepsis, most people survive.
TRUE [ACCURATE]
FALSE [INACCURATE]
Select common signs and symptoms of sepsis below:
Excessive hunger [INACCURATE]
Clammy or sweaty skin [ACCURATE]
Confusion or disorientation [ACCURATE]
Extreme pain or discomfort [ACCURATE]
Fever, shivering, or feeling very cold [ACCURATE]
High heart rate or low blood pressure [ACCURATE]
Shortness of breath [ACCURATE]
I do not know any of the signs and symptoms of sepsis. [INACCURATE] [This is locked]
Only doctors need to know their facility’s existing guidance for diagnosing and managing sepsis.
TRUE [INACCURATE]
FALSE [ACCURATE]
Which of the following activities, if any, should you advise your patients and/or residents to do to prevent infections that can lead to sepsis? Select all that apply.
Regular handwashing [ACCURATE]
Showering twice daily [INACCURATE]
Getting recommended vaccines [ACCURATE]
Avoiding public restrooms [INACCURATE]
Keeping cuts and wounds clean and covered until healed [ACCURATE]
Taking good care of chronic conditions [ACCURATE]
Ensuring proper patient catheter management (doctor or nurse only) [ACCURATE]
Do not know [INACCURATE] [Programmer: Lock response.]
If your patients and/or residents suspect sepsis or have an infection that’s not getting better or is getting worse, you should discuss with them if the infection could be leading to sepsis.
TRUE [ACCURATE]
FALSE [INACCURATE]
Which of the following groups of individuals are at higher risk for developing infections that can lead to sepsis? Select all that apply.
Adults 65 or older [ACCURATE]
People with weakened immune systems [ACCURATE]
People with chronic medical conditions, such as diabetes, lung disease, cancer, and kidney disease [ACCURATE]
Children younger than one year old [ACCURATE]
People who have previously survived sepsis [ACCURATE]
People with recent severe illness or hospitalization [ACCURATE]
Adults with no underlying conditions between the ages of 20 and 35 years [INACCURATE]
Do not know [INACCURATE] [Programmer: Lock response.]
Antibiotic therapy for patients who have developed sepsis should NOT be reassessed during the course of treatment.
TRUE [INACCURATE]
FALSE [ACCURATE]
Which of the following, if any, is true about sepsis? Select all that apply.
Only people with chronic diseases are at risk for sepsis. [INACCURATE]
Sepsis can cause tissue damage, organ failure, and death. [ACCURATE]
Sepsis is a medical emergency. [ACCURATE]
With fast recognition and treatment, most people survive. [ACCURATE]
Sepsis is not a medical emergency. [INACCURATE]
Do not know [INACCURATE] [Programmer: Lock response.]
Which of the following is true, if any, about what you should do if you suspect a patient has sepsis? Select all that apply.
Know your facility’s existing guidance for diagnosing and managing sepsis. [ACCURATE]
Immediately alert the clinician in charge if it is not you. [ACCURATE]
Start antibiotics as soon as possible in addition to other therapies appropriate for the patient. If a specific bacterial cause of sepsis is known, therapy should be targeted to optimize treatment, and broad-spectrum antibiotics might not be needed. [ACCURATE]
Check patient progress frequently. Always remember to prescribe the right antibiotic, at the right dose, for the right duration, and at the right time. Reassess antibiotic therapy to stop or tailor treatment based on the patient’s clinical condition and diagnostic test results as appropriate. [ACCURATE]
Schedule the next follow-up clinic appointment for the patient to be seen two weeks out. [INACCURATE]
Do not know [INACCURATE] [Programmer: Lock response.]
Some hospitalized COVID-19 patients are diagnosed with sepsis.
Attitudes and Beliefs [ALL]
Programmer: Include one set of questions (e.g., perceived susceptibility, perceived severity) per page.
Next, we are going to ask you some questions to learn more about your perspective on infections and sepsis. Please give us your honest responses. In the below questions, ‘residents’ refers to nursing home or long-term care residents in the facility where you work.
Please indicate the extent to which you agree with the following statements, from strongly disagree to strongly agree.
-
[Perceived Susceptibility]
Strongly Disagree
Disagree
Neither Agree nor Disagree
Agree
Strongly Agree
My patients and/or residents are at risk of developing sepsis.
My patients and/or residents are at risk of developing infections that could lead to sepsis.
[Perceived Severity]
Strongly Disagree
Disagree
Neither Agree nor Disagree
Agree
Strongly Agree
If one of my patients and/or residents developed sepsis, it could cause severe problems, such as tissue damage or organ failure.
If one of my patients and/or residents developed sepsis, it could lead to death.
[Perceived Benefits]
Strongly Disagree
Disagree
Neither Agree nor Disagree
Agree
Strongly Agree
If my patients and/or residents take proper care of their chronic conditions, this will decrease their chances of developing infections that can lead to sepsis.
If my patients and/or residents practice good hand hygiene, this will decrease their chances of developing infections that can lead to sepsis.
If my patients and/or residents keep their cuts and wounds clean and covered, this will decrease their chances of developing infections that can lead to sepsis.
If my patients and/or residents get recommended vaccinations, this will decrease their chances of developing infections that can lead to sepsis.
Fast recognition and treatment can increase my patients’ and/or residents’ chances of survival from sepsis.
Recognizing signs and symptoms of sepsis early decreases my patients’ and/or residents’ risk of death from sepsis.
Acting fast if I suspect sepsis in my patients and/or residents can save lives.
[Self-Efficacy]
Strongly Disagree
Disagree
Neither Agree nor Disagree
Agree
Strongly Agree
I am confident that I can educate my patients and/or residents on how to prevent infections that can lead to sepsis.
I am confident that I can recognize the signs and symptoms of sepsis in my patients and/or residents.
I am confident that I can take rapid action to treat infections and sepsis or get patients into the proper care they need when sepsis is suspected in patients.
Behavior [ALL EXCEPT EMS PERSONNEL]
Programmer: Include one question per page.
We’d like to know more about conversations you might have had with your patients and/or residents and their caregivers about sepsis.
Please indicate how frequently you discussed the following with your patients and/or residents and their caregivers in the past 2-3 months.
Programmer: Rotate response options in the first column.
Behavior (Information Sharing with Patients, Residents, Caregivers) |
Never |
Rarely |
Sometimes |
Often |
Always |
N/A |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
What are the barriers you commonly encounter when educating your patients and/or residents and their caregivers on preventing sepsis or on preventing infections that can lead to sepsis? Select all that apply.
I am not familiar enough with these topics.
I do not feel confident educating my patients and/or residents on these topics.
I do not think my patients/residents, or their caregivers will understand these topics.
I do not think it is important for my patients and/or residents or their caregivers to understand these topics.
I do not think my patients and/or residents, or their caregivers will be interested in or receptive to learning about these topics.
I do not have time to educate my patients and/or residents or their caregivers on these topics.
I do not think sepsis is a big problem for my patients and/or residents.
I’m not confident the healthcare system in the area where my patients and/or residents live can respond correctly to sepsis.
I’m not confident the healthcare professionals in the area where my patients and/or residents live can respond correctly to sepsis.
My patients and/or residents live very far from healthcare services.
My patients and/or residents rely on telehealth services.
My patients and/or residents think that Covid-19 patients have overwhelmed the healthcare system and healthcare professionals, therefore we may not be able to respond to sepsis correctly.
My patients and/or residents are afraid of getting Covid-19 if they go to the Emergency room/department.
Other, please explain below:
I have not encountered any barriers to educating my patients and/or residents, or their caregivers on these topics. [Programmer: Lock response.]
In the past 2-3 months, have you suspected that a patient and/or resident at your facility had sepsis?
Yes
No
Programmer: if the respondent selects “No” to the above question, skip the rest of the questions in this section and proceed to the "Behavior ALL" section.
Please indicate how many sepsis patients and/or residents you attended to in your facility within the past 2-3 months.
0
1 - 4
5 - 9
10 or more
Do not know
[Behavior - Act fast if sepsis is suspected] Please indicate how often you took the following steps for your sepsis patients in the past 2-3 months.
Behavior (Act fast if sepsis is suspected) |
Never |
Rarely |
Sometimes |
Often |
Always |
N/A (I am the clinician in charge of initiating treatment for these patients and/or residents.) |
|
|
|
|
|
|
|
[Behavior - Act fast if sepsis is suspected] Please indicate how often you took the following steps for your sepsis patients in the past 2-3 months.
Behavior (Act fast if sepsis is suspected) |
Never |
Rarely |
Sometimes |
Often |
Always |
N/A |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Please indicate how many patients you transported to the hospital that you believed had sepsis in the past 2-3 months.
0
1 - 4
5 - 9
10 or more
Do not know
Please select information you collect from patients or caregivers about your patients to help you assess possibility of sepsis, if any.
I ask about the patient’s age. [ACCURATE]
I ask the patient or caregivers what signs and symptoms the patient is experiencing. [ACCURATE]
I ask the patient or caregivers how long the symptoms have been ongoing. [ACCURATE]
I do not ask the patient or caregivers any questions about my patients. [INACCURATE]
I ask if the patient is confused/disoriented, has shortness of breath, in extreme pain, clammy or sweaty, or shivering/feeling cold. [ACCURATE]
I ask the patient or caregivers to provide names and/or dosages of medications the patient takes. [ACCURATE]
I ask if the patient has any open cut, injuries and /or abscess. [ACCURATE]
I collect the patient’s vital signs. (such as, temperature, pulse, breathing, blood pressure, etc.) [ACCURATE]
I ask if the patient recently received treatment for any bacterial or viral infection. [ACCURATE]
I ask if the patient has any underlying health condition. [ACCURATE]
I ask for the patient’s DNA. [INACCURATE]
I assess any injury and/or abscess on the patient. [ACCURATE]
I do not collect any information about my patients from the patient or caregivers. [INACCURATE]
Do not know/cannot recall [INACCURATE] [Programmer: Lock response.]
Please indicate how often you took the following steps for the patients you transported to the hospital that you believed had sepsis in the past 2-3 months.
Behavior (Act fast if sepsis is suspected) |
Never |
Rarely |
Sometimes |
Often |
Always |
N/A (I did not transport any patient I suspected had sepsis.) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Behavior [ALL]
[Behavioral Intention] I plan to take rapid action and initiate appropriate treatment when sepsis is suspected in my patients and/or residents.
Strongly disagree
Disagree
Neither agree nor disagree
Agree
Strongly agree
What are the barriers you experience to taking rapid action and initiating appropriate treatment when sepsis is suspected in your patients and/or residents? Select all that apply.
I am not confident I can identify the signs and symptoms of sepsis.
I do not know how to alert the clinician in charge. (it is not me)
I am not comfortable alerting the clinician in charge. (it is not me)
It is not my role to identify sepsis and/or to alert the clinician in charge.
High turnover rate or shortage of staff
Other, please specify below:
I do not have any barriers. [Programmer: Lock response.]
[ALL HCPs] In the last 2-3 months, have you looked for information about infections that can lead to sepsis?
Yes
No
Do not know/cannot recall
Programmer: If the respondent selects “Yes” to the above question, proceed to the next question, else skip it.
To whom or where do you go to learn about infections that can lead to sepsis? Select all that apply.
Colleagues, other healthcare professionals
Centers for Disease Control and Prevention (CDC) website or material, please specify below:
Peer-reviewed journals (Printed or online), please specify below:
Health websites/health-related mobile apps (e.g., WebMD, Mayo Clinic, Medscape, UpToDate, Epocrates, etc.), please specify below:
Medical conferences, please specify below:
Local/state health departments
Medical or professional associations, please specify below:
My place of work
Continuing education/medical education/training courses (CE/CME, etc.), please specify below:
Social media (e.g., Facebook, Instagram, Twitter, LinkedIn, Doximity, Sermo), please specify below:
Sepsis organizations (e.g., Sepsis Alliance, etc.), please specify below:
Other, please specify below:
I have not looked for information on this topic. [Programmer: Lock response.]
How trusted do you feel CDC is as a source of sepsis information?
Very trusted
Trusted
Somewhat trusted
A little trusted
Not at all trusted
Do you have Infection Prevention and Control (IPC) practices/guidelines at your facility?
Yes
No
Do not know
Programmer: If the respondent selects “Yes” to the above question, proceed to the next question, else skip it.
Do you know the content of the Infection Prevention and Control (IPC) practices/guidelines at your facility?
Do you have a sepsis protocol at your facility?
Yes
No
Do not know
Programmer: If the respondent selects “Yes” to the above question, proceed to the next question, else skip it.
Do you know the content of your facility’s sepsis protocol?
Did you know that CDC has a Get Ahead of Sepsis webpage with resources you can use to help educate your patients about preventing infections that can lead to sepsis?
Yes
No
Use of Campaign Materials [EXPOSED ONLY]
Have you been contacted by any of these organizations in the last 2-3 months about sepsis?
Local Health Department, please specify below:
State Health Department, please specify below:
Other, please specify below:
None of these organizations [Programmer: Lock response.]
Programmer: Put a page break here.
Did your partners provide any of these campaign materials for you to use to help educate your patients and/or residents about sepsis? Select all that apply.
Infographic
|

Fact sheet
|

None of the above
Programmer: If the respondent selects “none of the above” in the above question, skip to the last question in this section.
Programmer: only show campaign images and their corresponding questions to respondents who select them in the above question.
Programmer: Put a page break here.
A.

Please select how often in the past 2-3 months you used this infographic to educate your patients about sepsis?
Select one |
Rarely |
Sometimes |
Often |
Always |
|
|
|
|
|
Programmer: Put a page break here and skip logic.
How helpful for you was this infographic in educating your patients about sepsis?
Very helpful
Helpful
Somewhat helpful
A little helpful
Not at all helpful
Programmer: Put a page break here and skip logic.
|
|
B. |
|

Please select how often in the past 2-3 months you used this fact sheet to educate your patients and/or residents about sepsis?
Select one |
Rarely |
Sometimes |
Often |
Always |
|
|
|
|
|
Programmer: Put a page break here and skip logic.
How helpful for you was this fact sheet in educating your patients and/or residents about sepsis?
Very helpful
Helpful
Somewhat helpful
A little helpful
Not at all helpful
Programmer: Put a page break here and skip to demographics section.
Why have you not used CDC Get Ahead of Sepsis resources to educate your patients and/or residents about sepsis? Select all that apply.
I did use CDC Get Ahead of Sepsis resources to educate my patients, but they were not the ones shown above. If so, what resources did you use? Please specify below:
I do not usually use patient education resources when educating my patients on any topics.
I/my organization has my/our own resources.
I use resources developed by other organizations.
I forget to use them.
I do not have time to use them.
I do not know where to find these resources.
I looked at them, but did not find them helpful.
I am not familiar enough with these resources to feel comfortable using them.
Other, please specify below:
Do not know [Programmer: Lock response.]
Programmer: Put a page break here and skip to demographics section.
Media Use and Habits (UNEXPOSED ONLY)
Programmer: Include one set of questions (e.g., printed media, social media) per page. Rotate all media options. Leave “Other” response last.
We would like to ask you a few questions about your media use and habits.
In an average month, how often do you…
Printed Media |
1-2 times a day |
Once a week |
1-3 times a month |
Less than once a month |
Never |
Do not know/ cannot recall |
Read printed magazines |
|
|
|
|
|
|
Read printed newspapers |
|
|
|
|
|
|
Read brochures or flyers on health-related topics |
|
|
|
|
|
|
Read other printed media, please specify below:
|
|
|
|
|
|
|
In an average month, how often do you…
Social Media |
1-2 times a day |
Once a week |
1-3 times a month |
Less than once a month |
Never |
Do not know/cannot recall |
Use Facebook |
|
|
|
|
|
|
Use Instagram |
|
|
|
|
|
|
Use Twitter |
|
|
|
|
|
|
Use LinkedIn |
|
|
|
|
|
|
Use Doximity |
|
|
|
|
|
|
Use Sermo |
|
|
|
|
|
|
Use YouTube |
|
|
|
|
|
|
Use other social media, please specify below:
|
|
|
|
|
|
|
In an average month, how often do you…
Online/Internet Media |
1-2 times a day |
Once a week |
1-3 times a month |
Less than once a month |
Never |
Do not know/cannot recall |
Read health websites /resources |
|
|
|
|
|
|
Read news online |
|
|
|
|
|
|
Read magazines online |
|
|
|
|
|
|
Listen to internet radio |
|
|
|
|
|
|
Watch TV/movies using streaming services (e.g., Netflix, Hulu, [Amazon] Prime Video) |
|
|
|
|
|
|
Read blogs |
|
|
|
|
|
|
Streaming internet radio |
|
|
|
|
|
|
search engines (e.g., Google) |
|
|
|
|
|
|
Visit other websites, please specify below:
|
|
|
|
|
|
|
In an average month, how often do you…
TV and Radio |
1-2 times a day |
Once a week |
1-3 times a month |
Less than once a month |
Never |
Do not know/cannot recall |
Watch television (cable, satellite, or antenna) |
|
|
|
|
|
|
Listen to broadcast radio |
|
|
|
|
|
|
Listen to satellite radio |
|
|
|
|
|
|
Watch or listen to other TV or radio media, please specify below:
|
|
|
|
|
|
|
In an average month, how often do you…
Public Places |
1-2 times a day |
Once a week |
1-3 times a month |
Less than once a month |
Never |
Do not know/cannot recall |
See billboards |
|
|
|
|
|
|
Use buses, subways, or trains |
|
|
|
|
|
|
Use taxi cabs |
|
|
|
|
|
|
Shop in malls |
|
|
|
|
|
|
Shop in grocery stores |
|
|
|
|
|
|
Shop in pharmacies (e.g., CVS, Walgreens, Walmart) |
|
|
|
|
|
|
Visit other public places, please specify below:
|
|
|
|
|
|
|
In an average month, how often do you…
Other Media |
1-2 times a day |
Once a week |
1-3 times a month |
Less than once a month |
Never |
Do not know/cannot recall |
Read email newsletters from healthcare professional associations |
|
|
|
|
|
|
Listen to webcasts or webinars related to my profession |
|
|
|
|
|
|
Listen to podcasts |
|
|
|
|
|
|
Attend live events (presentation at a conference) |
|
|
|
|
|
|
Use other media, please specify below:
|
|
|
|
|
|
|
To whom or where do you go to learn about infections that can lead to sepsis? Select all that apply.
Colleagues, other healthcare professionals
Centers for Disease Control and Prevention (CDC) website or material, please specify below:
Peer-reviewed journals (Printed or online), please specify below:
Health websites/health-related mobile apps (e.g., WebMD, Mayo Clinic, Medscape, UpToDate, etc.), please specify below:
Medical conferences, please below:
Local/state health departments
Medical or professional associations, please specify below:
My place of work or organization
Continuing education/medical education/training courses (CE/CME, etc.), please specify below:
Social media (e.g., Facebook, Instagram, Twitter, LinkedIn), please specify below:
Sepsis organizations (e.g., Sepsis Alliance, etc.), please specify below:
Other, please specify below:
I have not looked for information on this topic
. [Programmer: Lock response.]
Demographic Characteristics [ALL]
Include one question per page.
Thank you. Now we would like to know more about you.
How long have you worked as a healthcare professional performing the same duties as your current role?
Less than one year
1-5 years
6-9 years
10 or more years
Prefer not to answer
What sex were you assigned at birth, on your original birth certificate?
Male
Female
Refused
I don’t know
Do you currently describe yourself as male, female, transgender?
Male
Female
Transgender
None of these
What is your ethnicity?
Hispanic or Latino
Not Hispanic or Latino
What is your race?
American Indian or Alaska Native
Asian
Black or African American
Native Hawaiian or Other Pacific Islander
White
What is the highest degree you have received? Please select only one.
Programmer: If a respondent selects “Prefer not to answer” do not allow them to select other responses.
High school graduate (or equivalent)
Some college or technical school (1–4 years, no degree)
Associate or technical degree
Bachelor’s (4-year college) degree
Master’s degree
Professional or doctoral degree (MD, JD, PhD, etc.)
Prefer not to answer
Before you go, a $75 incentive through Venmo or PayPal, or a $75 gift card will be sent to you as a token of our appreciation for your time. You should receive it within 7 business days.
*Please choose your preferred method to receive your incentive and fill out the short form to receive your incentive or click “Exit” if you do not wish to receive incentive.
Venmo Programmer: Link this option to “Venmo page.”
PayPal Programmer: Link this option to “PayPal page.”
Gift card by mail Programmer: Link this option to “Gift card by mail page.”
Digital gift card Programmer: Link this option to “Digital gift card page.”
Exit (I do not wish to receive incentive) Programmer: Link this option to “End of Survey.”
Venmo Page
If you do not feel comfortable providing the information below, please contact Julie Overby at j.o@tallgrassmarketresearch.com or call 253-238-7787 or 360-942-8466.
First and Last Name:
Your Venmo username:
Your email associated with Venmo (optional but recommended):
Your phone number associated with Venmo (optional but recommended):
Programmer: Link this page to “End of Survey.”
PayPal Page
If you do not feel comfortable providing the information below, please contact Julie Overby at j.o@tallgrassmarketresearch.com or call 253-238-7787 or 360-942-8466.
First and Last Name:
Your email associated with PayPal (optional but recommended):
Your phone number associated with PayPal (optional but recommended):
Programmer: Link this page to “End of Survey.”
Gift card by mail Page
If you do not feel comfortable providing the information below, please contact Julie Overby at j.o@tallgrassmarketresearch.com or call 253-238-7787 or 360-942-8466.
*First and Last Name:
*Address Line 1:
Address Line 2:
*Town/City:
*State/Territory
*ZIP/Postal Code:
Phone number (optional):
Email (optional):
Programmer: Link this page to “End of Survey.”
Digital gift card Page
If you do not feel comfortable providing the information below, please contact Julie Overby at j.o@tallgrassmarketresearch.com or call 253-238-7787 or 360-942-8466.
First and Last Name:
*Your email:
Your phone number:
Programmer: Link this page to “End of Survey.”
| File Type | application/vnd.openxmlformats-officedocument.wordprocessingml.document |
| File Modified | 0000-00-00 |
| File Created | 0000-00-00 |
© 2026 OMB.report | Privacy Policy