S+S Week Event Feedback Form Questions_OMBX
Safe + Sound Campaign
S+S Week Event Feedback Form Questions_OMB.DOCX
OMB: 1218-0269
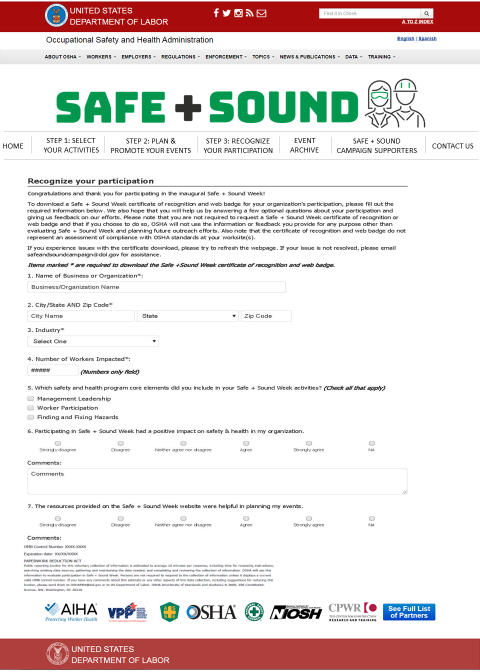
Safe + Sound Week Event Feedback Form
Name of Business or Organization* (Fill in Blank)
Industry* (Drop Down)
Email Address* (Fill in Blank)
Did you participate in the U.S.?* (Check box)
Yes
No
City/State AND Zip Code (Fill in Blank and Drop Down)
City/Country (Fill in Blank)
How did you find out about the event?* (Check all that apply) (Check box)
Communication from industry/trade association
Communication from safety and health professional organization
OSHA QuickTakes
OSHA Website
Safe + Sound Campaign Email List Serv
National/Local/Trade Press
Social Media
I don’t know/remember
Other (Fill in Blank)
Number of Workers Impacted* (Fill in Blank)
Which safety and health program core elements did you include in your Safe + Sound Week activities? (Check all that apply) (Check box)
Management Leadership
Worker Participation
Finding and Fixing Hazards
Participating in Safe + Sound Week had a positive impact on safety & health in my organization.
Strongly Disagree 1 2 3 4 5 NA Strongly Agree
(Check box)
Comments: (Fill in Blank)
The resources provided on the Safe + Sound Week website were helpful in planning my events.
Strongly Disagree 1 2 3 4 5 NA Strongly Agree
(Check box)
Comments: (Fill in Blank)
Tell us about your Safe + Sound Week experience. What did you do? (Fill in Blank)
What would improve your participation experience in the future? (Fill in Blank)
Would you like to share a quote about any successes, impacts, or outcomes related to your Safe + Sound Week activities? (Fill in Blank)
Are you interested in sharing more about your experience?
Yes
No
If yes, please provide contact information:
Contact Name (Fill in Blank)
Contact Phone Number (Fill in Blank)
OMB Control Number XXXX-XXXX
Expiration date: XX/XX/XXXX
PAPERWORK REDUCTION ACT
Public reporting burden for this voluntary collection of information is estimated to average 10 minutes per response, including time for reviewing instructions, searching existing data sources, gathering and maintaining the data needed, and completing and reviewing the collection of information. OSHA will use this information to evaluate participation in Safe + Sound Week. Persons are not required to respond to the collection of information unless it displays a current valid OMB control number. If you have any comments about this estimate or any other aspects of this data collection, including suggestions for reducing this burden, please send them to OSHAPRA@dol.gov or to US Department of Labor, OSHA Directorate of Standards and Guidance N-3609, 200 Constitution Avenue, NW, Washington, DC 20210.
Requirements for the form:
Question 1, 2, 3, 4, 7, 8 required for all responses.
Industry drop down should include the following:
Accommodation and Food Services
Agriculture, Forestry, Fishing and Hunting
Arts, Entertainment, and Recreation
Construction
Education Services
Financial Activities
Health Care and Social Assistance
Information
Manufacturing
Mining
Oil and Gas
Professional and Business Services
Public Administration
Real Estate Rental and Leasing
Trade (Wholesale/Retail)
Transportation and Warehousing
Utilities
Other: ___________________________________
Question 5 required if answer “yes” to Question 4.
Question 6 required if answer “no” to question 4.
In Question 5, the “State” field will be a drop-down menu with full state and territory names.
If Question 15 answered “yes”, contact name and contact phone number required.
| File Type | application/vnd.openxmlformats-officedocument.wordprocessingml.document |
| Author | Barclay, Pamela - OSHA |
| File Modified | 0000-00-00 |
| File Created | 2021-09-10 |
© 2026 OMB.report | Privacy Policy