6 Custom Web Survey with Consumer and Provider Paths
Federal COVID Response - Audience Feedback to Inform Ongoing Messaging and Strategies for "Combat COVID" (OD)
Attachment 6 - Custom Web Survey with Consumer and Provider Paths 061721
OMB: 0925-0769
Welcome Screen - ALL RESPONDENTS
dmConsent – ALL RESPONDENTS
Public reporting burden for this collection of information is estimated to average 15 minutes per response,
including the time for reviewing instructions, searching existing data sources, gathering and maintaining the
data needed, and completing and reviewing the collection of information. An Agency may not conduct or
sponsor, and a person is not required to respond to, a collection of information unless it displays a current
valid OMB control number. Send comments regarding this burden estimate or any other aspect of this
collection of information, including suggestions for reducing this burden, to NIH, Project clearance
Branch, 6705 Rockledge Drive, MSC 7974, Bethesda, MD 20892-7974, ATTN: PRA (XXXX-XXXX). Do
not return the completed form to this address.
[IF dmConsent/1 PROCEED TO dmCntry.]
[IF dmConsent/2 NO TERMINATE IMMEDIATELY.]
dmCntry – ALL RESPONDENTS
OMB Control Number: XXXX-XXXX Expiration
Date: XX/XX/XXXX
[IF dmCntry/244 UNITED STATES OF AMERICA PROCEED TO dmGen & dmAge.]
[IF hCntry DOES NOT EQUAL dmCntry TERMINATE IMMEDIATELY.]
dmGen & dmSex & dmAge – ALL RESPONDENTS
OMB Control Number: XXXX-XXXX Expiration
Date: XX/XX/XXXX
[IF dmAge/18+ PROCEED TO dmHispUS.]
[IF NOT 18+ TERMINATE IMMEDIATELY.]
dmHispUS – ALL US RESPONDENTS
OMB Control Number: XXXX-XXXX Expiration
Date: XX/XX/XXXX
[PROCEED TO dmRaceMUS.]
dmRaceMUS – ALL US RESPONDENTS
OMB Control Number: XXXX-XXXX Expiration
Date: XX/XX/XXXX
[PROCEED TO Q5.]
Q5 – ALL US RESPONDENTS
OMB Control Number: XXXX-XXXX Expiration
Date: XX/XX/XXXX
[IF Q5/1-20, PROCEED TO dmEmploy.]
[MUST RESIDE IN TARGET DMA 1-20. TERMINATE IF Q5/96 – None of the above.]
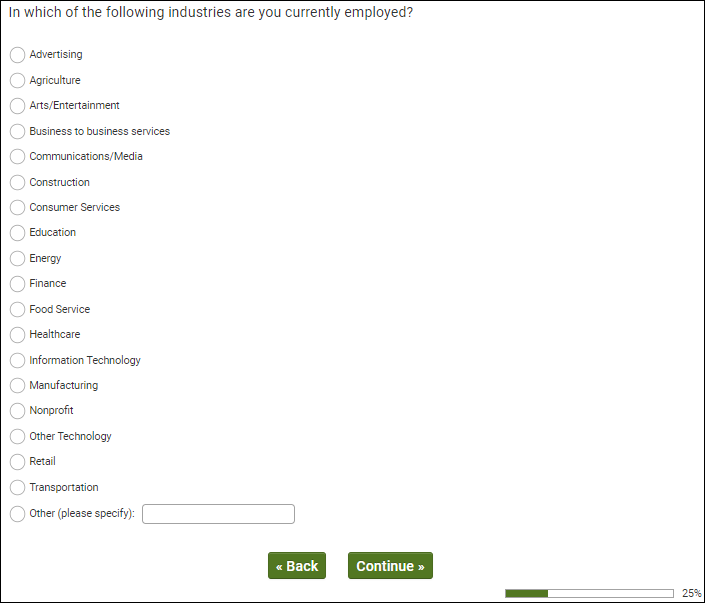
dmEmploy – ALL US RESPONDENTS
OMB Control Number: XXXX-XXXX
Expiration Date: XX/XX/XXXX
[IF dmEmploy/1,2,3,4 PROCEED TO Q10.]
[IF dmEmploy/5-10 PROCEED TO Q100]
Q10 - EMPLOYED (netEmploy/1)
OMB Control Number: XXXX-XXXX Expiration
Date: XX/XX/XXXX
[IF Q10/12 HEALTHCARE PROCEED TO Q20.]
[IF Q10/1-11,13-20 PROCEED TO Q100.]
Q20 - EMPLOYED IN HEALTHCARE (Q10/12) AND HCP SAMPLE SOURCE (Q1/2)
OMB Control Number: XXXX-XXXX Expiration
Date: XX/XX/XXXX
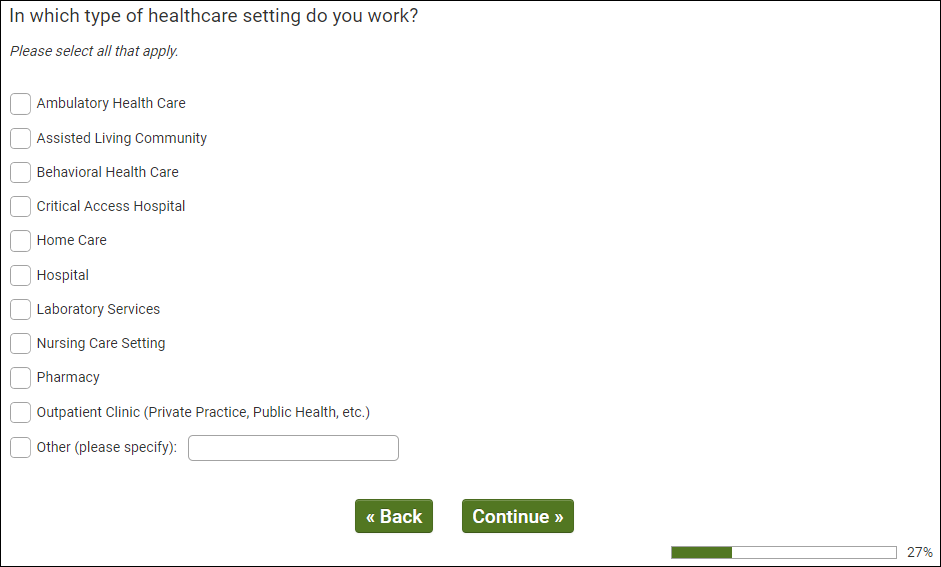
[IF HCP SAMPLE SOURCE Q1/2, MUST SELECT 1, 2, 4, 5, 6, 8, 9, 10 TO QUALIFY. PROCEED TO Q3. TERMINATE OTHERS]
Q30 - HCP SAMPLE (Q1/2) AND WORK IN QUALIFYING SETTING (Q20/1,2,4,5,6 OR 8)
OMB Control Number: XXXX-XXXX Expiration
Date: XX/XX/XXXX
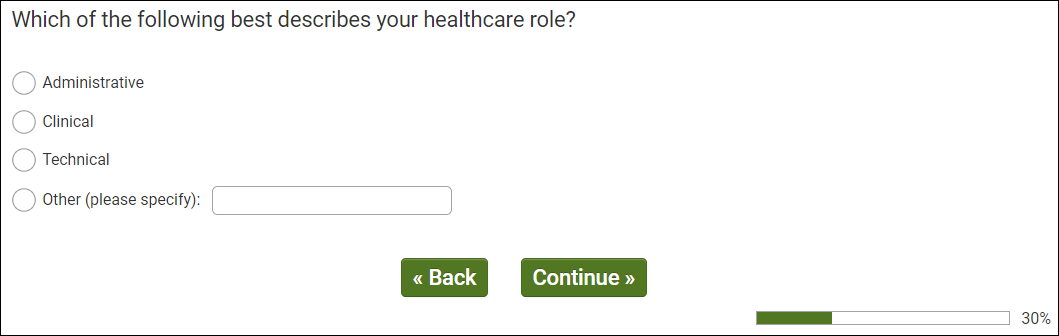
[IF HCP SAMPLE SOURCE (Q1/2) MUST SELECT 2/CLINICAL TO QUALIFY. PROCEED TO Q40. TERMINATE OTHERS]
Q40 - HCP SAMPLE (Q1/2) AND CLINICAL HEALTHCARE WORKER (Q30/2)
OMB Control Number: XXXX-XXXX Expiration
Date: XX/XX/XXXX
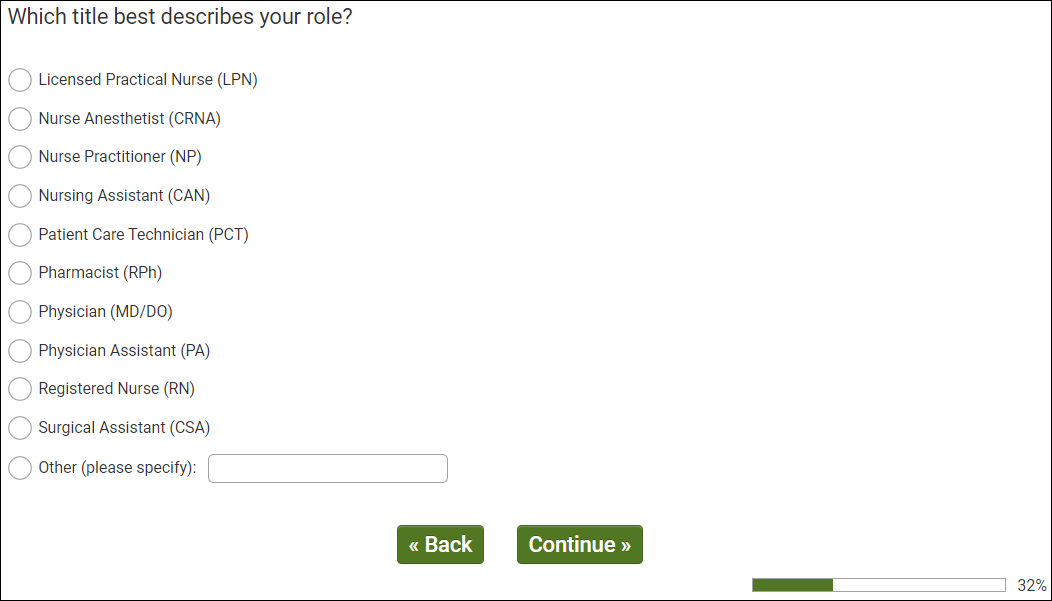
[IF HCP SAMPLE SOURCE (Q1/2) MUST SELECT 1, 2, 3, 6, 7, 8 OR 9 TO QUALIFY. PROCEED TO Q50. TERMINATE OTHERS]
Q50 - HCP SAMPLE (Q1/2) AND TARGET ROLE (Q40/3,6-7)
OMB Control Number: XXXX-XXXX Expiration
Date: XX/XX/XXXX
[IF HCP SAMPLE SOURCE (Q1/2) MUST SELECT 2/YES TO QUALIFY. PROCEED TO Q60 TERMINATE OTHERS]
Q60 - HCP SAMPLE (Q1/2) AND TREAT COVID PATIENTS (Q50/2)
OMB Control Number: XXXX-XXXX Expiration
Date: XX/XX/XXXX
QUALIFICATIONS
Consumers (Q1/1)
Live in target DMA (Q5/1-20)
Representative sample 18+
Healthcare Providers (Q1/2)
Live in target DMA (Q100/1-20)
Qualifying Setting (Q20/1, 2, 4, 5, 6, 8, 9, 10)
In Clinical Role (Q30/2)
Qualifying Specific Role (Q40/1,2,3,6,7,8,9)
Treat patients with COVID-19 (Q50/2)
Q100 – QUALIFIED CONSUMER RESPONDENTS
OMB Control Number: XXXX-XXXX Expiration
Date: XX/XX/XXXX
[IF QUALIFIED HCP (Q99/2) AND FAMILIAR (Q100 RATING 3-5) WITH TREATMENT TRIALS (Q100 CARD/2) PROCEED TO Q105.]
[IF QUALIFIED CONSUMER (Q99/1) AND FAMILIAR (Q100 RATING 3-5) WITH TREATMENT TRIALS (Q100 CARD/2) PROCEED TO Q108.]
Q105 - QUALIFIED HCP (Q99/2) AND FAMILIAR (Q100 RATING 3-5) WITH TREATMENT TRIALS (Q100 CARD/2)
OMB Control Number: XXXX-XXXX
Expiration Date: XX/XX/XXXX
[ALL QUALIFIED HCP PROCEED TO Q108.]
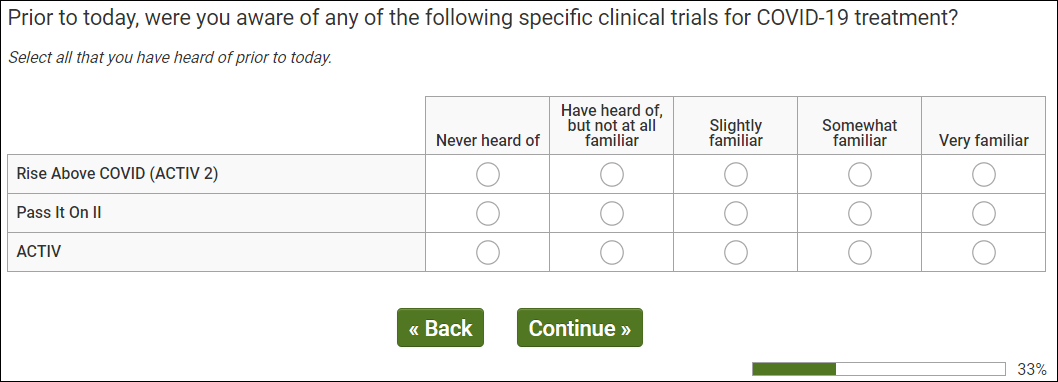
Q108 - AWARE OF CLINICAL TRIALS (Q100/2-5)
OMB Control Number: XXXX-XXXX Expiration
Date: XX/XX/XXXX
[ALL PROCEED TO Q110.]
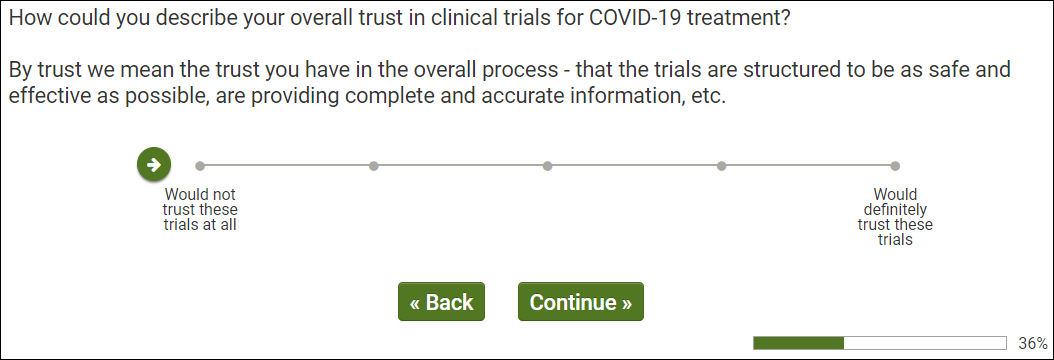
Q110 - QUALIFIED RESPONDENTS
OMB Control Number: XXXX-XXXX Expiration
Date: XX/XX/XXXX
[ALL PROCEED TO Q111.]
Q111 - QUALIFIED RESPONDENTS
OMB Control Number: XXXX-XXXX Expiration
Date: XX/XX/XXXX
[ALL PROCEED TO Q115.]
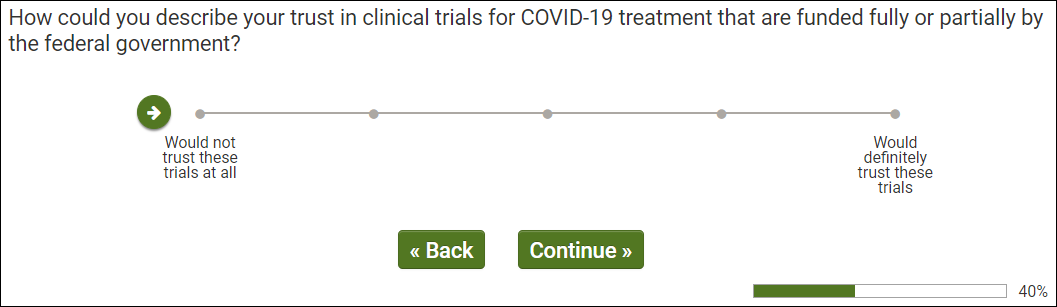
Q115 - QUALIFIED RESPONDENTS
OMB Control Number: XXXX-XXXX Expiration
Date: XX/XX/XXXX
[ALL PROCEED TO Q119.]
Q119 - QUALIFIED RESPONDENTS
OMB Control Number: XXXX-XXXX Expiration
Date: XX/XX/XXXX

[ALL PROCEED TO Q120.]
Q120 - QUALIFIED RESPONDENTS
OMB Control Number: XXXX-XXXX Expiration
Date: XX/XX/XXXX
[ALL PROCEED TO Q125.]
Q125 - QUALIFIED RESPONDENTS
OMB Control Number: XXXX-XXXX Expiration
Date: XX/XX/XXXX
[QUALIFIED CONSUMERS (Q99/1) PROCEED TO Q200.]
[QUALIFIED HCPS (Q99/2) PROCEED TO Q130.]
Q130 - QUALIFIED HCP (Q99/2)
OMB Control Number: XXXX-XXXX
Expiration Date: XX/XX/XXXX
[QUALIFIED HCPS (Q99/2) PROCEED TO Q135.]
Q135
OMB Control Number: XXXX-XXXX Expiration
Date: XX/XX/XXXX
[QUALIFIED HCPS (Q99/2) AND Q135/1-2 PROCEED TO Q136.]
[QUALIFIED HCPS (Q99/2) AND Q135/3-5 PROCEED TO Q137.]
Q136 - QUALIFIED HCP (Q99/2) AND Q135/1-2
OMB Control Number: XXXX-XXXX Expiration
Date: XX/XX/XXXX
[ALL PROCEED TO Q200.]
Q137 - QUALIFIED HCP (Q99/2) AND Q135/4-5
OMB Control Number: XXXX-XXXX Expiration
Date: XX/XX/XXXX
[ALL PROCEED TO Q200.]
Q200 - ALL RESPONDENTS
OMB Control Number: XXXX-XXXX Expiration
Date: XX/XX/XXXX

[ALL PROCEED TO Q201.]
Q201 - ALL RESPONDENTS
OMB Control Number: XXXX-XXXX Expiration
Date: XX/XX/XXXX
[IF Q201/1 PROCEED TO Q300.]
[IF Q201/2,3 PROCEED TO Q202.]
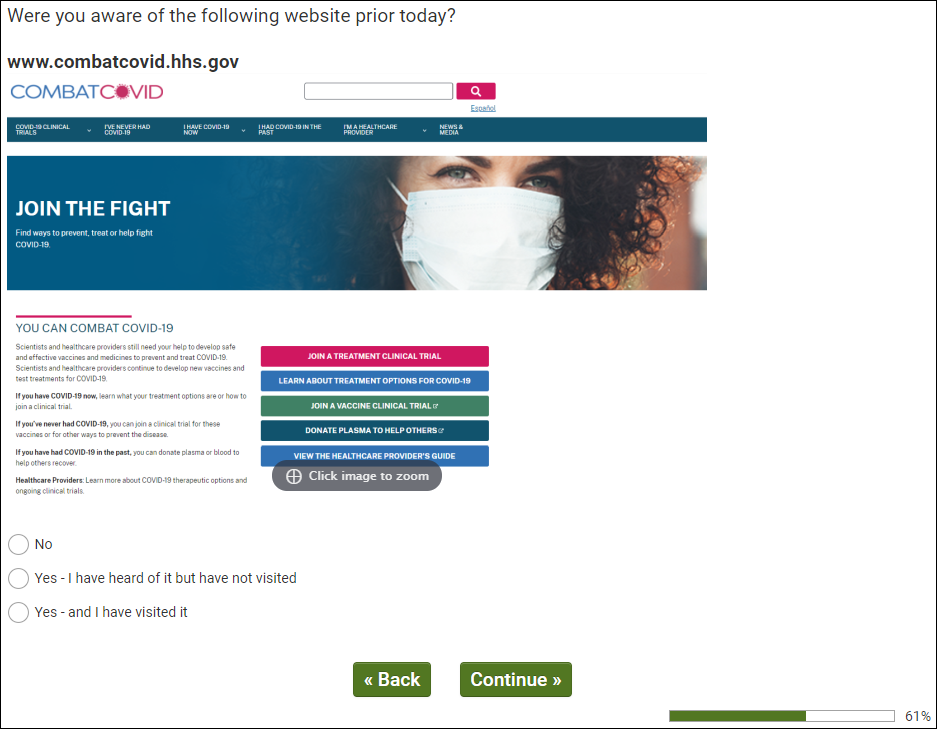
Q202 - AWARE OF WEBSITE (Q201/2,3)
OMB Control Number: XXXX-XXXX Expiration
Date: XX/XX/XXXX
[IF Q201/2 PROCEED TO Q215.]
[IF Q201/3 PROCEED TO Q205.]
Q205 - HAVE VISITED WEBSITE (Q201/3)
OMB Control Number: XXXX-XXXX Expiration
Date: XX/XX/XXXX
[PROCEED TO Q210.]
Q210 - HAVE VISITED SITE (Q201/3)
OMB Control Number: XXXX-XXXX Expiration
Date: XX/XX/XXXX
[PROCEED TO Q215.]
Q215- EXPOSED TO CAMPAIGN (Q200/2 OR Q201/2,3 OR Q203/2,3 OR Q204/2)
OMB Control Number: XXXX-XXXX Expiration
Date: XX/XX/XXXX
[PROCEED TO Q220.]
Q220 - EXPOSED TO CAMPAIGN (Q200/2 OR Q201/2,3 OR Q203/2,3 OR Q204/2)
OMB Control Number: XXXX-XXXX Expiration
Date: XX/XX/XXXX
[IF CONSUMER (Q99/1) PROCEED TO Q300.]
[IF HCP (Q99/2) PRCOEED TO Q405.]
Q300 – CONSUMER SAMPLE (Q99/1)
OMB Control Number: XXXX-XXXX Expiration
Date: XX/XX/XXXX
[ALL PROCEED TO Q305.]
Q305 – CONSUMER SAMPLE (Q99/1)
OMB Control Number: XXXX-XXXX Expiration
Date: XX/XX/XXXX
[ALL PROCEED TO Q310.]
Q310 – CONSUMER SAMPLE (Q99/1)
OMB Control Number: XXXX-XXXX Expiration
Date: XX/XX/XXXX
[ALL PROCEED TO Q315.]
Q315 – CONSUMER SAMPLE (Q99/1)
OMB Control Number: XXXX-XXXX Expiration
Date: XX/XX/XXXX
[ALL PROCEED TO Q320.]
Q320 – CONSUMER SAMPLE (Q99/1)
OMB Control Number: XXXX-XXXX Expiration
Date: XX/XX/XXXX
[ALL PRCOEED TO Q335.]
Q335 – CONSUMER SAMPLE (Q99/1)
OMB Control Number: XXXX-XXXX Expiration
Date: XX/XX/XXXX
[ALL PROCEED TO Q340.]
Q340 – CONSUMER SAMPLE (Q99/1)
OMB Control Number: XXXX-XXXX Expiration
Date: XX/XX/XXXX
[ALL PROCEED TO dmStateUS.]
Q405 – HCP SAMPLE (Q99/2)
OMB Control Number: XXXX-XXXX Expiration
Date: XX/XX/XXXX
[ALL PROCEED TO Q410.]
Q410 – HCP SAMPLE (Q99/2)
OMB Control Number: XXXX-XXXX
Expiration Date: XX/XX/XXXX
[ALL PROCEED TO Q415.]
Q415 – HCP SAMPLE (Q99/2)
OMB Control Number: XXXX-XXXX Expiration
Date: XX/XX/XXXX
[ALL PROCEED TO Q420.]
Q420 – HCP SAMPLE (Q99/2)
OMB Control Number: XXXX-XXXX Expiration
Date: XX/XX/XXXX
[ALL PROCEEDT Q420.]
Q425 - – HCP SAMPLE (Q99/2)
OMB Control Number: XXXX-XXXX Expiration
Date: XX/XX/XXXX
[ALL PROCEED TO dmStateUS.]
Real Answer Check – QUALITY CHECK
OMB Control Number: XXXX-XXXX Expiration
Date: XX/XX/XXXX
[REAL ANSWER CHECK INSERTED ACCORDING TO QUALITY CHECK LOGIC.]
ISQ Check – QUALITY CHECK
OMB Control Number: XXXX-XXXX Expiration
Date: XX/XX/XXXX
[ISQ CHECK INSERTED ACCORDING TO QUALITY CHECK LOGIC.]
dmStateUS – ALL RESPONDENTS
OMB Control Number: XXXX-XXXX Expiration
Date: XX/XX/XXXX
[PROCEED TO dmZipUS.]
dmZipUS – ALL RESPONDENTS
OMB Control Number: XXXX-XXXX Expiration
Date: XX/XX/XXXX
[PROCEED TO dmEduUS.]
dmEduUS – ALL RESPONDENTS
OMB Control Number: XXXX-XXXX Expiration
Date: XX/XX/XXXX
[PROCEED TO dmMarStat.]
dmMarStat – ALL RESPONDENTS
OMB Control Number: XXXX-XXXX Expiration
Date: XX/XX/XXXX
[PROCEED TO dmAdultHh.]
dmAdultHh – ALL RESPONDENTS
OMB Control Number: XXXX-XXXX Expiration
Date: XX/XX/XXXX
[PROCEED TO dmChildHh.]
dmChildHh – ALL RESPONDENTS
OMB Control Number: XXXX-XXXX Expiration
Date: XX/XX/XXXX
[PROCEED TO dmHhIncUS.]
dmHhIncUS – ALL RESPONDENTS
OMB Control Number: XXXX-XXXX Expiration
Date: XX/XX/XXXX
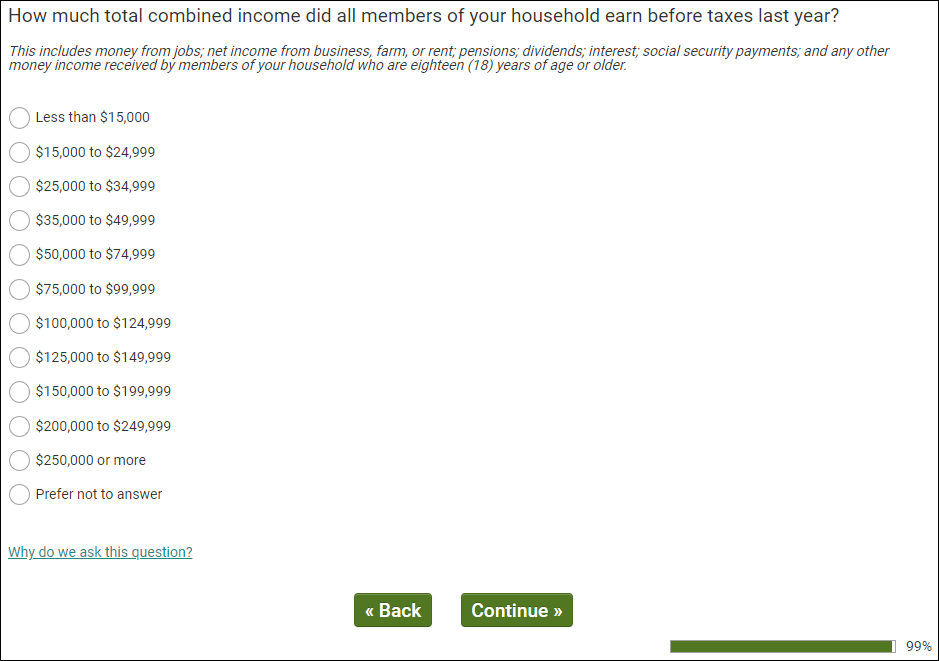
[PROCEED TO THANK YOU AND TERMINATE.]
| File Type | application/vnd.openxmlformats-officedocument.wordprocessingml.document |
| Author | Andrew Walton |
| File Modified | 0000-00-00 |
| File Created | 2021-07-05 |
© 2026 OMB.report | Privacy Policy