Federal IDR Process for Services relating to Nonparticipating Providers or Nonparticipating Emergency Facilities
No Surprise Act: IDR Process
14. Online PPDR Initiation Form
Federal IDR Process for Services relating to Nonparticipating Providers or Nonparticipating Emergency Facilities
OMB: 1210-0169
OMB Control Number: 0938-NEW
Expiration Date: XX/XXXX
APPENDIX 14
Online Patient-Provider Dispute Resolution Initiation Form
PPDR Initiation Screen Language
Expiration Date: 04/30/2022
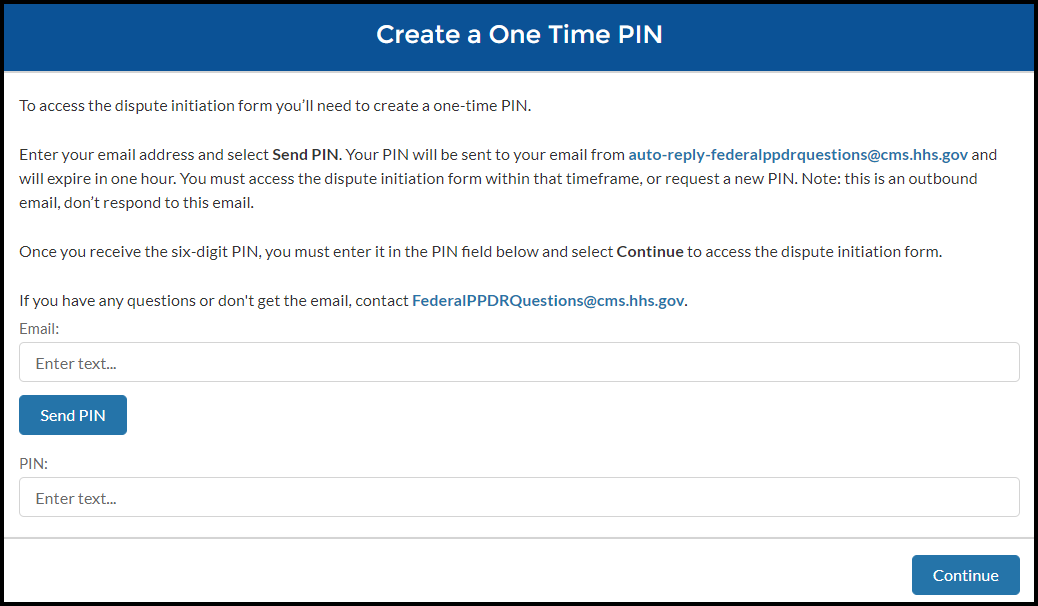
Create a One Time Pin
To access the dispute initiation form you’ll need to create a one-time PIN.
Enter your email address and select Send PIN. Your PIN will be sent to your email from auto-reply-federalppdrquestions@cms.hhs.gov and will expire in one hour. You must access the dispute initiation form within that timeframe, or request a new PIN. Note: this is an outbound email, don’t respond to this email.
Once you receive the six-digit PIN, you must enter it in the PIN field below and select Continue to access the dispute initiation form.
If you have any questions or don’t get the email, contact FederalPPDRQuestions@cms.hhs.gov.
Email: (field label)
![]()
Send PIN (button)
![]()
PIN: (field label)
![]()
The Email and/or PIN provided are not valid. (error message)
Continue (button)
![]()
Welcome Page
OMB Expiration Date
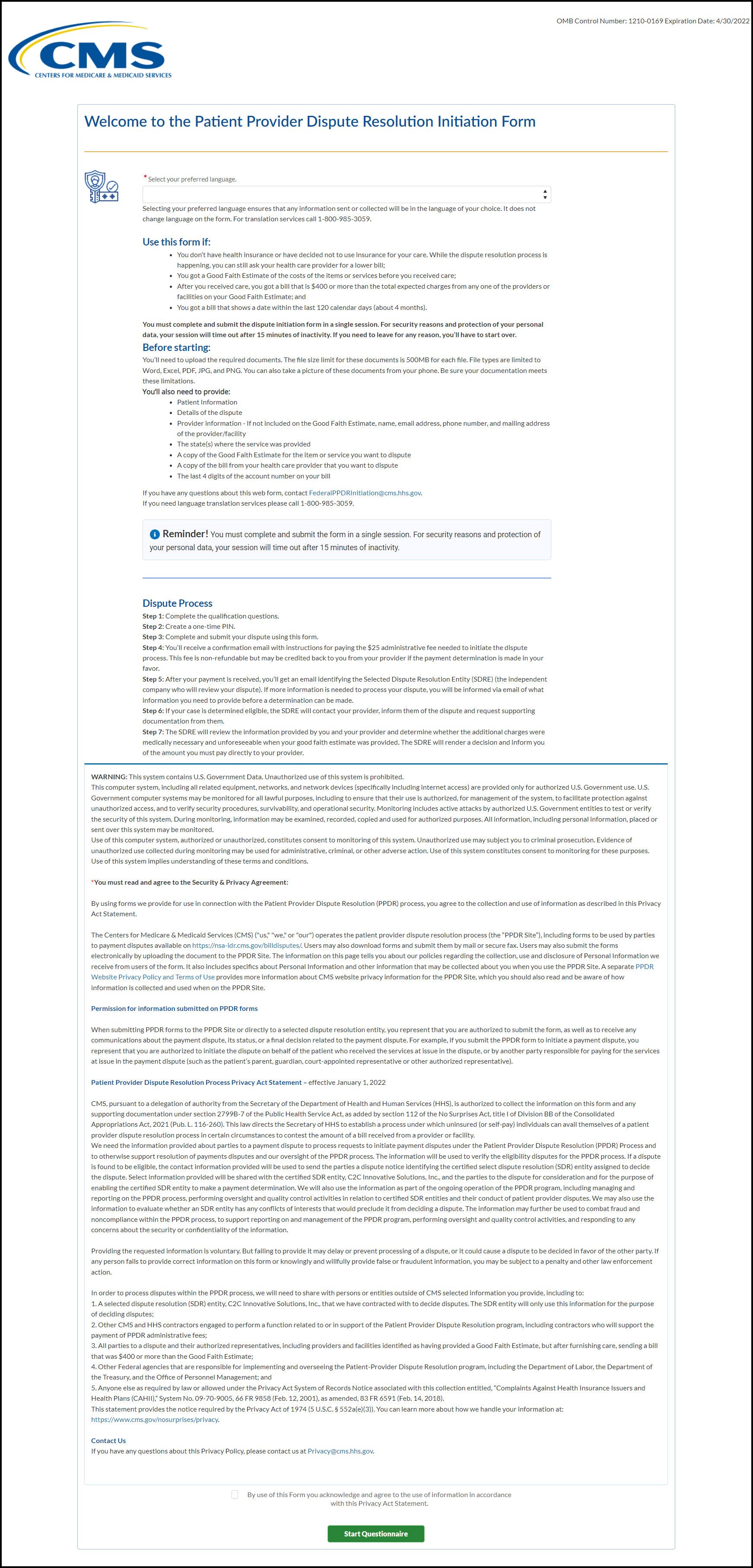
Welcome to the Patient Provider Dispute Resolution Initiation Form
*Select your preferred language.
Language (drop down)

English, Spanish (drop down selections)
Selecting your preferred language ensures that any information sent or collected will be in the language of your choice. It does not change language on the form. For translation services call 1-800-985-3059.
Si necesita servicios de traducción de idiomas, llame al 1-800-985-3059.
Use this form if:
You don’t have health insurance or have decided not to use insurance for your care. While the dispute resolution process is happening, you can still ask your health care provider for a lower bill;
You got a Good Faith Estimate of the costs of the items or services before you received care;
After you received care, you got a bill that is $400 or more than the total expected charges from any one of the providers or facilities on your Good Faith Estimate; and
You got a bill that shows a date within the last 120 calendar days (about 4 months).
You must complete and submit the dispute initiation form in a single session. For security reasons and protection of your personal data, your session will time out after 15 minutes of inactivity. If you need to leave for any reason, you’ll have to start over.
Before starting:
You’ll need to upload the required documents. The file size limit for these documents is 500MB for each file. File types are limited to Word, Excel, PDF, JPG, and PNG. You can also take a picture of these documents from your phone. Be sure your documentation meets these limitations.
You’ll also need to provide:
Patient information
Details of the dispute
Provider information - If not included on the Good Faith Estimate, name, email address, phone number, and mailing address of the provider/facility
The state(s) where the service was provided
A copy of the Good Faith Estimate for the item or service you want to dispute
A copy of the bill from your health care provider that you want to dispute
The last 4 digits of the account number on your bill
If you have any questions about this web form, contact FederalPPDRInitiation@cms.hhs.gov.
Reminder:

Dispute process:
Step 1: Create a one-time PIN. (completed)
Step 2: Complete the qualification questions.
Step 3: Complete and submit your dispute using this form.
Step 4: You’ll receive a confirmation email with instructions for paying the $25 administrative fee needed to initiate the dispute process. This fee is non-refundable but may be credited back to you from your provider if the payment determination is made in your favor.
Step 5: After your payment is received, you’ll get an email identifying the Selected Dispute Resolution Entity (SDRE) (the independent company who will review your dispute). If more information is needed to process your dispute, you will be informed via email of what information you need to provide before a determination can be made.
Step 6: If your case is determined eligible, the SDRE will contact your provider, inform them of the dispute and request supporting documentation from them.
Step 7: The SDRE will review the information provided by you and your provider and determine whether the additional charges were medically necessary and unforeseeable when your good faith estimate was provided. The SDRE will render a decision and inform you of the amount you must pay directly to your provider.
WARNING:
This system
contains U.S. Government Data. Unauthorized use of this system is
prohibited.
This
computer system, including all related equipment, networks, and
network devices (specifically including internet access) are provided
only for authorized U.S. Government use. U.S. Government computer
systems may be monitored for all lawful purposes, including to ensure
that their use is authorized, for management of the system, to
facilitate protection against unauthorized access, and to verify
security procedures, survivability, and operational security.
Monitoring includes active attacks by authorized U.S. Government
entities to test or verify the security of this system. During
monitoring, information may be examined, recorded, copied and used
for authorized purposes. All information, including personal
information, placed or sent over this system may be monitored.
Use
of this computer system, authorized or unauthorized, constitutes
consent to monitoring of this system. Unauthorized use may subject
you to criminal prosecution. Evidence of unauthorized use collected
during monitoring may be used for administrative, criminal, or other
adverse action. Use of this system constitutes consent to monitoring
for these purposes.
Use
of this system implies understanding of these terms and conditions.
*You must read and agree to the Security & Privacy Agreement:
By using forms, we provide for use in connection with the Patient Provider Dispute Resolution (PPDR) process, you agree to the collection and use of information as described in this Privacy Act Statement.
The Centers for Medicare & Medicaid Services (CMS) ("us," "we," or "our") operates the patient provider dispute resolution process (the “PPDR Site”), including forms to be used by parties to payment disputes available on https://nsa-idr.cms.gov/billdisputes/. Users may also download forms and submit them by mail or secure fax. Users may also submit the forms electronically by uploading the document to the PPDR Site. The information on this page tells you about our policies regarding the collection, use and disclosure of Personal Information we receive from users of the form. It also includes specifics about Personal Information and other information that may be collected about you when you use the PPDR Site. A separate [PPDR Website Privacy Policy and Terms of Use] provides more information about CMS website privacy information for the PPDR Site, which you should also read and be aware of how information is collected and used when on the PPDR Site.
Permission for information submitted on PPDR forms
When submitting PPDR forms to the PPDR Site or directly to a selected dispute resolution entity, you represent that you are authorized to submit the form, as well as to receive any communications about the payment dispute, its status, or a final decision related to the payment dispute. For example, if you submit the PPDR form to initiate a payment dispute, you represent that you are authorized to initiate the dispute on behalf of the patient who received the services at issue in the dispute, or by another party responsible for paying for the services at issue in the payment dispute (such as the patient’s parent, guardian, court-appointed representative or other authorized representative).
Patient Provider Dispute Resolution Process Privacy Act Statement – effective January 1, 2022
CMS, pursuant to a delegation of authority from the Secretary of the Department of Health and Human Services (HHS), is authorized to collect the information on this form and any supporting documentation under section 2799B-7 of the Public Health Service Act, as added by section 112 of the No Surprises Act, title I of Division BB of the Consolidated Appropriations Act, 2021 (Pub. L. 116-260). This law directs the Secretary of HHS to establish a process under which uninsured (or self-pay) individuals can avail themselves of a patient provider dispute resolution process in certain circumstances to contest the amount of a bill received from a provider or facility.
We need the information provided about parties to a payment dispute to process requests to initiate payment disputes under the Patient Provider Dispute Resolution (PPDR) Process and to otherwise support resolution of payments disputes and our oversight of the PPDR process. The information will be used to verify the eligibility disputes for the PPDR process. If a dispute is found to be eligible, the contact information provided will be used to send the parties to a dispute a notice identifying the certified select dispute resolution (SDR) entity assigned to decide the dispute. Select information provided will be shared with the certified SDR entity, C2C Innovative Solutions, Inc., and the parties to the dispute for consideration and for the purpose of enabling the certified SDR entity to make a payment determination. We will also use the information as part of the ongoing operation of the PPDR program, including managing and reporting on the PPDR process, performing oversight and quality control activities in relation to certified SDR entities and their conduct of patient provider disputes. We may also use the information to evaluate whether an SDR entity has any conflicts of interests that would preclude it from deciding a dispute. The information may further be used to combat fraud and noncompliance within the PPDR process, to support reporting on and management of the PPDR program, performing oversight and quality control activities, and responding to any concerns about the security or confidentiality of the information.
Providing the requested information is voluntary. But failing to provide it may delay or prevent processing of a dispute, or it could cause a dispute to be decided in favor of the other party. If any person fails to provide correct information on this form or knowingly and willfully provide false or fraudulent information, you may be subject to a penalty and other law enforcement action.
In order to process disputes within the PPDR process, we will need to share with persons or entities outside of CMS selected information you provide, including to:
A selected dispute resolution (SDR) entity, C2C Innovative Solutions, Inc., that we have contracted with to decide disputes. The SDR entity will only use this information for the purpose of deciding disputes;
Other CMS and HHS contractors engaged to perform a function related to or in support of the Patient Provider Dispute Resolution program, including contractors who will support the payment of PPDR administrative fees;
All parties to a dispute and their authorized representatives, including providers and facilities identified as having provided a Good Faith Estimate, but after furnishing care, sending a bill that was $400 or more than the Good Faith Estimate;
Other Federal agencies that are responsible for implementing and overseeing the Patient-Provider Dispute Resolution program, including the Department of Labor, the Department of the Treasury, and the Office of Personnel Management; and
Anyone else as required by law or allowed under the Privacy Act System of Records Notice associated with this collection entitled, “Complaints Against Health Insurance Issuers and Health Plans (CAHII),” System No. 09-70-9005, 66 FR 9858 (Feb. 12, 2001), as amended, 83 FR 6591 (Feb. 14, 2018).
This statement provides the notice required by the Privacy Act of 1974 (5 U.S.C. § 552a(e)(3)). You can learn more about how we handle your information at: https://www.cms.gov/nosurprises/privacy .
Contact Us
If you have any questions about this Privacy Act Statement, please contact us at Privacy@cms.hhs.gov.
By use of this Form you acknowledge and agree to the use of information in accordance with this Privacy Act Statement.
![]()
![]()
*You must agree to the security statement to proceed. (error message)
Start Questionnaire (button)
![]()
Qualification Questions
Page 1:
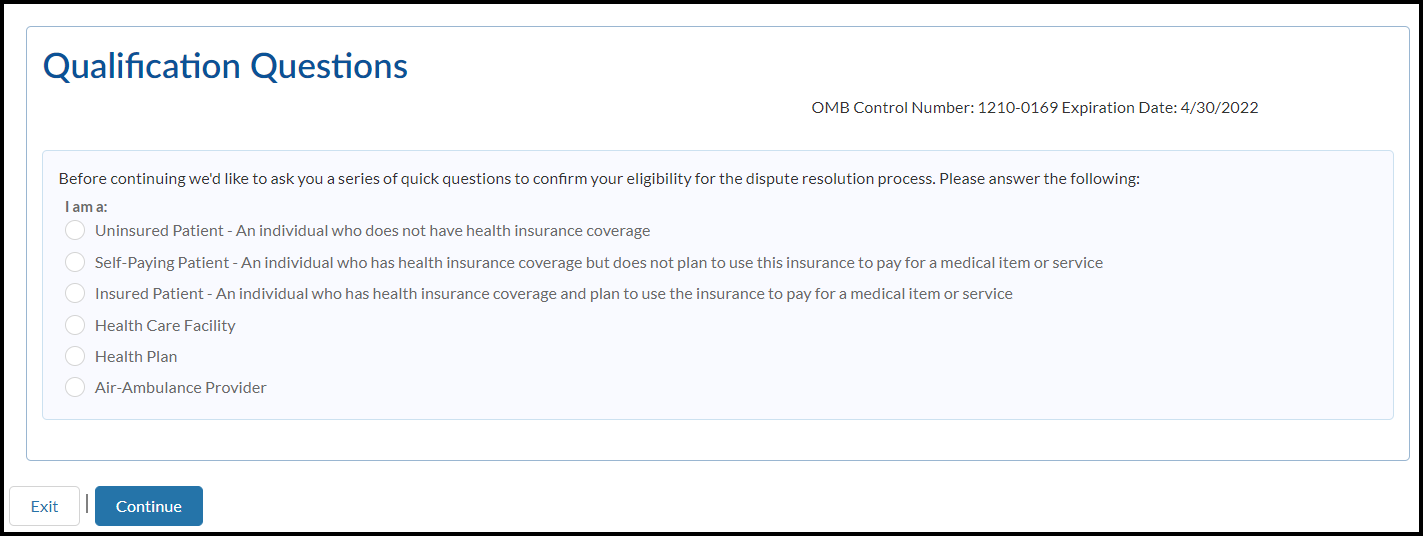
Qualification Questions
OMB Expiration Date
Before continuing we'd like to ask you a series of quick questions to confirm your eligibility for the dispute resolution process. Please answer the following:
I am a:
Radio-button Selections:
Uninsured Patient – An individual who does not have health insurance coverage
Self-Paying Patient – An individual who has health insurance coverage but does not plan to use this insurance to pay for ma medical item or service
Insured patient – An individual who has health insurance coverage and plan to use the insurance to pay for a medical item or service
Health Care Facility
Health Plan
Air-Ambulance Provider
Exit (button)
![]()
Continue (button)
![]()
 Page
2:
Page
2:
Qualification Questions
OMB Expiration Date
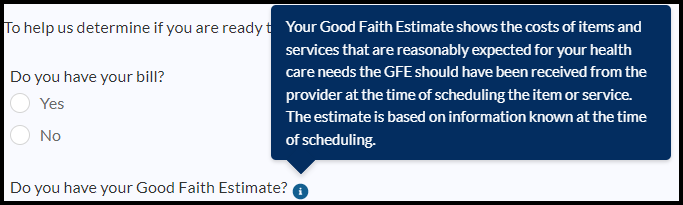
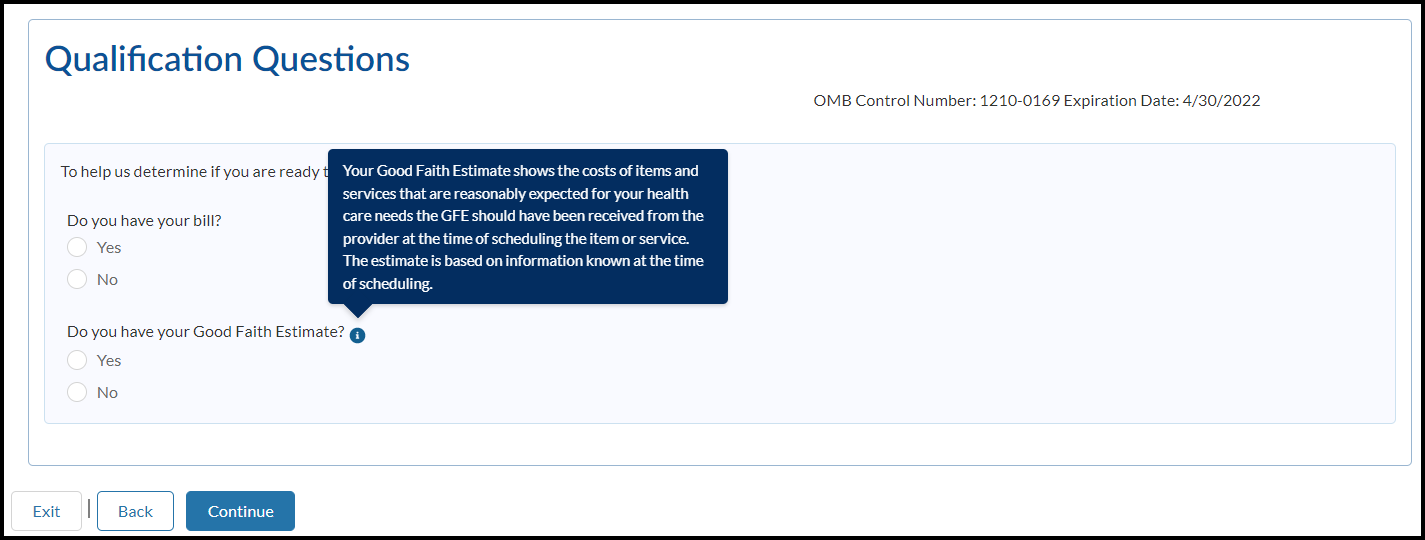
To help us determine if you’re ready to submit your dispute, answer the following:
Do you have your bill?
Yes
No
![]()
Do you have your Good Faith Estimate?
Yes
No
![]()
Information (bubble)
Exit (button)
![]()
Back (button)
![]()
Continue (button)
![]()
Information bubble: Your Good Faith Estimate shows the costs of items and services that are reasonably expected for your health care needs and you should’ve received one from the provider at the time of scheduling the item or service. The estimate is based on information known at the time of scheduling.
Page 3:
Qualification Questions
OMB Expiration Date
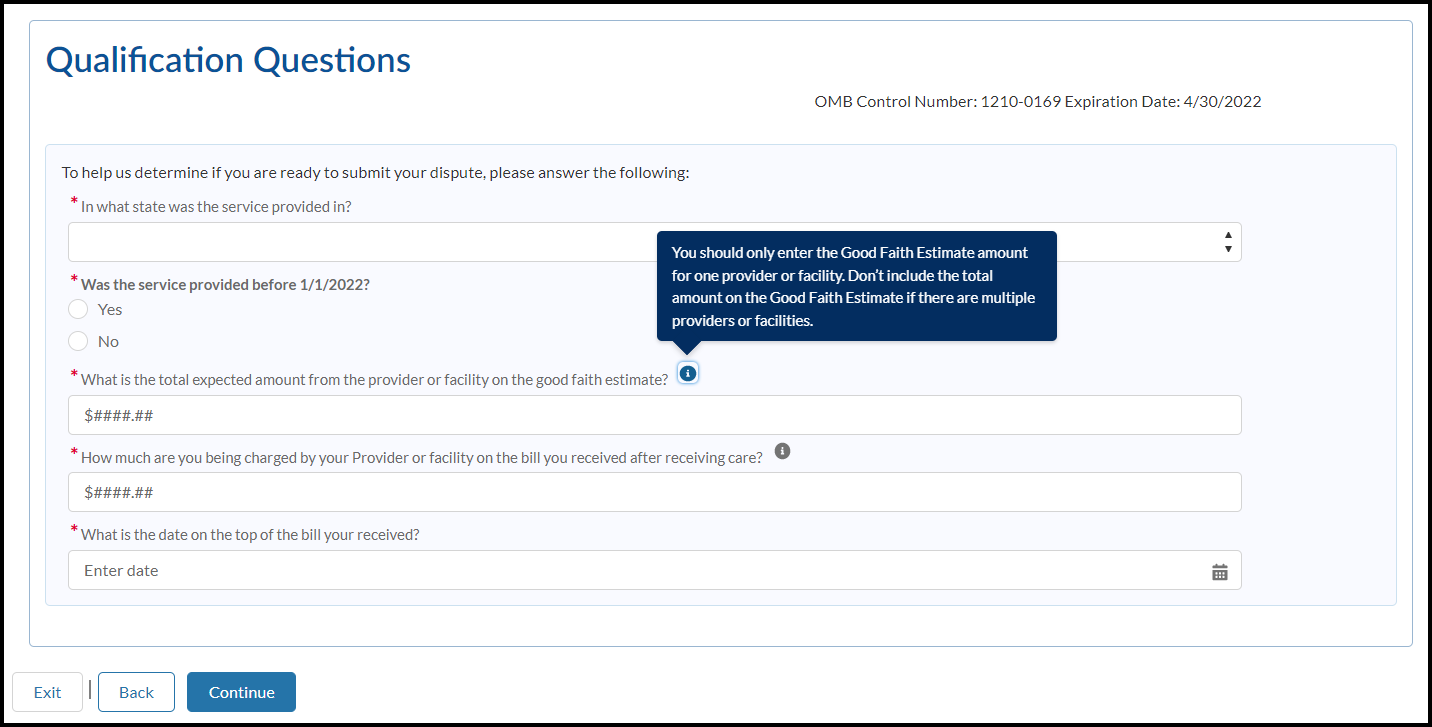
To help us determine if you’re ready to submit your dispute, answer the following:
*In what state was the service provided in?
![]()
All 50 states abbreviations + territories (drop down selections)
*Was the service provided before 1/1/2022?
Yes
No
*What is the total expected amount from the provider or facility on the Good Faith Estimate?

*How much are you being charged by your provider or facility on the bill you received after receiving care?

*What is the date on the top of the bill you received?
Enter date (help text)
![]()
Information bubble (GFE): You should only enter the Good Faith Estimate amount for ONE provider or facility. Do not include the total amount on the Good Faith Estimate if there are multiple providers or facilities.
Information Bubble (provider bill): You can only dispute the charges from the provider that supplied the GFE. You cannot dispute the charges of providers for which you did not get a GFE.
Exit (button)
![]()
Back (button)
![]()
Continue (button)
![]()
Error messages
Based on selections – error messages will appear per validation.
You’re not eligible for dispute resolution. Only uninsured patients or patients with insurance but who choose not to file a claim for their item or service (self-pay patients) are eligible to initiate the patient provider dispute resolution process. Please visit cms.gov/nosurprises/consumers for more information.
You’re missing required documents. You won’t be able to initiate a dispute without having both your Good Faith Estimate and your provider's bill.
You’re not eligible for dispute resolution because the difference between the Good Faith Estimate for the service from the provider or facility and the actual billed amount is less than $400. Contact your health care provider to negotiate your bill or ask for financial assistance.
Y



 ou’re
not eligible for dispute resolution because the date of service you
provided is before 1/1/2022. Contact your health care provider to
negotiate your bill and ask for financial assistance.
ou’re
not eligible for dispute resolution because the date of service you
provided is before 1/1/2022. Contact your health care provider to
negotiate your bill and ask for financial assistance.
Patient Provider Dispute Resolution Initiation Form:
OMB Expiration Date
Page 1:
P rogress
Tracker: Patient Information | Provider Information | Read &
Sign | Confirmation
rogress
Tracker: Patient Information | Provider Information | Read &
Sign | Confirmation
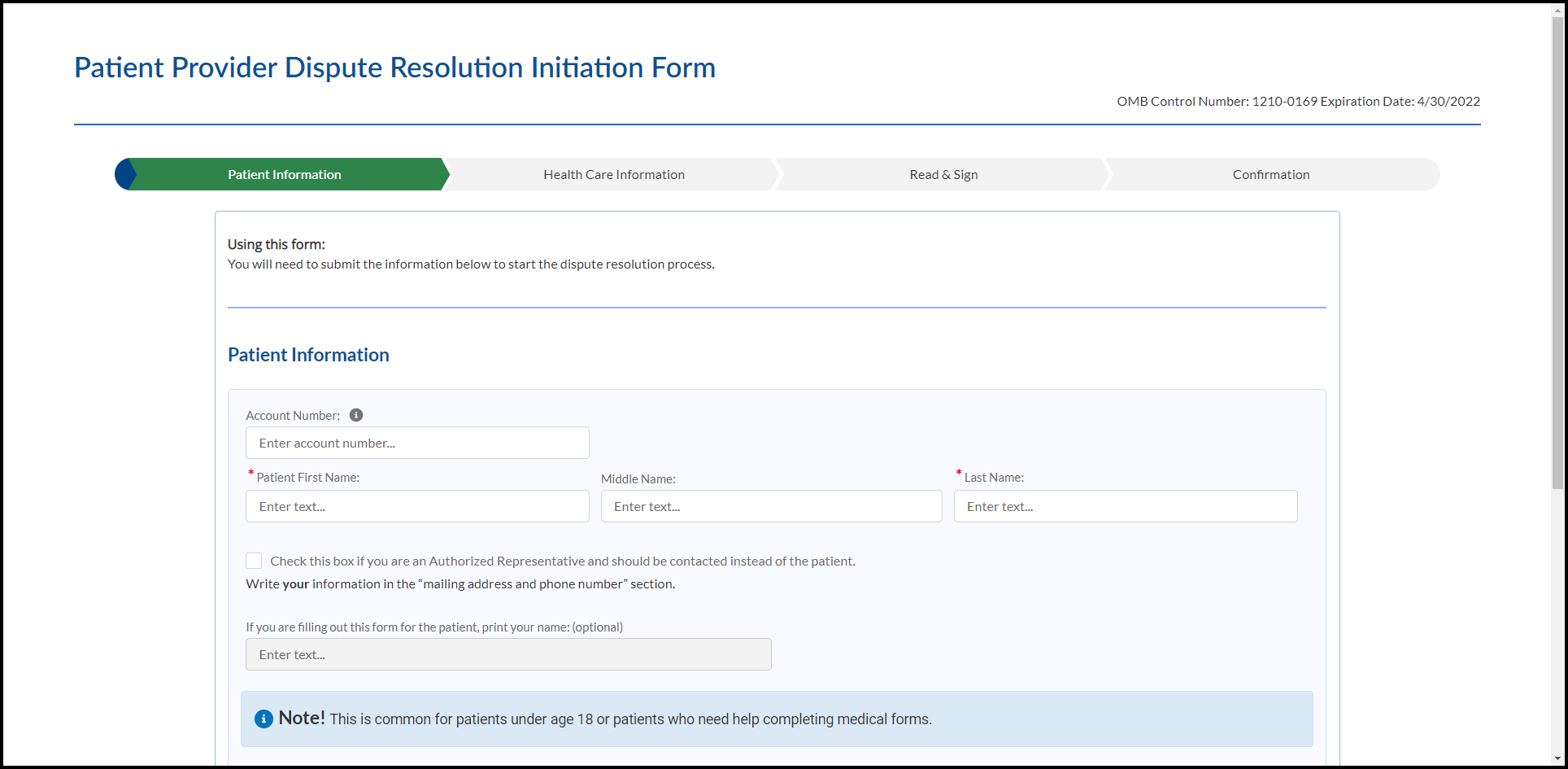
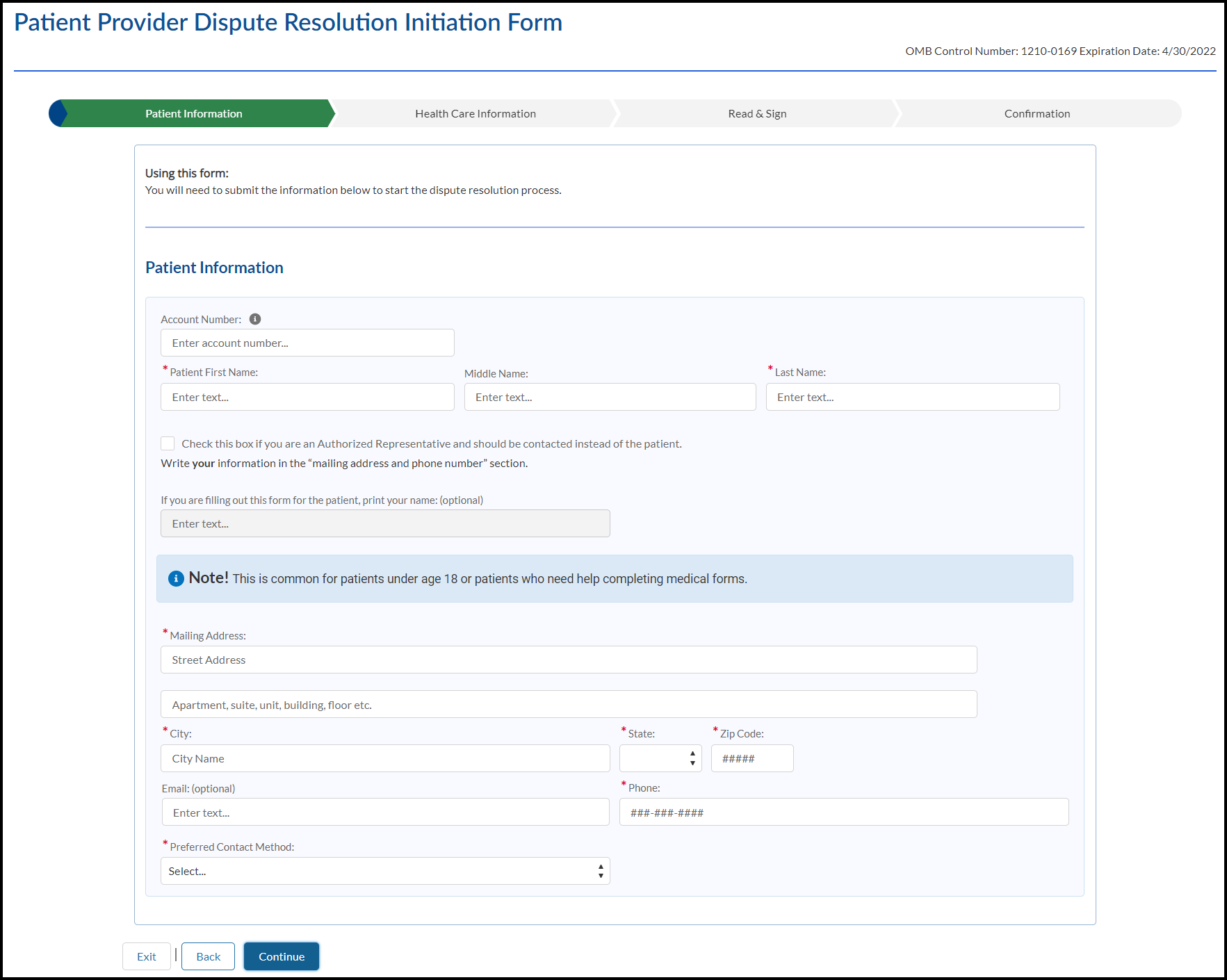
Using this form:
You will need to submit the information below to start the dispute resolution process.
Patient Information:
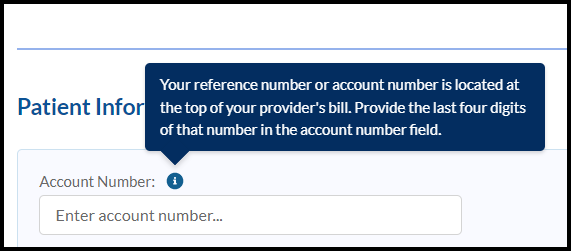
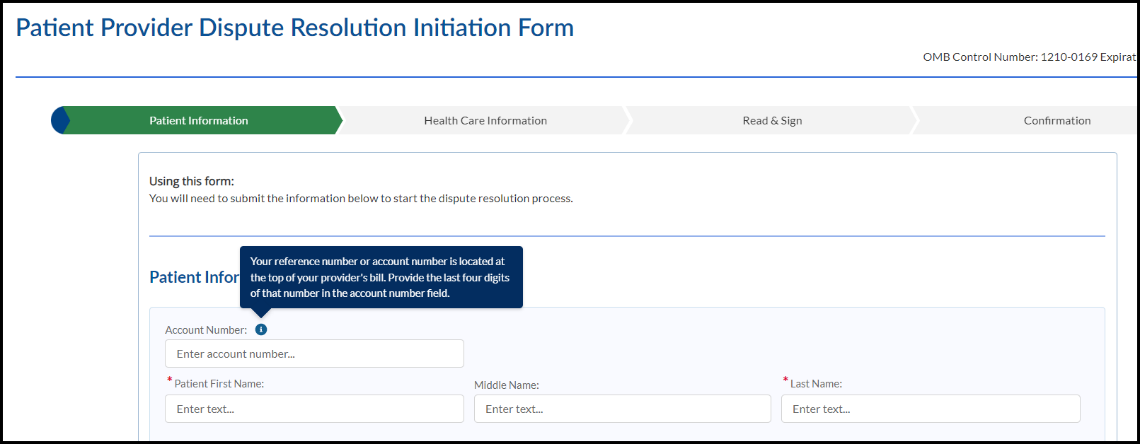
 Account
Number:
Account
Number:Enter account number (help text)
*Patient First Name:

Middle Name:
![]()
*Last Name:
![]()
Check this box if you are an Authorized Representative and should be contacted instead of the patient. Write your information in the “mailing address and phone number” section.
![]()
If you are filling out this form for the patient, print your name: (optional)

Note! This is common for patients under age 18 or patients who need help completing medical forms.
![]()
*Mailing Address:
![]()
Apartment, suite, unit, building, floor etc.:
![]()
*City:

*State:
![]()
*Zip Code:
![]()
Email: (optional)
![]()
*Phone:
![]()
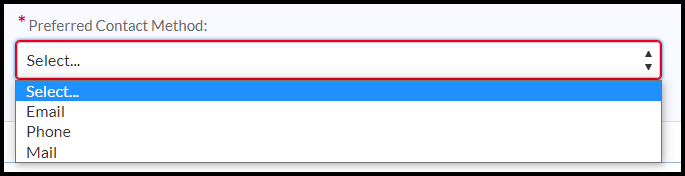
*Preferred Contact Method:
Select… (help text)
![]()
Email, Phone, Mail (drop down selections)
Exit (button)
![]()
Back (button)
![]()
Continue (button)
![]()
Page 2:
OMB Expiration Date
Progress Tracker: Patient Information | Provider Information | Read & Sign | Confirmation

Using this form:
You will need to submit the information below to start the dispute resolution process.
Health Care Provider Information
Provide the contact information for the health care provider that provided the item or performed the service. This should be on your Good Faith Estimate.
![]()
*Hosiptal, Facility or Group Name:
![]()
*Mailing Address:
![]()
Street Address
Apartment, suite, unit, building, floor, etc.
![]()
*City:
![]()
*State:
![]()
*Zip Code:
*Email:
![]()
![]()
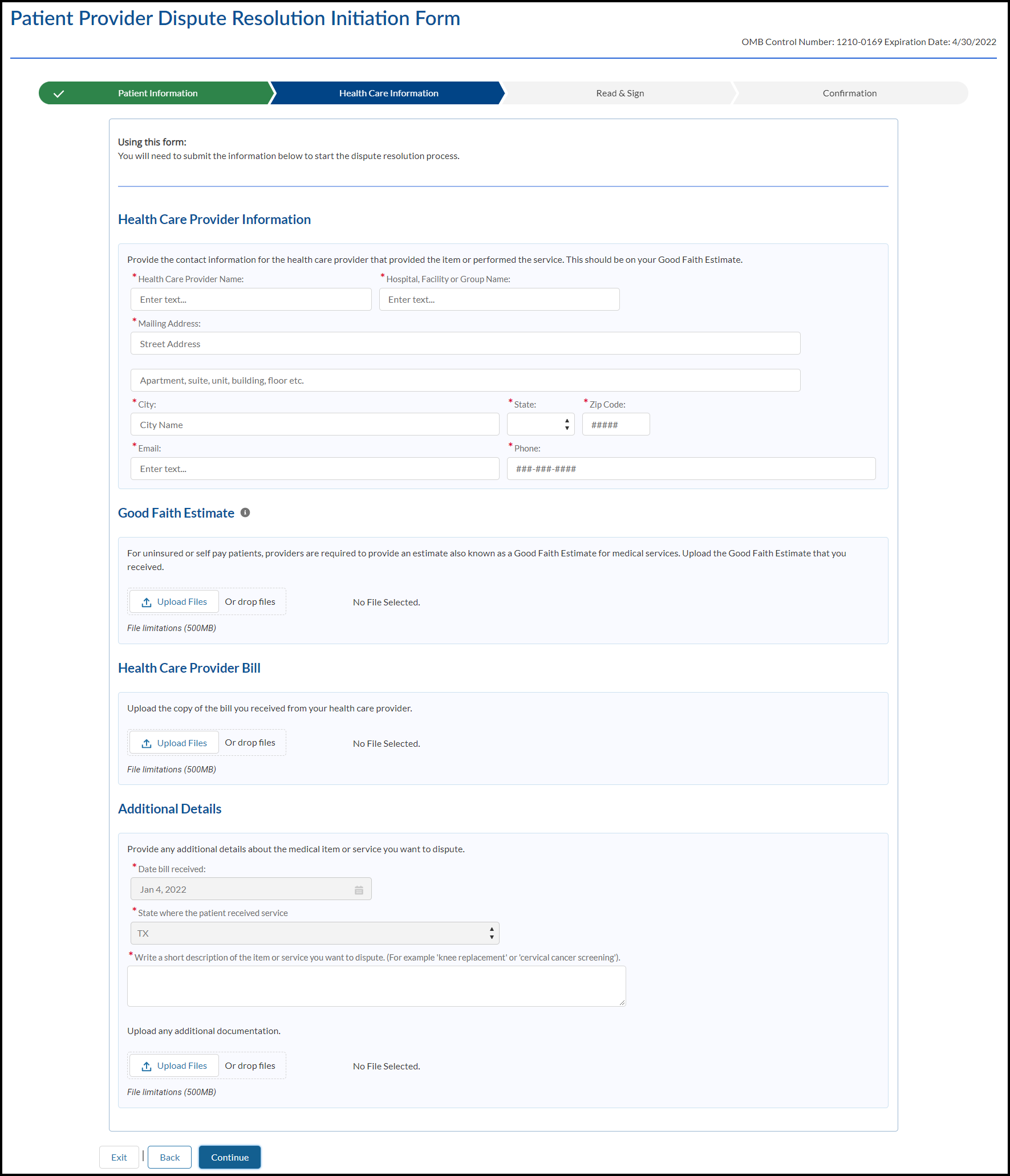
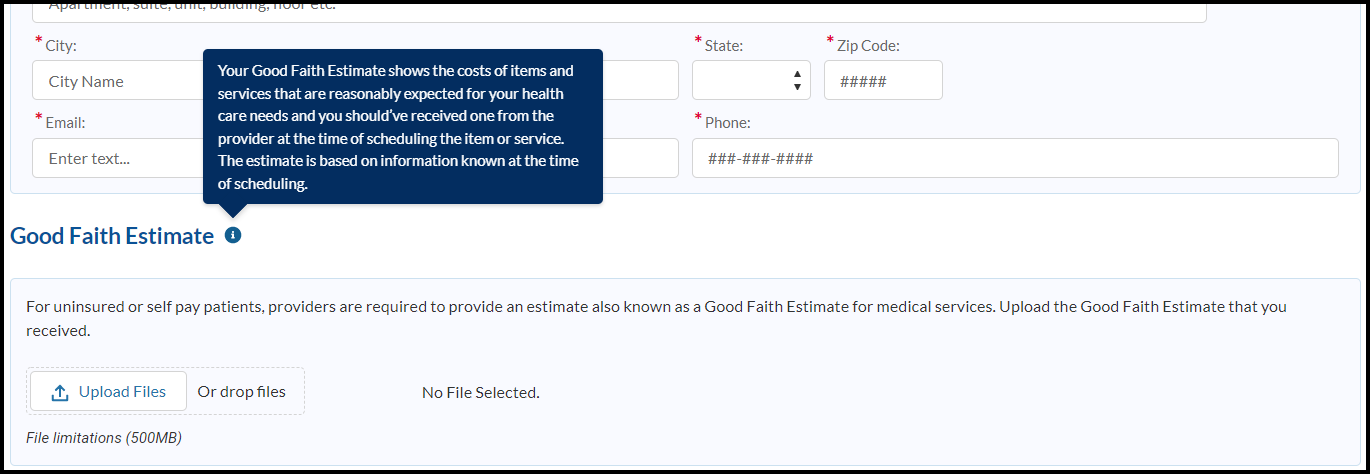
Good Faith Estimate
(Good Faith Estimate information bubble) Your Good Faith Estimate shows the costs of items and services that are reasonably expected for your health care needs and you should’ve received one from the provider at the time of scheduling the item or service. The estimate is based on information known at the time of scheduling.
For uninsured or self-pay patients, providers are required to provide an estimate also known as a Good Faith Estimate for medical services. You can only dispute the charges from the provider that supplied the GFE. You cannot dispute the charges of providers for which you did not get a GFE. Upload the Good Faith Estimate that you received.
Upload Files Or drop files (button)
![]()
File limitations (500MB)
![]()
Health Care Provider Bill
Upload the copy of the bill you received from your health care provider.

Upload Files or drop files (button)
![]()
No File Selected.
File limitations (500MB)
Additional Details
Provide any additional details about the medical item or service you want to dispute.
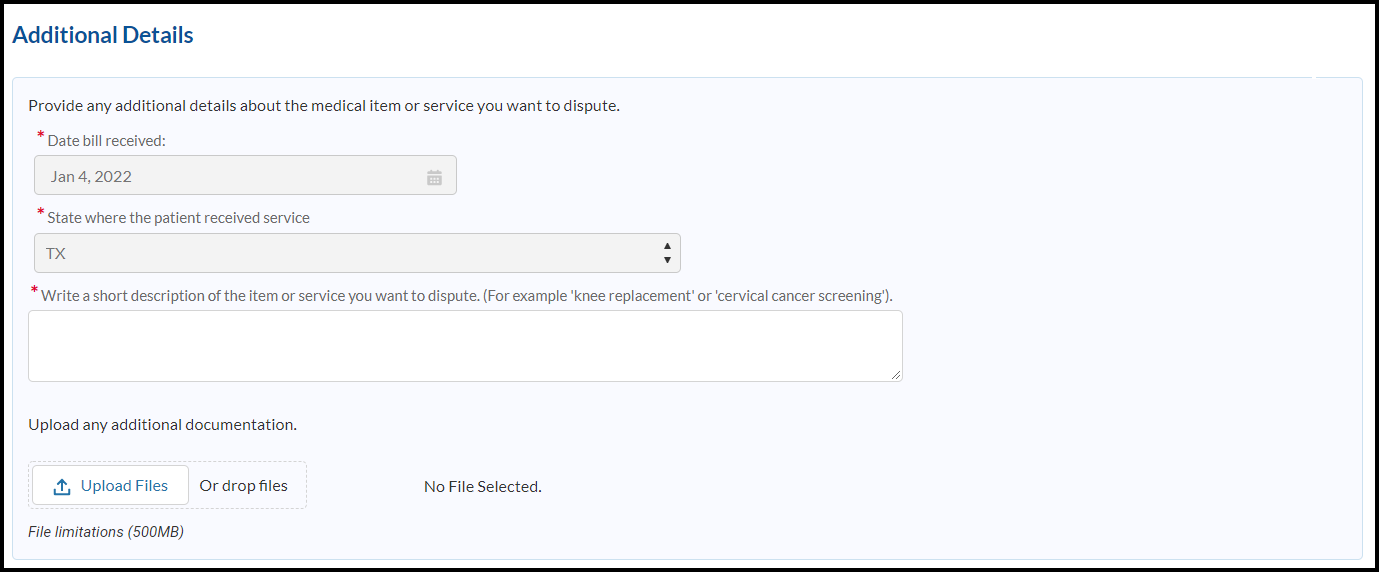
*Date bill received:
![]()
*State where the patient received service:
![]()
*Write a short description of the item or service you want to dispute. (For example, "knee replacement" or "cervical cancer screening")
![]()
Upload any additional documentation.
Upload Files Or drop files (button) Optional
No File Selected. (help text)
![]()
File limitations (500MB)
![]()
Exit (button)
![]()
Back (button)
![]()
Continue (button)
![]()
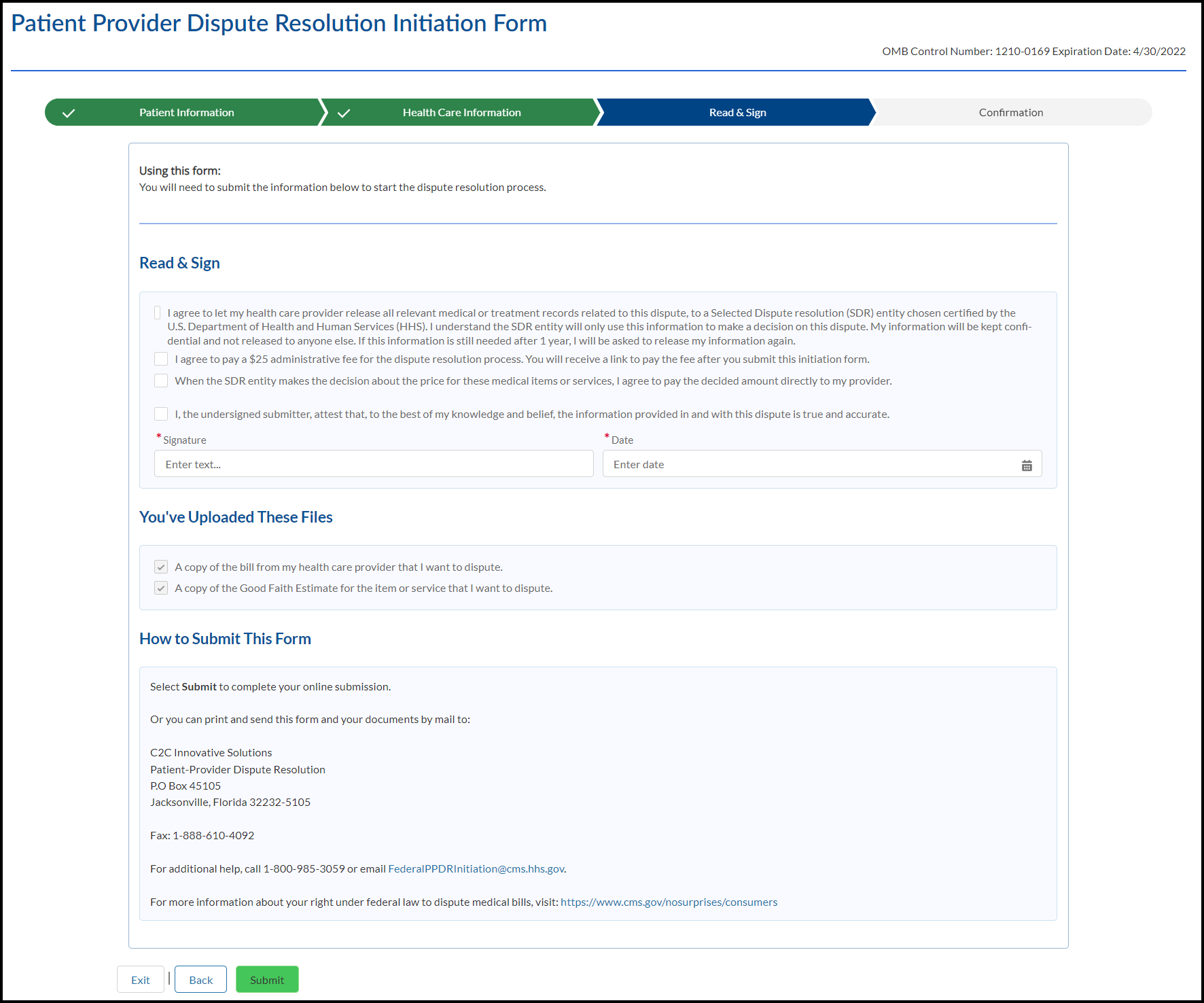
Read & Sign
OMB Expiration Date
Progress Tracker: Patient Information | Provider Information | Read & Sign | Confirmation

Using this form:
You will need to submit the information below to start the dispute resolution process.

Read and Sign
I agree to let my health care provider release all relevant medical or treatment records related to this dispute, to a Selected Dispute Resolution (SDR) entity chosen and certified by the U.S. Department of Health and Human Services (HHS). I understand the SDR entity will only use this information to make a decision on this dispute. My information will be kept confidential and not released to anyone else. If this information is still needed after 1 year, I will be asked to release my information again.
I agree to pay a non-refundable $25 administrative fee for the dispute resolution process. You will receive a link to pay the fee after you submit this initiation form.
When the SDR entity makes the decision about the price for these medical items or services, I agree to pay the decided amount directly to my provider.
I, the undersigned submitter, attest that, to the best of my knowledge and belief, the information provided in and with this dispute is true and accurate.
Signature
![]()
Date
![]()
You've uploaded these files
A copy of the bill from my health care provider or facility that I want to dispute.
![]()
A copy of the Good Faith Estimate for the item or service that I want to dispute.
![]()
![]()
How to submit this form
Select Submit to complete your online submission.
Or you can print and send this form and your documents by mail to:
C2C Innovative Solutions
Patient-Provider Dispute Resolution
P.O Box 45105
Jacksonville, Florida 32232-5105
Fax: 1-888-610-4092
For additional help, call 1-800-985-3059 or email FederalPPDRInitiation@cms.hhs.gov
For more information about your right under federal law to dispute medical bills, visit: www.cms.gov/nosurprises/consumers
Exit (button)
![]()
Back (button)
![]()
Submit (button)
![]()
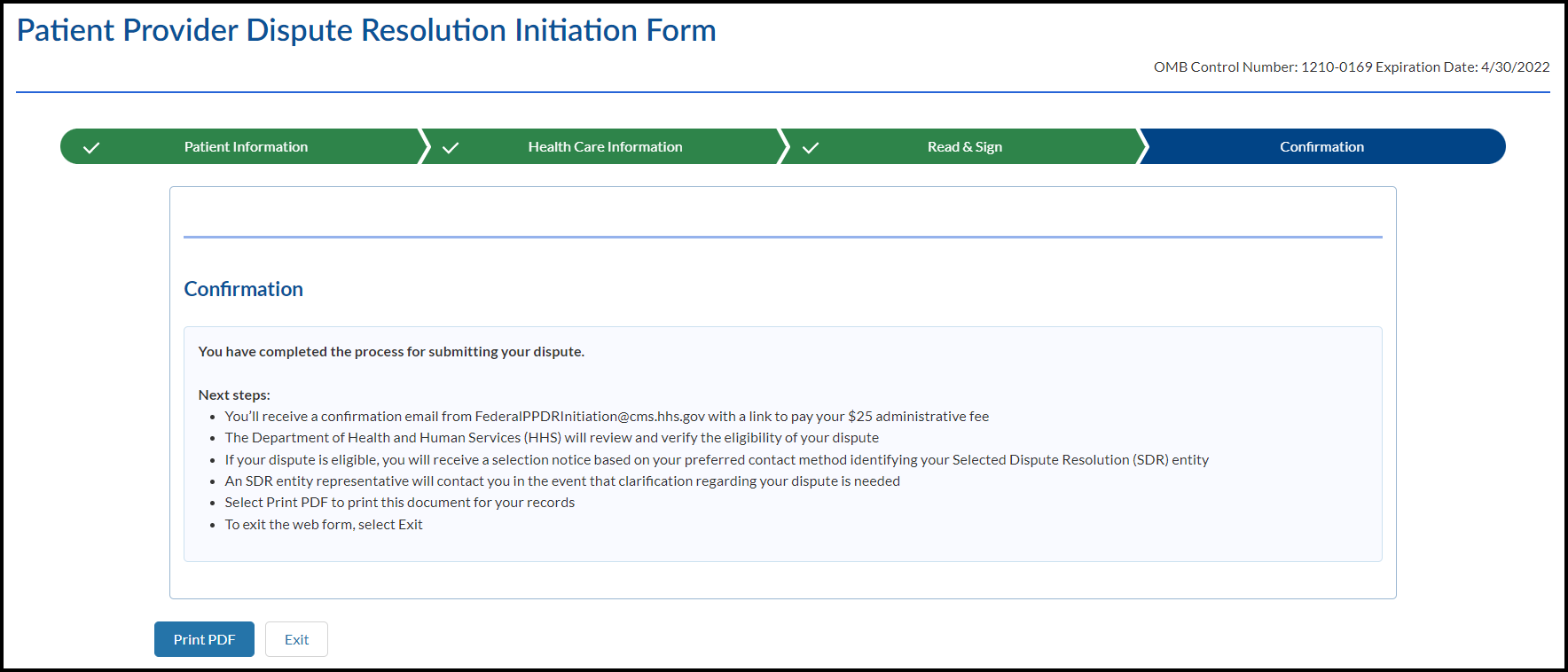
Confirmation
OMB Expiration Date
Progress Tracker: Patient Information | Provider Information | Read & Sign | Confirmation

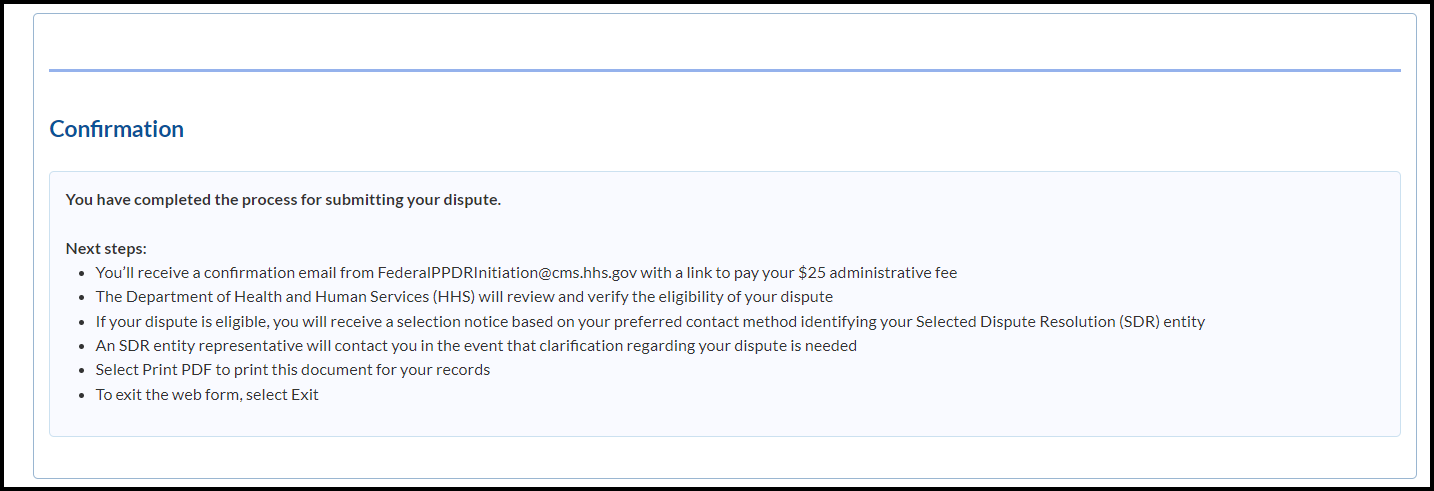
Confirmation
You have completed the process for submitting your dispute.
Next steps:
You’ll receive a confirmation email from FederalPPDRInitiation@cms.hhs.gov with a link to pay your $25 administrative fee.
The Selected Dispute Resolution (SDR) entity will review and verify the eligibility of your dispute.
If your dispute is eligible, you’ll receive a notice based on your preferred contact method identifying your SDR entity.
The SDR entity will contact you in the event that clarification regarding your dispute is needed.
Select Print PDF to print this document for your records.
To exit the web form, select Exit.
Print PDF (button)
![]()
Exit (button)
![]()
Exit Modal
Need to Leave?
All data entered up to this point will be lost. Are you sure you want to exit?
![]()
Cancel (button)
![]()
Exit (button)
![]()
e
Good Faith Estimate amount for one provider
or facility. Do not include the total amount on
Session Time Out
The window has been inactive for 15 minutes. Select Continue if you would like to remain on this page. If not, select Exit to return to the No Surprise’s Act page. If you take no action, you will be redirected in 21 seconds.
Exit (button)
![]()
Continue (button)
![]()
Paperwork Reduction Act Statement: According to the Paperwork Reduction Act of 1995, no persons are required to respond to a collection of information unless it displays a valid Office of Management and Budget (OMB) control number. The valid OMB control number for this information collection is 1210-0169. The time required to complete this information collection is estimated to average 1.3 hours per response, including the time to review instructions, search existing data resources, gather the data needed, and complete and review the information collection. If you have comments concerning the accuracy of the time estimate(s) or suggestions for improving this form, please write to: CMS, 7500 Security Boulevard, Attn: PRA Reports Clearance Officer, Mail Stop C4-26-05, Baltimore, Maryland 21244-1850.
PRIVACY ACT STATEMENT: CMS is authorized to collect the information on this form and any supporting documentation under section 2799B-7 of the Public Health Service Act, as added by section 112 of the No Surprises Act, title I of Division BB of the Consolidated Appropriations Act, 2021 (Pub. L. 116-260). We need the information on the form to process your request to initiate a payment dispute, verify the eligibility of your dispute for the PPDR process, and to determine whether any conflict of interest exists with the independent dispute resolution entity selected to decide your dispute. The information may also be used to: (1) support a decision on your dispute; (2) support the ongoing operation and oversight of the PPDR program; (3) evaluate selected IDR entity’s compliance with program rules. Providing the requested information is voluntary. But failing to provide it may delay or prevent processing of your dispute, or it could cause your dispute to be decided in favor of the provider or facility.
| File Type | application/vnd.openxmlformats-officedocument.wordprocessingml.document |
| Author | Charyszyn, Lisa |
| File Modified | 0000-00-00 |
| File Created | 2023-08-20 |
© 2026 OMB.report | Privacy Policy