Example SOAR Demonstration Grant Program Reporting Workbook 3.15.23.xlsx
SOAR Demonstration Grant Program Data
Example SOAR Demonstration Grant Program Reporting Workbook 3.15.23.xlsx
OMB: 0970-0609
⚠️ Notice: This form may be outdated. More recent filings and information on OMB 0970-0609 can be found here:
Document [xlsx]
Download: xlsx | pdf
Q. Client Demographics
Q. HTRP
Q. Network Providers
Q. Training Feedback Form
FY.Categories of Assistance



















































Overview
Q. Provider Capacity BuildingQ. Client Demographics
Q. HTRP
Q. Network Providers
Q. Training Feedback Form
FY.Categories of Assistance
Sheet 1: Q. Provider Capacity Building

|
Training Reporting Summary | Q1 | Q2 | Q3 | Q4 | |||||||||||||||||||||||
| Grant Recipient Name: | Total HT 101 Trainings | 0 | 0 | 0 | 0 | |||||||||||||||||||||||
| Grant Number: | Total Trauma Informed Care Trainings | 0 | 0 | 0 | 0 | |||||||||||||||||||||||
| Report Type: | Total Partnership Building Trainings | 0 | 0 | 0 | 0 | |||||||||||||||||||||||
| Report Period: | *Do not edit data in the table above. Counts will automatically update. | Total Trainings Delivered: | 0 | |||||||||||||||||||||||||
| Total Providers Trained: | 0 | |||||||||||||||||||||||||||
| OMB Control Number: 0970-NEW Expiration Date: XX/XX/XXXX |
||||||||||||||||||||||||||||
| Training Reporting | ||||||||||||||||||||||||||||
| As required by the Paperwork Reduction Act (PRA) of 1995, 44 U.S.C. § 3501-3521, the public reporting burden for the following performance indicators is estimated to average 1 hour per response, including the time for reviewing instructions, gathering and maintaining the data needed, and reviewing the collection of information. This form is approved under the Office of Management and Budget (OMB) control number OMB No: 0970-XXXX, expiration date is XX/XX/XXXX. An agency may not conduct or sponsor, and a person is not required to respond to, a collection of information unless it displays a currently valid OMB control number. | number | number | number | number | ||||||||||||||||||||||||
| Q1 | Q2 | Q3 | Q4 | |||||||||||||||||||||||||
| Human Trafficking 101: Definition, Types, Laws, and Indicators | Federal definition of severe forms of trafficking in persons | |||||||||||||||||||||||||||
| State and tribal anti-trafficking laws and legal considerations for a specific geographic area | ||||||||||||||||||||||||||||
| Information about human trafficking, including types of human trafficking and recruitment and/or retention tactics used by traffickers; indicators that a person may be experiencing human trafficking |
||||||||||||||||||||||||||||
| Case studies of individuals who have experienced human trafficking | ||||||||||||||||||||||||||||
| Approaches, Strategies, and Special Considerations for Working with Victims (e.g. Trauma Informed Care) | Safety protocols for those in direct contact with individuals potentially experiencing human trafficking | |||||||||||||||||||||||||||
| Please reference the Reporting Reference Guide (p.X-XX) to populate this table. | Services and benefits available for individuals who have experienced human trafficking | |||||||||||||||||||||||||||
| Special considerations for both domestic and foreign national minors experiencing human trafficking, which may include relevant legal and social welfare systems, such as juvenile justice, immigration, and child welfare |
||||||||||||||||||||||||||||
| Human Trafficking 101: Definition, Types, Laws, and Indicators | ||||||||||||||||||||||||||||
| How to deliver person-centered, trauma-informed services and assistance to individuals who have experienced human trafficking | ||||||||||||||||||||||||||||
| Housing and employment needs of individuals who have experienced human trafficking | ||||||||||||||||||||||||||||
| Intersectionality between race and human trafficking | ||||||||||||||||||||||||||||
| Intersectionality between sexual orientation, gender identity, and human trafficking | ||||||||||||||||||||||||||||
| Intersectionality between individuals with disabilities and human trafficking | ||||||||||||||||||||||||||||
| Intersectionality between human trafficking and forced criminality | ||||||||||||||||||||||||||||
| Building a Community Referral Network and Partnership Building | Referral protocols within a continuum of care for aftercare and ongoing service needs | |||||||||||||||||||||||||||
| Information about local continuums of care or multidisciplinary anti-trafficking task forces | ||||||||||||||||||||||||||||
| Processes by which organizational partnerships are developed and maintained | ||||||||||||||||||||||||||||
| Post-identification reporting and referral protocols | ||||||||||||||||||||||||||||
| Provider Type | Individuals Trained by Prime Recipient Providers | |||||||||||||||||||||||||||
| Individuals Trained by Subrecipient Providers | ||||||||||||||||||||||||||||
| Individuals Trained by Partner Organization Providers | ||||||||||||||||||||||||||||
Sheet 2: Q. Client Demographics
|
|
||||||||||||||||||||||||||||
| Client Demographics | ||||||||||||||||||||||||||||
| Grant Recipient Name: | Q1 | Q2 | Q3 | Q4 | ||||||||||||||||||||||||
| Grant Number: | number | number | number | number | ||||||||||||||||||||||||
| Report Period: | Client Demographics (All Providers) |
Number of clients enrolled in services by providers within the recipient’s multidisciplinary network by client age | ||||||||||||||||||||||||||
| Adult | ||||||||||||||||||||||||||||
| OMB Control Number: 0970-NEW Expiration Date: XX/XX/XXXX |
Minor | |||||||||||||||||||||||||||
| Total number of clients enrolled in services by providers within the recipient’s multidisciplinary network by client race/ethnicity | ||||||||||||||||||||||||||||
| As required by the Paperwork Reduction Act (PRA) of 1995, 44 U.S.C. § 3501-3521, the public reporting burden for the following performance indicators is estimated to average 1 hour per response, including the time for reviewing instructions, gathering and maintaining the data needed, and reviewing the collection of information. This form is approved under the Office of Management and Budget (OMB) control number OMB No: 0970-XXXX, expiration date is XX/XX/XXXX. An agency may not conduct or sponsor, and a person is not required to respond to, a collection of information unless it displays a currently valid OMB control number. | American Indian or Alaska Native (AIAN) | |||||||||||||||||||||||||||
| Asian | ||||||||||||||||||||||||||||
| Black or African American | ||||||||||||||||||||||||||||
| Native Hawaiian or Other Pacific Islander | ||||||||||||||||||||||||||||
| White | ||||||||||||||||||||||||||||
| Hispanic or Latino | ||||||||||||||||||||||||||||
| Other | ||||||||||||||||||||||||||||
| Not Reported | ||||||||||||||||||||||||||||
| Total number of clients enrolled in services by providers within the recipient’s multidisciplinary network by client current gender identity | NOTE: Award recipients will be required to obtain this information from clients/patients utilizing NASEM’s recommended two-step question and to report information to OTIP in the aggregate. Write-In responses to “I use a different term: [free text]” will not be provided to OTIP. Rather, the recipients will report the total number of individuals who elected to write in an option. “Not Reported” will reflect the count of clients/patients who selected “Prefer not to answer". See Reporting Reference Guide for additional operational guidance. | |||||||||||||||||||||||||||
| Female | ||||||||||||||||||||||||||||
| Male | ||||||||||||||||||||||||||||
| Transgender | ||||||||||||||||||||||||||||
| Please reference the Reporting Reference Guide (p.X-XX) to populate this table. | Two-Spirit | |||||||||||||||||||||||||||
| Different term | ||||||||||||||||||||||||||||
| Don’t know | ||||||||||||||||||||||||||||
| Not Reported | ||||||||||||||||||||||||||||
| Total number of clients enrolled in services by providers within the recipient’s multidisciplinary network by client sexual orientation | ||||||||||||||||||||||||||||
| Lesbian or gay | NOTE: Award recipients will be required to obtain this information from clients/patients utilizing NASEM’s recommended question and to report information to OTIP in the aggregate. Write-In responses to “I use a different term: [free text]” will not be provided to OTIP. Rather, the recipients will report the total number of individuals who elected to write in an option. “Not Reported” will reflect the count of clients/patients who selected “Prefer not to answer". See Reporting Reference Guide for additional operational guidance. | |||||||||||||||||||||||||||
| Straight, that is, not gay or lesbian | ||||||||||||||||||||||||||||
| Bisexual | ||||||||||||||||||||||||||||
| Two-Spirit | ||||||||||||||||||||||||||||
| Different term | ||||||||||||||||||||||||||||
| (Don’t know) | ||||||||||||||||||||||||||||
| Not Reported | ||||||||||||||||||||||||||||
| Total number of clients enrolled in services by providers within the recipient’s multidisciplinary network by client disability status | ||||||||||||||||||||||||||||
| Ambulatory Difficulty | ||||||||||||||||||||||||||||
| Cognitive Difficulty | ||||||||||||||||||||||||||||
| Hearing Difficulty | ||||||||||||||||||||||||||||
| Independent Living Difficulty | ||||||||||||||||||||||||||||
| Self-Care Difficulty | ||||||||||||||||||||||||||||
| Vision Difficulty | ||||||||||||||||||||||||||||
| Not Reported | ||||||||||||||||||||||||||||
| Total number of clients enrolled in services by providers within the recipient’s multidisciplinary network by client preferred language | ||||||||||||||||||||||||||||
| Prefer to be served in English | ||||||||||||||||||||||||||||
| Prefer to be served in a language other than English | ||||||||||||||||||||||||||||
Sheet 3: Q. HTRP
|
|
||||||||||||||||||||||||||||
| Human Trafficking Response Protocol (HTRP) | ||||||||||||||||||||||||||||
| Grant Recipient Name: | Q1 | Q2 | Q3 | Q4 | ||||||||||||||||||||||||
| Grant Number: | number | number | number | number | ||||||||||||||||||||||||
| Report Period: | Implementation Summary | Total number of providers coordinating care within the recipient's multidisciplinary network | ||||||||||||||||||||||||||
| Number of clients screened by providers within multidisciplinary network | ||||||||||||||||||||||||||||
| Number of clients identified as potential victims of HT based on screening conducted by providers within recipient’s multidisciplinary network by type of trafficking experienced |
||||||||||||||||||||||||||||
| Sex | ||||||||||||||||||||||||||||
| As required by the Paperwork Reduction Act (PRA) of 1995, 44 U.S.C. § 3501-3521, the public reporting burden for the following performance indicators is estimated to average 2.5 hours per response, including the time for reviewing instructions, gathering and maintaining the data needed, and reviewing the collection of information. This form is approved under the Office of Management and Budget (OMB) control number OMB No: 0970-XXXX, expiration date is XX/XX/XXXX. An agency may not conduct or sponsor, and a person is not required to respond to, a collection of information unless it displays a currently valid OMB control number. | Labor | |||||||||||||||||||||||||||
| Sex and Labor | ||||||||||||||||||||||||||||
| Not Reported | ||||||||||||||||||||||||||||
| Number of clients enrolled in services by providers within recipient’s multidisciplinary network by type of trafficking experienced |
||||||||||||||||||||||||||||
| Sex | ||||||||||||||||||||||||||||
| Labor | ||||||||||||||||||||||||||||
| Sex and Labor | ||||||||||||||||||||||||||||
| Not Reported | ||||||||||||||||||||||||||||
| Total number of clients referred to providers within the recipient’s multidisciplinary network | ||||||||||||||||||||||||||||
| Total number of clients referred to providers external to the recipient’s multidisciplinary network | ||||||||||||||||||||||||||||
| Check all that apply | ||||||||||||||||||||||||||||
| Q1 | Q2 | Q3 | Q4 | |||||||||||||||||||||||||
| Barriers to Service Delivery and Implementation | Client/Patient Constraints | |||||||||||||||||||||||||||
| Affordability | ||||||||||||||||||||||||||||
| Accommodation | ||||||||||||||||||||||||||||
| Availability | ||||||||||||||||||||||||||||
| Accessibility | ||||||||||||||||||||||||||||
| Acceptability | ||||||||||||||||||||||||||||
| Not Specified | ||||||||||||||||||||||||||||
| Safety Concerns | ||||||||||||||||||||||||||||
| Feelings of No Support and Isolation | ||||||||||||||||||||||||||||
| Excluded from key decision-making opportunities | ||||||||||||||||||||||||||||
| Experiences of bias or discrimination as it pertains to [insert leadership, practice, policy] (e.g., gender, race, ethnicity, sexual orientation) |
||||||||||||||||||||||||||||
| Feeling undervalued or not perceived as a leader in my organization | ||||||||||||||||||||||||||||
| Lack of authority to use new skills in current position | ||||||||||||||||||||||||||||
| Ineffective Coordination with Agencies and Providers | ||||||||||||||||||||||||||||
| Difficulty coordinating with benefits-issuing agencies | ||||||||||||||||||||||||||||
| Difficulty establishing/maintaining multidisciplinary team (MDT) | ||||||||||||||||||||||||||||
| Lack of data sharing among organizations | ||||||||||||||||||||||||||||
| Lack of shared responsibility across organizational collaborators | ||||||||||||||||||||||||||||
| Need for partnership building with other orgs | ||||||||||||||||||||||||||||
| Variation in mission/regulatory frameworks when partnering with other organizations | ||||||||||||||||||||||||||||
| Lack of Adequate Funding | ||||||||||||||||||||||||||||
| Lack of Adequate Resources | ||||||||||||||||||||||||||||
| Competing priorities | ||||||||||||||||||||||||||||
| Frequent staff turnover | ||||||||||||||||||||||||||||
| Lack of senior leadership support | ||||||||||||||||||||||||||||
| Lack of support/accountability from frontline staff | ||||||||||||||||||||||||||||
| Lack of time to implement changes | ||||||||||||||||||||||||||||
| Lack of urgency | ||||||||||||||||||||||||||||
| Shortage of key personnel (including clinician shortage issues) | ||||||||||||||||||||||||||||
| Lack of Adequate Training | ||||||||||||||||||||||||||||
| Lack of accessible research/information | ||||||||||||||||||||||||||||
| Lack of training for staff on how to implement change | ||||||||||||||||||||||||||||
| Lack of Formal Rules and Regulations | ||||||||||||||||||||||||||||
| Lack of Procedures | ||||||||||||||||||||||||||||
| Lack of Knowledge of Victims’ Rights | ||||||||||||||||||||||||||||
| Public Health Concerns | ||||||||||||||||||||||||||||
Sheet 4: Q. Network Providers
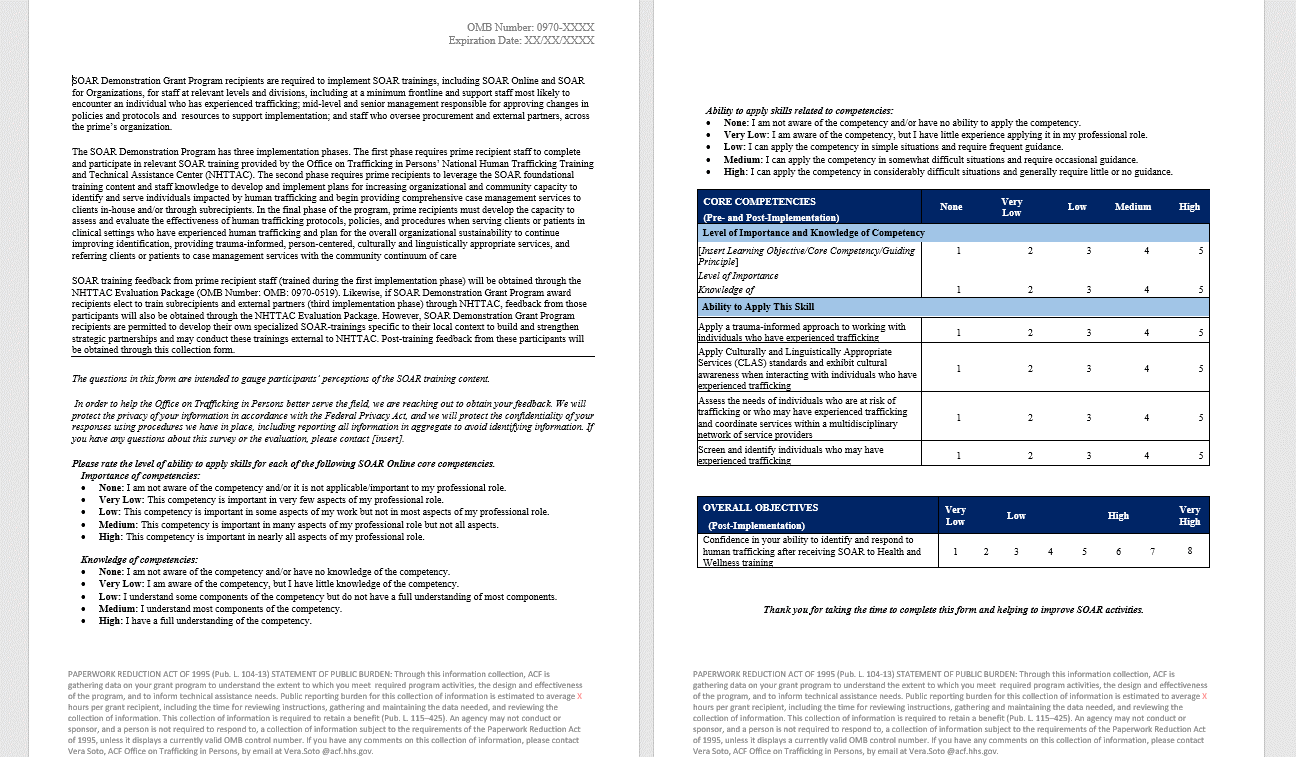
Sheet 5: Q. Training Feedback Form
| Separate PDF based form; obtained through SOAR/NHTTAC implementation | ||||||||||||
| See TAB F: SOAR Demonstration Grant Participant Training Feedback Form | ||||||||||||
| Average Burden Hours per Response: 0.75 hours | ||||||||||||
|
||||||||||||
Sheet 6: FY.Categories of Assistance
| File Type | application/vnd.openxmlformats-officedocument.spreadsheetml.sheet |
| File Modified | 0000-00-00 |
| File Created | 0000-00-00 |
© 2026 OMB.report | Privacy Policy