Protocol
Attachment 3. Protocol.docx
National Firefighter Registry
Protocol
OMB: 0920-1348
DRAFT
National Firefighter Registry (NFR)
Protocol
Project Officer: Kenneth W. Fent, PhD, CIH, National Institute for Occupational Safety and Health;
Division of Field Studies and Engineering, Field Research Branch
Co-Investigators: Miriam Siegel, DrPH, MPH*, Alexander Mayer, MPH*, Andrea Wilkinson, MS, LAT, ATC*, Jill Raudabaugh, MPH*
* Division of Field Studies and Engineering, Field Research Branch
Version: 10/16/2020
DISCLAIMERS:
Mention of any company or product does not constitute endorsement by the National Institute for Occupational Safety and Health (NIOSH), Centers for Disease Control and Prevention (CDC).
This information is distributed solely for the purpose of pre dissemination peer review under applicable information quality guidelines. It has not been formally disseminated by NIOSH, CDC. It does not represent and should not be construed to represent any agency determination or policy.
TABLE OF CONTENTS:
SUMMARY
I. PERSONNEL AND RESOURCES
A. Key Personnel
II. PURPOSE
III. BACKGROUND
A. Exposure studies
B. Epidemiological studies
C. Knowledge Gaps
D. Firefighter Cancer Registry Act of 2018
E. Rationale
IV. PROPOSED APPROACH
A. Participant Population
B. Stakeholder Participation and Advisory Committee
C. Objectives
V. DATA MANAGEMENT AND ANALYSIS
A. Data Security
B. Data Analysis
C. Potential Limitations and Considerations
VI. HUMAN SUBJECTS PROTECTIONS
A. Surveillance and Research Activities
B. Informed Consent
C. The Reasonable Person Standard
D. Confidentiality
VII. STUDY RISKS AND BENEFITS
A. Assessment of Potential Benefits
B. Assessment of Potential Risks
C. Description of Measures Taken to Minimize Potential Risks
D. Vulnerable populations
E. Risk versus Benefit Evaluation
VIII. FUNDING
REFERENCES
APPENDICES
Appendix A – NFR Design Flowcharts
Appendix B – NFR Promotional Campaign
Appendix C – List of Stakeholders
Appendix D – Informed Consent Document
Appendix E – User Profile Questions
Appendix F – Enrollment Questionnaire
Appendix G – Assurance of Confidentiality
ACRONYMS
AoC Assurance of Confidentiality
BLS Bureau of Labor Statistics
BSC Board of Scientific Counselors
CDC Centers for Disease Control and Prevention
DNA Deoxyribonucleic acid
DUA Data use agreement
FRs Flame retardants
HCN Hydrogen cyanide
IABPFF International Association of Black Professional Fire Fighters
IAFC International Association of Fire Chiefs
IAFF International Association of Fire Fighters
IAWF International Association of Wildland Fire
IARC International Agency for Research on Cancer
IIF Information in Identifiable Form
IRB Institutional Review Board
LTAS Life Table Analysis System
MFA Multi-factored authentication
NAACCR North American Association of Central Cancer Registries
NDI National Death Index
NFORS National Fire Operations Reporting System
NFPA National Fire Protection Association
NFR National Firefighter Registry
NIOSH National Institute for Occupational Safety and Health
NIST National Institute of Standards and Technology
NVFC National Volunteer Fire Council
OMB Office of Management and Budget
PAH Polycyclic aromatic hydrocarbons
PCB Polychlorinated biphenyls
PPE Personal protective equipment
RFI Request for information
SEER Surveillance, Epidemiology, and End Results
SIRs Standardized Incidence Ratios
SMR Standardized mortality ratio
STEL Short term exposure limits
TDE Transparent Data Encryption
UUID Universally unique identifier
VOC Volatile organic compounds
VPR-CLS Virtual Pooled Registry Cancer Linkage System
USFA United States Fire Administration
SUMMARY
Cancer risk in the U.S. fire service is a topic of growing concern, and firefighters’ occupational exposure to hazardous contaminants is thought to play an important role in their excess cancer risk. Dozens of chemicals classified by the International Agency for Research on Cancer (IARC) as known or probable carcinogens (IARC, 2010; IARC, 2020) have been identified on the fireground. Polycyclic aromatic hydrocarbons (PAH) metabolites, some of which are classified as known or probable carcinogens by IARC, have been identified in firefighters’ urine after fire responses (Fent et al., 2014).
Epidemiologic evidence from recent studies suggest firefighters have an increased risk for cancer. Specifically, a meta-analysis conducted by LeMasters et al. in 2006 found firefighters have an increased risk for several types of cancer (LeMasters et al., 2006). In 2010, IARC classified firefighters’ occupational exposure to be possibly carcinogenic (Group 2B) (IARC, 2010). In 2014, Daniels et al. conducted a study with nearly 30,000 firefighters and found 9% more cancer diagnoses than expected based on rates in the general population (Daniels et al., 2014). An additional analysis found an exposure-response relationship between fire-runs and leukemia, and fire hours and lung cancer (Daniels et al., 2015).
More information is needed to assess the cancer risk for minority and female firefighters. Minority firefighters make up roughly 20% of the career workforce (BLS, 2019), and roughly 8% of all firefighters are women (NFPA, 2018). While there is evidence to suggest that minority and female firefighters have an increased risk for some cancers (Daniels et al., 2014; Tsai et al., 2015; Lee et al., 2020), most studies have lacked sufficient power to examine cancer risk for these populations.
Few studies have examined the potential cancer risk for volunteer firefighters, who comprise a majority of the U.S. fire service, as well as subspecialty groups like wildland firefighters, fire investigators, and instructors. Similarly, while nearly half of U.S. fire departments serve rural populations (NFPA, 2018), cancer risk has yet to be evaluated for most firefighters serving rural areas. More information on lifestyle characteristics is needed to better understand the relationship between firefighting and cancer. More comprehensive information on exposure characteristics like fire incidents (e.g., number of fire runs, time spent on fireground) and control measures (e.g. consistent use of respiratory protection, decontamination measures, etc.) and how they relate to cancer would allow for better informed public health decisions relating to efforts to reduce cancer incidence in the U.S. fire service.
In order to accurately monitor trends in cancer incidence and evaluate control measures among the U.S. fire service, Congress passed the Firefighter Cancer Registry Act of 2018. Under this legislation, the U.S. Centers for Disease Control and Prevention’s (CDC) National Institute for Occupational Safety and Health (NIOSH) was directed to create a registry of U.S. firefighters for the purpose of monitoring cancer incidence and risk factors among the current U.S. fire service. Funding of the project was authorized through this legislation for five years as of fiscal year 2019.
The main goal of the National Firefighter Registry (NFR), according to the Firefighter Cancer Registry Act of 2018, is “to develop and maintain…a voluntary registry of firefighters to collect relevant health and occupational information of such firefighters for purposes of determining cancer incidence.” Results from the NFR will provide information for decision makers within the fire service and medical or public health community to devise and implement policies and procedures to lessen cancer risk and/or improve early detection of cancer among firefighters. This goal aligns with public health surveillance. Below, we have identified the primary surveillance activities necessary to achieve this goal:
Collect self-reported information from firefighters on employment/workplace characteristics, exposure, demographics, lifestyle factors, co-morbidities, and other confounders related to cancer.
Obtain records from fire departments/agencies to track trends and patterns of exposure as it relates to cancer in firefighters.
Monitor cancer in firefighters by linking with health information databases (e.g., population-based cancer registries and the National Death Index (NDI)) to assess cancer incidence and mortality.
I. PERSONNEL AND RESOURCES
A. Key Personnel
Key personnel include Kenneth Fent, PhD (Research Industrial Hygienist/Team Lead), Miriam Siegel, DrPH (Lead Epidemiologist), Alex Mayer, MPH (Health Scientist), Jill Raudabaugh, MPH (Data Scientist), Andrea Wilkinson, MS (Health Scientist), William Wepsala, MPA (Health Communication Specialist), Breanna Newton, MPH (Data Scientist), I-Chen Chen, PhD (Statistician), Stephen Bertke, PhD (Statistician).
The investigator leading the project has extensive research experience working on exposure science as it relates to firefighters. Dr. Kenneth Fent has led and published on several projects assessing firefighters’ exposures. Dr. Miriam Siegel is serving as the lead epidemiologist on the project and has experience working with firefighters. Alex Mayer and Andrea Wilkinson will serve as health scientists on the team, and both individuals have published on several projects assessing exposures among firefighters. Jill Raudabaugh is a data scientist and team leader for the Data Science Team in the Field Research Branch. Jill Raudabaugh will lead the data security aspect of the project. Breanna Newton will assist with data management. Drs. Stephen Bertke and I-Chen Chen are experienced statisticians who will provide data analysis support. Will Wepsala will lead the communications aspects of the project, including the development of recruiting and promotional materials.
II. PURPOSE
The purpose of the NFR is to evaluate and monitor cancer rates and risk factors in the current U.S. fire service. With voluntary participation from firefighters, the NFR will obtain information about work and exposure history, demographics, co-morbidities, and lifestyle factors. This information will be linked with records from population-based, or state, cancer registries to monitor cancer diagnoses and improve our knowledge about cancer risks for firefighters, especially those linked to workplace exposures. Special emphasis will be given to recruit a large sample that is diverse by geography, sex, race/ethnicity, career status, and firefighter specialization.
III. BACKGROUND
A. Exposure studies
Structural firefighters are occupationally exposed to a number of hazardous chemicals during emergency fire responses. Chemicals found on the fireground include PAHs like benzo[a]pyrene and dibenz[a,h]anthracene, volatile organic compounds (VOCs) like benzene, polychlorinated biphenyls (PCBs), dioxins, flame retardants (FRs), formaldehyde, and hydrogen cyanide (HCN), and respirable particulates (Bolstad-Johnson et al., 2000; Fent et al., 2018; Fent et al., 2019a; Jankovic et al., 1991). Over a dozen of these chemicals are listed by IARC as Group 1, known carcinogens to humans, including benzene, benzo[a]pyrene, formaldehyde, and PCBs, while other chemicals are listed as Group 2A, probably carcinogenic to humans, such as dibenz[a,h]anthracene (IARC, 2010; IARC, 2020).
PAHs are produced during incomplete combustion and have been associated with certain types of cancer (Dreij, 2017). Several studies (Fent et al., 2017; Fent et al., 2014; Kirk and Logan, 2015; Stec et al., 2018) have found structural firefighters are occupationally exposed to PAHs, including a study by Fent et al. in 2014 where PAH metabolites were identified in firefighters’ urine post firefighting. In addition, studies have found phthalates, PAHs, and FRs on firefighters’ personal protective equipment (PPE) after fire responses (Alexander and Baxter, 2016; Easter et al., 2016; Fent et al., 2014). These contaminants could also be transferred to skin and dermally absorbed, inhaled, or inadvertently ingested.
By comparison, fewer studies have evaluated exposures in subspecialty groups of firefighters. Of note, a study by Fent et al. examined firefighter instructors supervising three trainings per day and found PAH metabolite concentrations increased after each training (Fent et al., 2019b). Some studies have examined wildland firefighters’ exposures, including a study reporting carbon monoxide air exposure that exceeded short term exposure limits (STEL) (Adetona et al., 2013). Another study investigated prescribed burns and identified increased PAH metabolite concentrations in urine collected from wildland firefighters post-fire (Adetona et al., 2017). Workloads, work schedules, and environments also vary substantially by firefighting subspecialty, impacting the frequency and duration of exposures. Indeed, firefighters’ occupational exposures to contaminants are thought to play an important role in their cancer risk.
B. Epidemiological studies
Early epidemiological studies on the association between firefighting and cancer mortality in the U.S. often evaluated only a single municipal fire department or a collection of a few regionally-linked departments (Baris et al., 2001; Beaumont et al., 1991; Demers et al., 1992; Lewis et al., 1982; Musk et al., 1978; Vena et al., 1987). Findings from these individual studies were somewhat inconsistent, with moderately weak measures of association and some variability in the cancers found to be elevated. These studies were limited by relatively small sample sizes, short periods of follow-up, and geographic variation across samples.
Several studies have been published in recent years that have evaluated cancer among larger, more diverse samples of firefighters. In the U.S., Daniels et al. (2014) conducted a retrospective cohort study of nearly 30,000 firefighters employed in Philadelphia, Chicago, and San Francisco between 1950–2009 and found 14% more cancer deaths and 9% more cancer diagnoses than expected based on rates in the general population. These increases were primarily due to digestive (esophagus, intestine, colon/rectum), respiratory (lung, mesothelioma), urinary (kidney, bladder), and oral (buccal and pharynx) cancers. There was some evidence for elevated prostate cancer and leukemia among non-white firefighters and breast and bladder cancer among female firefighters, but sample sizes were small, or estimates were not statistically significant for these groups. A mortality update of the cohort published in 2020 found additional evidence for elevated mortality due to non-Hodgkin’s lymphoma overall (Pinkerton et al., 2020). A recent large case-control study of approximately 4,000 California firefighters found elevated odds of melanoma, multiple myeloma, leukemia, and cancers of the esophagus, prostate, brain, and kidney overall (Tsai et al., 2015); and non-Hodgkin’s lymphoma and cancers of the tongue, testes, and bladder were found to be associated with firefighting among small samples of non-white firefighters. A recent mortality study of Indiana firefighters found excess deaths due to malignant cancers, including oral, pancreatic, kidney, connective tissue, and nervous system cancers (Muegge et al., 2018). In Florida, a study published in 2020 found firefighting to be associated with melanoma and cancers of the prostate, testes, thyroid, and colon in men; and cancers of the thyroid and brain in women (Lee et al., 2020). Large international studies generally support the finding from U.S. studies that firefighters have elevated rates of cancer, with some variation by cancer site (Ahn et al., 2012; Amadeo et al, 2015; Glass et al., 2016b; Glass et al., 2017; Glass et al., 2019; Harris et al., 2018; Petersen et al., 2018a; b; Pukkala et al., 2014).
Recent meta-analyses have pooled findings from individual epidemiological studies on cancer mortality and incidence in U.S. and international firefighting populations (LeMasters et al., 2006; Guidotti et al., 2007; IARC, 2010; Sritharan et al., 2017; Jalilian et al., 2019; Soteriades, et al., 2019; Casjens et al., 2020). These meta-analyses identified cancers that appeared to be elevated based on a weight of the evidence, including testicular (Lemasters et al., 2005; Guidotti et al., 2007; IARC, 2010; Jalilian et al., 2019; Soteriades, et al., 2019; Casjens et al., 2020), prostate (Lemasters et al., 2005; Guidotti et al., 2007; IARC, 2010; Jalilian et al., 2019; Sritharan et al., 2017; Soteriades, et al., 2019; Casjens et al., 2020), bladder (Guidotti et al., 2007; Jalilian et al., 2019; Soteriades, et al., 2019; Casjens et al., 2020), colorectal (Jalilian et al., 2019; Soteriades, et al., 2019; Casjens et al., 2020), lymphohematopoietic (e.g., non-Hodgkin lymphoma, multiple myeloma) (Lemasters et al., 2005; Guidotti et al., 2007; IARC, 2010; Jalilian et al., 2019; Sritharan et al., 2017; Soteriades, et al., 2019), central nervous system (Soteriades, et al., 2019), thyroid (Jalilian et al., 2019), pancreatic (Casjens et al., 2020), and pleural cancers (Jalilian et al., 2019; Casjens et al., 2020), and melanoma (Jalilian et al., 2019; Soteriades, et al., 2019; Casjens et al., 2020). As a result of the meta-analysis conducted by IARC, the agency classified firefighting to be possibly carcinogenic to humans (Group 2B) (IARC, 2010). However, in March of 2019, the IARC Advisory Group recommended firefighting as a high priority for reevaluation based on new human cancer and mechanistic evidence (IARC, 2019).
Few studies have evaluated potential exposure-response relationships. Of these studies, some surrogates of exposure have included duration of employment/firefighting (Aronson et al., 1994; Baris et al., 2001; Bates et al., 2001; Beaumont et al., 1991; Demers et al., 1994; Guidotti et al., 1993; Heyer et al., 1990; Tornling et al., 1994; Vena et al., 1987), number of fire runs (Baris et al., 2001; Daniels et al., 2015; Tornling et al., 1994), and number of hours spent at fires (Daniels et al., 2015). Cancers that were found to be significantly elevated with increasing exposure in these studies included testicular (Bates et al., 2001), prostate (Demers et al., 1994), and lung cancers, and leukemia (Daniels et al., 2015).
The research on cancer for subspecialty groups of firefighters is limited, but a recent study of fire instructors (paid and volunteer) in Australia found an exposure-response relationship between training exposures (based on job activities) and cancer incidence (Glass et al., 2016a). To examine cancer risk for wildland firefighters, Navarro et al. (2019) conducted a risk assessment using an exposure-response relationship for risk of lung cancer mortality and measured particulate matter exposure from smoke at wildfires. This study estimated that wildland firefighters were at an increased risk of lung cancer mortality (8 to 43 percent) across different exposure scenarios and career durations.
In addition to epidemiological studies, mechanistic studies have used biomarkers to investigate exposures’ effects on biological changes that could be related to cancer development. These studies provide evidence of DNA damage, oxidative stress, and epigenetic changes related to firefighter exposures (Abreu et al., 2017; Adetona et al., 2017; Andersen et al., 2017; Hoppe-Jones et al., 2018; Jeong et al., 2018; Keir et al., 2017; Oliveira et al., 2018; Zhou et al. 2019).
C. Knowledge Gaps
Exposure research supports that firefighters are exposed to hundreds of chemicals at fires, many of which are known or probable carcinogens (IARC, 2010; IARC, 2020). Epidemiologic evidence suggests that firefighters are at an increased risk for cancer. There is some variation in the literature on the risk of cancer by cancer site, which could be due to chance findings or differences in exposures, workplace practices, and PPE use by geographic region; firefighter characteristics; and time (Fritschi et al., 2014; Casjens et al., 2020). Many details about the risk of cancer among the fire service are still poorly understood.
While there is some possible evidence to suggest that non-white or minority and female firefighters have an increased risk of specific cancers (Daniels et al., 2014; Tsai et al., 2015), analyses of demographic subgroups have been underpowered because study samples have consisted of predominantly white male populations. Roughly 20% of career firefighters are non-white or minorities, approximately 8% of all firefighters are women, and select subspecialty groups of firefighters may be even more diverse (BLS, 2019; NFPA, 2018). Therefore, findings are not necessarily generalizable to the entire workforce unless samples sufficiently represent these demographics. Furthermore, in the general population, cancer rates vary by demographic characteristics, including sex and race/ethnicity (Howlader et al., 2019), as do cancer risk factors (e.g., social determinants of health) (Ellis et al., 2018), and biological mechanisms for metabolism of substances and/or the development of cancer (Wiencke et al., 2004; Zahm et al., 1995). But little is known about how cancer risk differs across varying demographic groups of firefighters. Additionally, larger samples of female firefighters are needed to estimate specific cancer incidence, such as cancers of the breast and female reproductive organs.
Studies support that workplace activities, practices, and exposures can vary based on firefighting specialization (Broyles, 2013; Fritschi et al., 2014; Glass et al., 2016a), but most epidemiologic studies have evaluated cancer risk only among groups of career structural firefighters. More information is needed on cancer rates and risk factors for volunteers, wildland and airport rescue firefighters, fire investigators, instructors, and others. Similarly, while nearly half of U.S. fire departments serve rural populations of less than 2,500 people (NFPA, 2018), cancer risk has yet to be evaluated for firefighters serving rural areas.
More accurate information on exposure characteristics like fire incidents (e.g., number of fire runs, time spent on fireground) and control measures (e.g. consistent use of respiratory protection, hood exchange programs, etc.) and how they relate to cancer incidence in the U.S. fire service is needed. It is also important to consider personal and lifestyle risk factors for cancer, such as tobacco and alcohol use, sleep deprivation, diet, and physical activity, in order to better understand how they may affect the relationship between firefighting and cancer; especially because the effects of these personal risk factors on cancer risk appear to be larger than the individual effects of firefighting and firefighting exposures that have been observed (Daniels et al., 2015; IARC, 2012; Schottenfeld et al., 2006). Likewise, information on the use of PPE and workplace practices is necessary to obtain a more comprehensive understanding of cancer risk associated with firefighting as an occupation. Lastly, it is important to collect health information from firefighters because comorbidities (e.g., diabetes) and associated health behaviors may increase or mediate the risk of certain types of cancer.
Some population-based (i.e., state) cancer registries collect occupational information, but it is often vague and incomplete (Freeman, et al. 2017) because patient information related to work history is often not obtained in the healthcare setting. Among firefighters specifically, one study found that roughly half of career firefighters in Florida with a cancer diagnosis were missing an occupation classification in the cancer registry, and only 17% were classified as a firefighter in the cancer registry (McClure et al., 2019). This estimate would likely be much smaller for former or retired firefighters, or volunteers working a non-firefighting job, at the time of cancer diagnosis, since the extent of occupational information ascertained may relate only to current job. Therefore, there is not enough accurate information available from state cancer registries alone to produce comprehensive estimates of cancer burden and risk factors among the fire service nationally.
D. Firefighter Cancer Registry Act of 2018
The President of the United States signed the Firefighter Cancer Registry Act of 2018 in July 2018, authorizing the Secretary of Health and Human Services to develop a voluntary registry to collect data on cancer incidence among firefighters (Congress, 2018). This law charged NIOSH—through CDC’s Director—to create the National Firefighter Registry.
Specifically, NIOSH is required to “improve data collection and data coordination activities related to the nationwide monitoring of the incidence of cancer among firefighters” and “to collect, consolidate, and maintain, epidemiological information and analyses related to cancer incidence and trends among volunteer, paid-on-call and career firefighters”. The law also requires NIOSH to “generate a statistically reliable representation of minority, female, and volunteer firefighters” and requires NIOSH “consult with non-Federal experts on the Firefighter Registry”. Lastly, NIOSH is responsible for developing a “reliable and standardized method for estimating the number of fire incidents attended by a firefighter as well as the type of fire incident”.
E. Rationale
There are over 1.1 million firefighters currently serving in the United States (NFPA, 2018). Though roughly 20% of the firefighting workforce are racial/ethnic minorities, 8% are women, and 67% are volunteers (BLS, 2019; NFPA, 2018), these subgroups have been understudied in relation to cancer risk. In order to obtain a diverse sample of U.S. firefighters to accurately assess cancer incidence, NIOSH investigators will seek to enroll firefighters at fire departments with higher numbers of female and minority firefighters from all regions of the country. In addition, NIOSH will encourage participation from subspecialty groups of firefighters including but not limited to wildland firefighters, fire investigators, and fire instructors. Overall, the NFR will seek to register approximately 200,000 firefighters in an effort to capture a more generalizable sample of the workforce.
This would be the largest database of firefighters ever assembled for health purposes and would allow NIOSH investigators to monitor cancer incidence in the U.S. fire service. Specifically, this sample size may enable investigators to monitor firefighters for rare types of cancer not previously identified in this workforce. Additionally, previous studies like Daniels et al. (2015) examined firefighters’ cancer risk based on exposures to burning of older structures (1950-2009). Through the NFR, NIOSH investigators can examine cancer risk among firefighters who may have different exposures, such as those experienced from the burning of synthetic materials present in newer structures. By aiming for a diverse sample with representation from subgroups specified in the Act (i.e., women, minorities, and volunteers), investigators can be more confident that results will better inform public health action.
IV. PROPOSED APPROACH
A. Participant Population
The NFR will be a surveillance system of adult (> 18 years of age) U.S. firefighters designed to evaluate cancer rates and occupational risk factors in the current U.S. firefighting workforce. The goal is to achieve a total NFR sample (i.e., General NFR Sample) of close to 200,000 participants 5 years after beginning enrollment that is diverse demographically (gender, race, etc.), geographically, and by firefighting specialization (investigation, wildland firefighting, etc.) and type of firefighter (career, volunteer, paid-on call, etc.). There will be no exclusion or inclusion criteria based on cancer or health status. There will be two components of the comprehensive General NFR Sample: a subsample comprised of a Targeted Cohort for assessing cancer incidence; and a more-inclusive Open Cohort for describing cancer risk factors and other cross-sectional analyses (Appendix A). Specific inclusion criteria and sampling/recruitment strategies for each NFR component are outlined below.
1. Targeted Cohort
The Targeted Cohort will provide the population at risk required for assessing cancer incidence by targeting a sample of firefighters from career and volunteer fire departments that is diverse by geographic, demographic, and occupational characteristics, and following their vital and cancer status. The Targeted Cohort will be a prospective dynamic cohort (continuous enrollment). Firefighters in the Targeted Cohort will be recruited from two sampling frames: selected departments and state firefighter certification databases. Eligible participants will be all current firefighters from selected departments or states with rosters of firefighters. These eligible fire personnel will be invited by NIOSH to participate in the NFR. Additionally, departments with high participation from the Open Cohort (e.g., >70% of the department’s fire personnel) might also be added to the Targeted Cohort, as described below in the Open Cohort section. If individuals decline to participate or do not respond to our request, their information will not be used for NFR analyses.
The Targeted Cohort will be important for several reasons, including: 1) this approach will limit selection/participation bias with specific eligibility criteria and a sampling design; 2) quality exposure information can be obtained from department records; 3) the design provides a defined population at risk for estimating cancer incidence rates; and, 4) department workforce information allows for the assessment of NFR response characteristics and potential biases of the Open Cohort.
a. Targeted Cohort: Selected Fire Departments
Targeted career and volunteer departments will be selected in two sampling phases, as outlined below in Fire Department Sampling Strategy. Phase 1 will be recruitment from departments with high numbers of female, minority, and volunteer firefighters, to ensure adequate sample size for analysis. Fire departments with large numbers of female and minority firefighters will generally be those with a large overall workforce, thus these departments will also contribute large numbers of firefighters to the Targeted Cohort overall. Phase 2 will utilize a stratified random design to select a geographically diverse sample of career and volunteer departments from across the country.
The departments selected for targeted recruitment will be contacted to identify a primary point of contact for all NFR-related matters. The NIOSH team will then obtain rosters of the current firefighting workforce (i.e., employed at the time of NIOSH’s roster solicitation) for these departments. These rosters will provide the total number of current fire personnel and firefighters’ contact information (e.g., name and email address) to allow NIOSH to send individual invitations for firefighters to voluntarily enroll. NIOSH investigators will also request support in individual firefighter recruitment from department and state leadership and from the local union/memberships (if applicable). Fire departments may be unable or decline to participate, in which case, NIOSH will reach out to other departments with similar characteristics by using the same means of selection or from the same sampling stratum. For those departments that agree to participate, NIOSH investigators will provide informational and promotional materials (directly and through the department/union) to encourage all eligible firefighters to enroll through the NFR web portal. See Appendix B for an example of recruiting materials. Additionally, NIOSH will request incident records from departments dating back to at least January 1, 2010, and preferably older, as discussed under Objective 2, for ascertaining incident-specific exposure information. Updated rosters and incident records will be requested on a recurring basis (e.g., every two years) to recruit firefighters new to the department and to update incident information. Departments that are unwilling or unable to provide incident records might still be included in the Targeted Cohort, however, NIOSH may recruit additional or alternate departments with similar characteristics (i.e., from the same phase/strata) in order to obtain adequate rosters with incident records for the Targeted Cohort. All new firefighters identified in rosters obtained by NIOSH periodically (e.g., every two or three years) will be actively invited to participate in NFR enrollment (firefighters can also enroll themselves through the web portal before then) until a sufficient number of firefighters are enrolled to provide statistical power to detect meaningful differences in risk estimates according to the sample size calculation (see Sample Size Calculation (Targeted Cohort)).
i. Fire Department Sampling Strategy
Phase 1: Focused Enrollment of Women, Minorities, and Volunteers:
Phase 1 will involve focused enrollment of female, minority, and volunteer firefighters (Appendix A). Departments with high numbers of female and minority firefighters, defined as the approximate number currently active with the department, will be identified by recent estimates from surveys of fire departments (e.g., NFPA census estimates) and/or conversations with relevant stakeholder groups. At least 10 departments with large numbers of female firefighters and 20 departments with large numbers of minority firefighters will be recruited; otherwise, departments will be recruited until sufficient samples of female and minority firefighters have been obtained for the Targeted Cohort (as indicated by Sample Size Calculations (Targeted Cohort)).
Additionally, NIOSH will consult estimates from surveys of fire departments (e.g., NFPA census estimates) and stakeholder groups to identify a list of large volunteer/mostly volunteer departments or career departments with a large volunteer workforce from across the country (i.e., with representation in all four U.S. regions). NIOSH will randomly select approximately six of these departments from each of the four regions defined by the U.S. Census Bureau (Northeast, Midwest, South, West) to ensure geographic variability. Otherwise, volunteer departments will be recruited from the four regions until a sample of volunteer firefighters has been obtained that is adequate for analysis (as indicated by Sample Size Calculations (Targeted Cohort)).
Phase 2: Stratified Random Sample:
NIOSH will use a three-level sampling design to sample from career/mostly career and volunteer/mostly volunteer departments across the country (Appendix A). The U.S. will be divided into nine geographic units that fall within the four US regions (Northeast, Midwest, South, West) specified by the U.S. Census Bureau (i.e., New England, Middle Atlantic, East North Central, West North Central, South Atlantic, East South Central, West South Central, Mountain, and Pacific; https://www2.census.gov/geo/pdfs/maps-data/maps/reference/us_regdiv.pdf). Using recent national estimates from fire department surveys or databases (e.g., NFPA, USFA, FireCARES), departments within each region will be stratified by career/mostly career and volunteer/mostly volunteer status. Career/mostly career departments will then be categorized according to population size served (i.e., >100,000 vs. <100,000). The population size served for all departments will be obtained from resources on department characteristics and population data, including USFA, NFPA, FireCARES, and the U.S. Census. From each geographic region, NIOSH will first randomly select at least three career/mostly career departments with at least 100 current firefighters from each category of population size served to invite to participate (Tier 1); and will then randomly select at least three volunteer/mostly volunteer departments to invite to participate (Tier 2). Volunteer departments will not be stratified by population size served since a majority serve populations of <50,000, therefore it may be difficult to find larger volunteer departments in some regions.
b. Targeted Cohort: State Firefighter Certification Databases
In addition to the fire department sampling frame, NIOSH will incorporate other sampling frames for the Targeted Cohort, including state rosters of certified firefighters. A few states (e.g., Georgia, Kentucky, Ohio, etc.) require all firefighters, career and volunteer, to be certified and regularly re-certified to be active in that state. Each of these states has a governing body that keeps track of all active firefighters and their certifications. NIOSH will work with these states to obtain contact information (e.g., name and email address) for all currently active firefighters in that state. All new firefighters identified in state records sent to NIOSH periodically (e.g., every two or three years) will be invited to enroll. Additionally, some states could potentially include a link or invitation to the NFR during their initial certification and/or recertification process. Some of the state governing bodies may also have access to incident records. NIOSH will explore obtaining these records either from the state or from individual fire departments in the state. In most cases, however, state certification databases are not anticipated to have records with the level of detail related to fire incidents that are available from individual departments.
c. Sample Size Calculation (Targeted Cohort)
A sample size calculation was used to determine the minimum baseline sample sizes (i.e., number of currently active firefighters) necessary to detect elevated cancer rates for select subgroups of interest. The sample size calculations were based on attaining 80% power from a Poisson regression with 30 years of follow-up, comparing the observed cancer rate of the cohort to the U.S. population cancer rate with an α = 0.05 level of significance. It was further assumed that the cohort would grow by 2.5% per year as was calculated from the Daniels et al. (2014) study data. Population death rates and cancer incidence rates were obtained from CDC Wonder and the average of the most recent 5 years (2012-2017 for mortality and 2011-2016 for incidence) was used and assumed to remain constant into the future. Using this information, an initial targeted cohort of 5,000 firefighters is needed to observe a standardized incidence ratio (SIR) of 1.09 for all cancer sites among a general sample of firefighters; a similar number of non-white firefighters (i.e., 6,500) is needed to observe an SIR 1.09 for all cancer sites among a sample of only non-white firefighters; and 1,000 female firefighters are needed to observe an SIR of 1.45 for breast cancer among a sample of only female firefighters. The SIRs for these calculations were obtained from the Daniels et al. (2014) study.
These sample sizes were used to determine the minimum number of departments to recruit with the fire department sampling strategy. More specifically, mean reported counts of firefighters from a recent NFPA census of U.S. fire departments were used to estimate current workforce sizes. Under an assumption of 50% participation rate, we estimate that the proposed fire department sampling strategy (Appendix A) will contribute a baseline sample of roughly 26,000 firefighters, including approximately 1,000 women, 6,500 non-white firefighters, and 5,000 volunteers, that will grow to roughly 56,000 after 30 years of follow-up by 2050 (assuming an annual growth rate of 2.5%). The number of necessary fire departments could change based on observed participation rates and participation from state firefighter certification databases.
NIOSH anticipates including several states’ firefighter certification databases in the Targeted Cohort, which would greatly increase the sample size and potentially reduce the number of individual departments necessary to recruit for the fire department sampling strategy. Hypothetically, if a state with 40,000 active firefighters participated in the NFR, the Targeted Cohort would increase by roughly 20,000 participants, assuming the same participation rate as above. Thus, a total Targeted Cohort of approximately 46,000 firefighters at baseline would grow to approximately 100,000 after 30 years of follow-up. Additions of departments with high participation from the Open Cohort would further increase the size of the Targeted Cohort.
With high participation from fire departments selected in the fire department sampling strategy and multiple states, the Targeted Cohort will be used to evaluate even smaller measures of effect, more subgroups of firefighters, and rarer cancers.
2. Open Cohort
The Open Cohort will involve a non-probability sampling design and include all firefighters that complete enrollment through the secure web portal not otherwise recruited for the Targeted Cohort. All adult members of the U.S. fire service, including active, former, and retired members, who have ever been an active firefighter will be eligible to join the NFR through this method. This will include former firefighters at fire departments selected for the Targeted Cohort. Additionally, the Open Cohort will be designed to recruit large representation from sub-specialties of firefighting, such as wildland, instructors, fire investigators, and airport rescue. Participants will be able to enroll on a continuous basis.
Firefighters will be recruited for the Open Cohort by disseminating informational and promotional materials through stakeholders, membership organizations, social media, and trade literature. Appendix B provides an informational brochure. These materials will be provided to our list of stakeholders (Appendix C) for dissemination to their membership.
NIOSH investigators will deliver presentations on the NFR at professional conferences and meetings all over the United States. NIOSH will also set up booths at professional conferences where firefighters can obtain informational materials and possibly even register by using electronic tablets at the booth.
Through non-probability sampling, some firefighters may be more likely to register than others based on characteristics such as cancer status (i.e., selection/participation bias). Therefore, the Open Cohort may limit the ability of investigators to make statistical inferences related to cancer rates from this sample. Nevertheless, enrolling large numbers of NFR participants through this design will be relatively quick and cost-effective. Further, because of the broad eligibility criteria, this approach would provide the opportunity for any fire service members to participate in the NFR, including subgroups not initially eligible or selected for the Targeted Cohort. Lastly, previous cohorts of a similar design (e.g., the Women’s Health Initiative Observational Study and Nurse’s Health Study III) have demonstrated that the Open Cohort will have strong utility for descriptive and hypothesis-generating analyses of cancer risk factors, including those cross-sectional and prospective in design (Hays, et al. 2003; Chlebowski, et al. 2019; Bao, et al., 2016).
a. Adding Open Cohort Groups to the Targeted Cohort
NFR investigators will evaluate the opportunity for treating subgroups from the Open Cohort as part of the Targeted Cohort and/or additional department records collection based on the estimated severity of participation bias (e.g., based on cancer status) and participation rates of such subgroups (e.g., high participation from single departments, states, or organizational memberships for which denominator information is available). For example, if select departments have high participation (e.g., >70% of the department’s fire personnel) in the Open Cohort and, thus, minimal participation bias based on cancer status, NFR investigators may treat this subgroup as part of the Targeted Cohort; that is, by possibly soliciting incident records and performing prospective analyses related to cancer incidence. NIOSH will determine participation rates using denominator information available from NFPA, USFA, and/or contact with individual departments/states.
b. Power/Sample Size Calculation (Open Cohort)
Previous power calculations for a cohort of a similar design to the NFR Open Cohort have shown the capability of such an approach. For example, the Women’s Health Initiative Observational Study provides the opportunity for comparing characteristics between participants that have developed a given disease (e.g., cancer) with a suitable number of time-from-enrollment matched controls, i.e., using a nested case-control analysis. Power analyses demonstrate that, for example, a 1:1 matched case-control analysis based on a cohort size of 80,000 is approximately equal to a full-cohort analysis based on a cohort of size 40,000. Furthermore, in a hypothetical cohort of 40,000, investigators suggest that “an odds ratio as small as 1.50 for an exposure having a frequency of 0.50 can be detected with a probability (power) of 90% or greater by an average of 3 years of follow-up for diseases such as breast cancer… having an annual incidence of at least 0.20%. Such an odds ratio can be detected with a power of 80% for much rarer diseases having an annual incidence of 0.05% by an average of 9 years of follow-up” (The Women's Health Initiative Study Group, 1998, pg. 90–91). The NFR Open Cohort is anticipated to be much larger than 40,000.
B. Stakeholder Participation and Advisory Committee
There are many stakeholders interested in the NFR (Appendix C). NIOSH investigators have identified a list of individuals and organizations to be included in communications regarding the NFR including representatives from academic institutions, other federal agencies, fire and emergency response organizations, firefighter unions, fire departments, and cancer registry experts. Specifically, members of the International Association of Fire Fighters (IAFF), International Association of Fire Chiefs (IAFC), Firefighter Cancer Support Network, United States Fire Administration (USFA), National Fire Protection Association (NFPA), and International Association of Wildland Fire (IAWF) have expressed interest in assisting with efforts to maximize participation in the NFR. In addition, the Firefighter Cancer Registry Act of 2018 specifically mentions generating representation of female, volunteer, and minority firefighters, so NIOSH investigators have communicated with representatives from the National Volunteer Fire Council (NVFC), Women in Fire, National Association of Hispanic Fire Fighters, and the International Association of Black Professional Fire Fighters (IABPFF).
NIOSH engages with stakeholders for the NFR through various forms of communication including periodic emails, quarterly newsletters, individual conference calls, and presentations at conferences. NIOSH investigators published a request for information (RFI) in the Federal Register and presented at meetings open to the general public including at the NIOSH Board of Scientific Counselors (BSC) bi-annual meeting and the 2019 Firefighter Cancer Symposium. Additionally, NIOSH investigators provided NFR updates to members of Congress and will continue to do so annually. Through these mechanisms, stakeholders were able to express opinions and share insights in both public and private forums, and their perspectives were instrumental during the development of the protocol. NIOSH investigators will continue to provide opportunities for stakeholder feedback at upcoming conferences.
Additionally, the NFR team will continue holding conference calls with important stakeholder groups, such as IAWF and IAFF, to discuss recruitment strategies and disseminate promotional materials being developed as part of a promotional campaign for the NFR. This campaign will include a social media plan and digital advertisements to reach firefighters through CDC and NIOSH social media channels and leverage relationships with stakeholders such as unions and affinity groups that will share information and materials on behalf of the NFR team. The NFR team is using firefighter focus groups to inform the development of this promotional campaign. NIOSH investigators also created an email address (NFRegistry@cdc.gov) solely dedicated to answering questions regarding the NFR. Through a subcommittee of the NIOSH BSC, NIOSH created the NFR Subcommittee—an advisory committee for the NFR. The NFR Subcommittee, as outlined in the Firefighter Cancer Registry Act of 2018, is comprised of non-federal experts in related fields including cancer registries, cancer epidemiology, clinicians with expertise in cancer or firefighter health, fire and emergency response organizations, active firefighters, state health departments, and state departments of homeland security. The NFR Subcommittee will provide guidance on the design, implementation, and reporting for the NFR and meet at least once a year.
The results from our study will be communicated to stakeholders via scientific journal publications, presentations, and communications to the public.
C. Objectives
Objective 1: Enroll firefighters and collect self-reported information on employment/workplace characteristics, exposure, demographics, lifestyle factors, co-morbidities, and other confounders related to cancer.
NIOSH will develop a secure web portal that allows any firefighter in the nation to self-register. All firefighters participating in the NFR will enroll through the web portal. The web portal will meet all requirements of the Federal Information Security Management Act of 2002 (FISMA). Firefighters will access the web portal through the dedicated NFR website (www.cdc.gov/niosh/firefighters/registry.html or www.cdc.gov/NFR). This website will include frequently asked questions (FAQs) and other important background information about the NFR. After reviewing the NFR website, if firefighters are interested in enrolling in the NFR, they will click the “REGISTER” icon. This will take them to the secure web portal, which will have multi-factored authentication (MFA) (see Data Security section for more details). The NFR team will pilot test the enrollment process with multiple firefighters prior to deploying the web portal nationwide. Appendix A.2 outlines the planned enrollment process and design steps following enrollment.
a. Enrollment
To complete enrollment in the NFR, the firefighters will need to first complete the informed consent document (Appendix D) and then the user profile (Appendix E) and then the enrollment questionnaire (Appendix F). Icons for each of these documents will be included on their profile page or dashboard. If firefighters have questions that are not included or fully answered in the FAQs, they can call the NIOSH investigators at the phone number provided on the informed consent document.
After completing and electronically signing the informed consent document, the firefighters will be taken to the user profile page. This page will serve to collect basic information from the firefighter that could change over time and hence can be accessed and updated by the user. After completing the user profile questions, the firefighter will be directed to complete the enrollment questionnaire. The questionnaire will collect information on employment/workplace characteristics, exposure, demographics, lifestyle factors, co-morbidities, and other confounders. The enrollment process, including the questionnaire, is expected to take 30–45 minutes to complete and has been pilot tested with multiple firefighters from a variety of backgrounds to ensure clarity and brevity prior to deployment. Further pilot testing will continue in an electronic format to test the enrollment process and system load.
The very last question on the questionnaire asks for the participant’s Social Security Number (SSN). The questionnaire explains why the SSN is needed, “In the United States, each state has a cancer registry that collects and combines information on all cancer diagnoses from all hospitals in that state. In order to match the information you have provided in this survey with any potential cancer diagnosis reported to a state, we need your social security number (SSN).” If a firefighter submits the questionnaire without providing their SSN, a warning textbox will pop-up that says,
“We noticed that you did not include an SSN. Would you consider providing the last four digits of your SSN? Although not as reliable as your full SSN, the last four digits of your SSN would increase the likelihood of linking your information to any future cancer diagnosis.”
Two clickable icons will be provided in the text box:
Yes, I’ll provide my last four digits here
No, I do not wish to ensure my identity is correct. I understand this may exclude my information from analyses conducted to estimate cancer risks in firefighters.
This language has been discussed with stakeholders at multiple meetings and conferences and has been reviewed by firefighters, investigators, cancer researchers, and health communication specialists. The NFR team will hold additional focus groups with firefighters to discuss potential communication strategies for the NFR, including discussion items about the collection of SSNs. Promotional materials will be developed to communicate the importance of collecting SSNs based on feedback received through these focus groups and other conversations. If firefighters are unable to complete the questionnaire in one sitting, they can log-off and return at a later date to complete it. If they have not completed the questionnaire within 7 days of completing the informed consent, the firefighters will be sent a reminder email using the email address they provided during login and/or a text message using the mobile phone number they provided as part of the registration process. If necessary, another reminder email or text message will be sent 14 days, 28 days, and 42 days later. If there is no response after 42 days, no further emails or text messages will be sent.
Once the questionnaire has been completed and submitted, all responses will be uploaded to a secure server and the firefighter participant will no longer be able to access their questionnaire responses. However, the profile page or dashboard will include the profile data that were entered (see Appendix E). All this information can be viewed and edited from the dashboard, but only after the participant successfully logs in using MFA.
b. Follow-Up Questionnaires and Continued Engagement
Following enrollment, NIOSH will send NFR participants notifications for periodic follow-up questionnaires (e.g., one per year) to be filled out through the web portal. These follow-up questionnaires will contain questions related to documenting changes in work history (e.g., incident frequency/type, department, position), workplace practices (e.g., PPE use, shiftwork), and covariates (e.g., smoking and alcohol use) longitudinally, as well as more focused questions related to particular risk factors or health outcomes (e.g., reproductive health and breast cancer risk factors). These questionnaires will be voluntary but important for understanding the relationship between firefighting and health status over time. All questionnaires will be designed to be short and minimize the time burden on NFR participants.
In addition to notifications for follow-up questionnaires, NIOSH will send NFR participants regular updates/newsletters (e.g., every six months) by email and/or text message to keep participants engaged and remind them to keep their contact information and user profile information up to date. Additionally, NIOSH may provide links to recent publications, study opportunities, or preliminary results from the NFR in the participants’ user profile. This continued engagement will also likely improve response rate for follow-up questionnaires and provide a mechanism for notifying participants of external study opportunities (refer to Sharing Data with External Investigators).
Objective 2: Obtain records from fire departments/agencies to track trends and patterns of exposure as related to cancer in firefighters.
In addition to roster information, NIOSH will request fire incident records dating back to January 1, 2010, or earlier when available, from fire departments participating in the Targeted Cohort. Fire departments are required to collect some basic information about fire incidents under the National Fire Incident Reporting System (NFIRS) established by the U.S. Fire Administration. Department incident records will provide NIOSH investigators with apparatus and incident-specific information to be used as surrogates of exposure for exposure-response analyses. Specific variables of interest that will be requested from department incident records will include but are not limited to: incident number, fire station, apparatus, incident type (structure fire, car fire, etc.), on scene time, off scene time, job assignments, number of fire runs, and duration at fires. For departments able to share their incident records as part of the Targeted Cohort, NIOSH will explore obtaining records directly through states, NFIRS, and/or software vendors (FIREHOUSE, ImageTrend, etc.) to reduce the burden on each participating fire department. This process will be pilot tested prior to collection of records.
NIOSH will also solicit employment records for firefighters participating in the NFR, which will provide investigators with key individual-level information. Specific variables of interest requested from employment records for each firefighter participating in the NFR will include but are not be limited to: full name, employee ID, current and past job titles (e.g., recruit, firefighter, chief, etc.), hire date, termination date (if applicable), promotion history, duration of employment, fire station, apparatus, and crew assignment(s). Where possible, NIOSH will attempt to collect electronic records from departments instead of paper records.
Meetings will be held with individual departments and local unions to reach agreement on their support to participate in the Targeted Cohort. Specifically, the NFR team will work with individual fire department leadership to determine the most effective and secure mechanism for sharing employment and incident records with NIOSH. This will include employment records for all fire personnel participating in the NFR and department incident records dating back to at least January 1st, 2010 or earlier when available (i.e., for information on eligible firefighters that were active at the department prior to 2010). Data use agreements (DUAs) can be developed if necessary.
Firefighters from departments in the Targeted Cohort will be asked to enroll through the NFR web registration. NIOSH investigators will be able to track response rate by running queries of the database. NIOSH investigators will code work history and incident and response records and combine data from each department into one database with linkages to individual participants where such linkages can be reliably made.
Additionally, if participants are currently tracking their exposures, they can individually give the exposure tracking programs (e.g., PER, NFORS, PIIERS, FirstForward) permission to provide this information to the NFR. At this time, it is not clear how many firefighters use exposure tracking systems, how long they have been using these systems (most are relatively new), or how complete or consistent the data are across the different platforms. If these programs gain in popularity and meet specific data standards and quality, there may be an opportunity to use the data to estimate exposures longitudinally, at least for certain groups of firefighters (e.g., new recruits). Therefore, although exposure tracking programs are not the primary data source for estimating lifetime exposures, the NFR program will consider these data for exploratory analyses and possible use in future assessments of exposure. Other data collection methods for individual and department level information will also be considered and added as amendments to this protocol.
Objective 3: Monitor cancer in firefighters by linking with health information databases (e.g., population-based cancer registries and the National Death Index) to assess cancer incidence and mortality.
NIOSH will identify all cancer diagnoses and determine vital status for all NFR participants by periodically linking with health information databases. These linkages will be used to associate NFR participants’ occupational information with cancer and/or cause of death information. NIOSH will link to all outcome databases (i.e., Social Security Administration Death Master File, NDI, and population-based cancer registries) using identifying information ascertained in the NFR web portal’s profile and enrollment questionnaire (e.g., name, social security number, date of birth, address, sex).
For participants who become deceased, we will obtain underlying and contributing causes of death from NDI to determine cancer mortality and mortality due to other causes. Cancer incidence will be determined to more accurately assess the risk of specific cancers in the initial analysis and among living participants at each period of follow-up (i.e., linkage update), which is a more accurate measure for cancers with high survival rates (e.g., testicular and prostate). Cancer diagnoses will be identified by matching participant records with applicable population-based cancer registries (commonly referred to as state cancer registries) from all states and territories in the U.S. Records will be obtained from cancer registries either by applying for data from registries individually or, when available, from pooled resources such as the North American Association of Central Cancer Registries’ Virtual Pooled Registry Cancer Linkage System (NAACCR VPR-CLS), which is an automated, standard linkage methodology and streamlined application process available for cancer registries that volunteer to participate (https://www.naaccr.org/about-vpr-cls/). The VPR-CLS offers a secure mechanism for NIOSH to submit NFR identifiers for linking with participating state cancer registries. The deliverable to NIOSH will be a report of the number of matches by state that occurred, allowing NIOSH to prioritize individual state cancer registries for individual-level data exchange.
In order to conduct further vital status tracing over time and ensure quality control in data linkages, NIOSH will refer to existing administrative records resources, such as those available through the Internal Revenue Service (IRS) and LexisNexis.
Vital status, cause of death, and cancer incidence data will be updated periodically as new participants enroll and as the cohort ages. Linkages between exposure, demographic, and lifestyle information and mortality/cancer diagnosis information will be used to determine rates of death due to cancer and other causes, as well as the incidence of cancer among firefighters, overall and for specific subgroups/subspecialties of firefighters (e.g., men, women, non-white or minority, instructors, investigators, urban/rural, structural/wildland, career/volunteer, geographic regions, exposure amounts).
V. DATA MANAGEMENT AND ANALYSIS:
A. Data security
Account creation begins with the interested participant clicking the “Register” button on the CDC/NIOSH NFR web portal application. This self-registration initiates the process of creating a login.gov managed account. Login.gov is a single sign-on solution for U.S. government websites. This federal government service enables participants to log in to federal government applications using MFA. MFA is an authentication method that requires more than one method of authentication from independent categories of credentials to verify the user’s identity for a login or other transaction. When the participant clicks the “Register” button it will redirect to login.gov where they can sign in or create an account. The login.gov page that the participant is redirected to will be branded with the NFR logo to give the participant a consistent user interface experience.
Account creation requires entering one’s first and last name and an email address or phone number, creating a password and confirming it, and choosing a preferred language from a drop-down menu. The web portal will require firefighters to create an account using MFA. Briefly, the firefighters will enter their email address and a strong password and then be asked to provide at least two levels of authentication, which could include: 1) passcode via text message to their mobile phone; 2) security token via third-party authenticator app; and/or 3) answers to challenge questions. Through the login.gov authentication process, a universally unique identifier (UUID) that identifies the user is assigned to the participant. The firefighters’ UUID and email will be shared with NIOSH. Participants can find assistance for creating accounts at https://login.gov/help/. After account creation, the participant is redirected back to the NFR web portal with the UUID that identifies the participant. After completing account creation (and informed consent document if not already signed), the firefighters will be taken to a profile page and asked to enter (or update if returning to the site) their legal first, middle, and last name; current email address, mobile phone number, current or most recent fire department, current work status, and job title (see Appendix E). This will establish their profile.
The NFR web portal will have a register/log in button. When the participant clicks the button, it will redirect to login.gov to handle the MFA process. Every time the participant signs in to the NFR web portal, they will need their email address, their password, and access to one of the two-factor authentication methods they chose to set up. After the participant enters their email address and password to sign in, login.gov will ask them to authenticate (enter a security code sent to their phone by voice or text or enter the security code from their authentication application). After authenticating with login.gov, they are redirected back to the NFR web portal. Once a participant is authenticated on login.gov and passed back to the NFR web portal, the session will be managed by secure CDC on-premise infrastructure, including CDC-managed web servers and database servers.
When completing the questionnaire (Appendix F), firefighters will be automatically logged-off if there is no online activity for 5 minutes. To log back in, the firefighters will be required to successfully perform MFA as described previously.
3. Password management
To change their password, participants will be redirected to the “Manage Account” page on login.gov. They will select “Edit” next to password, enter the new password and submit their change. Login.gov enforces strong passwords that meet National Institute of Standards and Technology (NIST) requirements
4. Encryption
Collected data (including questionnaire data, exposure data, and matched cancer data) will be stored by unique participant ID. This unique participant ID will be a UUID, assigned by login.gov. User accounts will be proofed at (LOA3), corresponding to NIST 800-63-2 levels of assurance (LOA). All collected data will be stored in a secure database that meets NIST 800-53, SC-28 PROTECTION OF INFORMATION AT REST standards. Multiple layers of encryption will be implemented on the database. Information in Identifiable Form (IIF) fields will be masked on the Graphical User Interface because of the sensitivity of the data. For example, month and year of birth will be masked.
5. Minimize collection of identifiable information
The information required for registration has been limited to only that needed to confidently link an individual to state cancer registries and the NDI.
6. Internal Access
Restrictions on internal access and auditing of internal access will be implemented to meet the controls listed in NIST Special Publication 800-53 (as amended), Security and Privacy Controls for Federal Information Systems and Organizations.
7. Physical and Environmental Protection (PE)
CDC facilities meet security controls in accordance with the PE security control requirements stated in NIST SP 800-53, Revision 4, Security and Privacy Controls for Federal Information Systems and Organizations. Servers are stored in a server room secured by the CDC. Physical controls are in place to secure entry into CDC buildings (Guards, ID Badges, Key Card, Cipher Locks, and Closed-Circuit TV).
All incidents involving a suspected or confirmed breach of Personally Identifiable Information (PII) must be reported to CDC Office of the Chief Information Security Officer (OCISO) according to the policy titled “OCISO/CDC Standard for Responding to Breaches of Personally Identifiable Information (PII).”
The primary goal of this surveillance system is to monitor trends in cancer incidence among firefighters (e.g., incidence rates), as specified in the mandate. Beyond this goal, the data will be evaluated by NIOSH staff and external researchers for various potential analytic objectives, including but not limited to descriptive and hypothesis-generating investigations of cancer risk factors, exposure-response analyses, and comparisons of cancer risk and risk factors between subgroups of firefighters as well as external/general populations. Data analysis objectives and plans may change and evolve over time as the cohort grows and surveillance needs develop. While the objectives in this protocol outline the design of the NFR, a data analysis plan for select analyses related to the primary goal of the NFR is described below.
1. Comparing Cohort Characteristics
Initially, characteristics of NFR sample subgroups will be evaluated to understand inherent discrepancies between enrollment groups of the NFR sample. Because of the varying enrollment strategies implemented for the sampling design, firefighters may differ depending on whether they were enrolled through the Targeted Cohort Phase 1, Targeted Cohort Phase 2, or Open Cohort. Baseline characteristics will be compared to assess the advantages of stratified and sensitivity analyses, identify potential confounding variables, and evaluate the impacts of pooling data for any analyses. The examination of subcohort characteristics will also aid in identifying the level of selection bias in the Open Cohort, and subsequently the ability to pool these participants with the Targeted Cohort for prospective (e.g., mortality and incidence) analyses of cancer.
2. Analyzing Mortality and Cancer Incidence Rates
Mortality and cancer rates will be calculated and compared to the general U.S. population as was done in previous NIOSH studies of firefighters (Daniels et al., 2014; Pinkerton, et al., 2020). State rates will be used for comparison where available. Briefly, mortality rates will be assessed by using the NIOSH Life Table Analysis System (LTAS.NET) or a similar program to generate expected numbers of cancer deaths (NIOSH, 2001). Enumeration of observed deaths and person-years at risk for NFR participants will begin at enrollment and end at the date deceased or end of observation, whichever is earliest. Numbers of deaths observed for each cause (e.g., cancer site) will be divided by the expected number of deaths to obtain cause-specific standardized mortality ratios (SMRs). The precision of each estimated SMR will be assessed assuming a Poisson or Negative Binomial distribution, with two-sided 95% confidence intervals.
To analyze cancer incidence, SIRs, person days at risk, and the expected number of cancer incidence cases will be calculated using LTAS.NET, SEER*Stat, or a similar program. The methods for producing these estimates are the same as those used for the mortality analyses. Person-days at risk will accumulate beginning at enrollment. Each individual contributes person-days until the date of diagnosis of cancer, the date of death, or the end of observation, whichever is earliest.
Regression analyses will be conducted to further evaluate the associations between risk factors and selected cancer outcomes through internal comparisons. In general, exposure-response modeling of longitudinal data will be approached using standard methods of regression modeling of survival data (i.e., failure-time data). Analysis plans guiding specific modeling strategies will be developed based on review of available data.
Analyses of the Targeted Cohort might potentially incorporate sampling weights, as appropriate, for the oversampling of women and minorities of Phase 1 and the stratified sampling design of Phase 2 to improve the generalizability of results.
C. Potential Limitations and Considerations
The proposed approach for the NFR surveillance system has some limitations. The Targeted Cohort will be much more resource-intensive than the Open Cohort, but it provides the most scientifically rigorous method for assessing prospective cancer incidence and mortality and a streamlined method for obtaining incident records. Despite specific inclusion criteria and a sampling design for the Targeted Cohort, the participant population will be limited to fire service personnel from departments/states that are willing and able to participate in the NFR. These departments and states may employ workplace practices and policies for firefighters that differ from departments/states that decline or are unable to participate in the NFR, potentially limiting the generalizability of the NFR. Additionally, efforts to ensure large representation of women, minorities, and volunteers from large departments in Phase 1 of the Targeted Cohort may further impact generalizability of a pooled sample. Some analyses like mortality/incidence for rare cancers and subgroups (e.g., women, minorities, rural, volunteers) of firefighters may be limited by small sample sizes; and sample sizes for smaller subgroups may not be generalizable (e.g., samples of women and minorities, who will likely come from mostly large/urban settings in certain regions).
NIOSH will have the ability to identify potential biases affecting the NFR sample by comparing the demographics and characteristics of NFR participants to those of the U.S. firefighter workforce that are provided by external sources, such as NFPA, USFA, and the U.S. Bureau of Labor Statistics. Likewise, internal comparisons of NFR subsamples will identify strengths and limitations of pooling data, stratified analyses, sensitivity analyses, and controlling for select covariates. Additionally, with roster information available from fire departments and states selected in the Targeted Cohort serving as denominator estimates, NIOSH will be able to evaluate estimates of response and non-response.
Exposure-response analyses using department incident records will be limited to participants and time periods for which records are available from each department. However, questionnaire data will be used to examine exposure-response for all participants based on comprehensive work history and estimated number of fire responses (even across multiple departments).
The NFR analyses may be affected by “healthy worker” biases since a firefighting population is healthier than the general U.S. population, and firefighters in the Targeted Cohort must have survived until present day to be eligible (healthy worker survivor effect (HWSE)) (Checkoway et al., 1989; Naimi et al., 2013). These biases will be evaluated analytically where possible. Methods accounting for HWSE are currently evolving (e.g., Naimi et al., 2013). NIOSH will keep current with the literature on HWSEs and utilize proven methodology as practicable.
The ability to perform lagged analyses may be difficult where timing of exposures or behaviors cannot be accurately ascertained through self-report. However, information will be obtained longitudinally with follow-up questionnaires and cancer can also be evaluated prospectively in relation to some self-reported information after expected latency periods have occurred. Timing of incidents/practices will also be available from department records for some participants and some self-reported items in the questionnaire for all participants. However, because of the long latency period of cancer and the NFR’s prospective design, it will be some time before cancer incidence rates, comparisons with the general population, and some cancer risk factors may be evaluated.
VI. HUMAN SUBJECTS PROTECTIONS
A. Surveillance and Research Activities
The primary objective of the NFR is to monitor cancer and cancer risk factors among the U.S. fire service. This primary objective is a public health surveillance activity deemed not to be research under the 2018 Requirements (subpart A of 45 CFR part 46), and therefore does not require Institutional Review Board (IRB) submission.
By definition, public health surveillance activities include “the collection and testing of information or biospecimens, conducted, supported, requested, ordered, required, or authorized by a public health authority. Such activities are limited to those necessary to allow a public health authority to identify, monitor, assess, or investigate potential public health signals, onsets of disease outbreaks, or conditions of public health importance (including trends, signals, risk factors, patterns in diseases, or increases in injuries from using consumer products)” (https://www.hhs.gov/ohrp/regulations-and-policy/requests-for-comments/draft-guidance-activities-deemed-not-be-research-public-health-surveillance/index.html). The NFR has been authorized by CDC/NIOSH to collect information to allow NFR investigators to identify and monitor cancer trends and risk factors among the U.S. fire service. Public health surveillance activities of the NFR include ongoing recruitment and enrollment of participants; follow-up or supplemental questionnaire administration related to cancer and cancer risk factors, including but not limited to work history, exposure, comorbidities, and lifestyle characteristics; and routine linkages with NDI and cancer registries to determine cancer status and/or cause of death.
NIOSH investigators will create and administer follow-up questionnaires to capture additional information related to firefighters’ work, cancer, or other health conditions. Any potential questionnaires not related to the primary goal of monitoring cancer and cancer risk factors among firefighters will need to undergo research/non-research determination at CDC/NIOSH. If the questionnaires and related activities are deemed a public health surveillance activity under the goals of the NFR, they will be added to this protocol as an amendment and submitted for review and approval according to CDC/NIOSH procedures. The questionnaire will also be submitted to the U.S. Office of Management and Budget (OMB) for approval. If the new questionnaires are deemed research, the NIOSH investigators will develop a new protocol, undergo CDC/NIOSH review procedures, and obtain all the necessary IRB and OMB approvals before posting these questionnaires to the web portal and notifying participants via email or text message of the new questionnaire.
External researchers can also request that NIOSH reach out to NFR participants to solicit their interest in an outside study. NIOSH will review and approve these requests on a case-by-case basis, ensuring that all studies have received appropriate review and approvals. Once NIOSH has approved the proposal, the NFR program will be responsible for re-contacting participants and sharing resources for the external study.
Additionally, NIOSH is required to make NFR data available to external researchers as stated in the legislation (subparts (2)(f)-(g)). See the Assurance of Confidentiality section (below) for more details on how data will be made available to external researchers.
NIOSH will obtain informed consent as described in Objective 1. Interested firefighters will be able to read the consent form in its entirety and provide an electronic signature indicating their consent. If firefighters have questions, they will be referred to the FAQs on the NFR website and if their questions are not answered there, we will provide a phone number that they can call to reach a member of the NFR investigation team. The consent form was determined to have a Flesch-Kincaid 10th grade reading level and was thought to be adequate for the target audience of firefighters. It is important to note that most career fire departments require at least a high school education and nearly all fire departments (including volunteer departments) require fluency in English.
C. The Reasonable Person Standard
Application of the reasonable person standard is required by the revised Common Rule in development of the consent process and form. That is, the consent form must provide the information that a reasonable person would want to have in order to make an informed decision about whether to participate. Key Information is the phrase used to describe a new requirement for consent processes and forms: Obtaining consent must begin by presenting the potential participants with the key information that is most likely to assist them in understanding the reasons why they might or might not want to participate in this surveillance project.
Based on conversations the NFR team has had with stakeholders, it is clear that confidentiality of data is of utmost importance to the firefighters. It is also clear that there is confusion among firefighters regarding who can register in the NFR. Consequently, it is important that firefighters understand that their data will be protected to the fullest extent allowed by law and cannot be released to their fire departments or insurance companies and that all firefighters in the United States can register, regardless of their position or health status. The “Key Information” section of the consent form (first paragraph, Appendix D) provides these details in a short and understandable format so that a firefighter (or any reasonable person) has these details up-front as they continue to read the consent form. The rest of the consent form then provides additional details (including potential risks) that are also necessary to make an informed decision about whether or not to participate in the study.
In addition to the details in the consent form, the participants will also be provided with a link to FAQs (www.cdc.gov/niosh/firefighters/registry.html) and a phone number to reach a member of the NFR team if they have additional questions. However, we have strived to make the consent form comprehensive, concise, and understandable (Flesch-Kincaid grade level of 10.0), so that a reasonable person has all the information in the consent form necessary to decide whether or not to participate.
D. Confidentiality
1. Assurance of Confidentiality
NIOSH will seek to obtain an Assurance of Confidentiality (AoC) for the NFR. An AoC is a formal confidentiality protection authorized under Section 308(d) of the Public Health Service Act. An AoC protects individuals and institutions involved in either research or non-research (e.g., surveillance), thereby protecting the confidentiality of participants involved in both surveillance and any future research involving NFR data. Only individuals that are part of the NFR program will have access to directly identifiable information (e.g., name, SSN, email address, etc.). These individuals may include NIOSH employees, Federal contractors, or cooperative agreement partners. However, all individuals with access to direct identifiers will have to comply with the data security requirements outlined above in the Data Security section.
This protection will allow the NFR team to assure participants, departments, and other institutions that NIOSH will protect the confidentiality of the data collected. The legislation states that no identifiable information may be used for any purpose other than the purpose for which it was supplied, and that no disclosure of the data may be made unless such institution or individual has consented to that disclosure.
The main purpose of NFR data is to monitor cancer incidence among firefighters and evaluate the relationship between occupational factors and other risk factors and cancer incidence as specified under the Firefighter Cancer Registry Act of 2018. The data can also be analyzed for other purposes provided those purposes are related to public health surveillance or firefighter health and safety research.
NIOSH will make NFR data accessible, upon request, to external researchers through a Research Data Center (RDC). All requests for NFR data files must be made through a proposal to the RDC. The proposal will be reviewed by the RDC, NIOSH, and state cancer registry staff, if applicable. If approved by all parties, the appropriate de-identified data files will be provided to the RDC for analysis. All direct identifiers will be removed but indirect identifiers (e.g., sex, race, etc.) will be provided at the individual level for analysis. Some indirectly identifying data (e.g., cells with n<10) may be redacted to minimize the possibility of identifying participants through these identifiers. External researchers will only be permitted to leave the RDC with summary data tables which will be reviewed by RDC staff to ensure that participants cannot be indirectly identified.
Collected data (including questionnaire data, exposure data, and matched cancer and death data) will be stored by unique participant ID. This participant ID will be a UUID, assigned by login.gov. User accounts will be proofed at (LOA3), corresponding to NIST 800-63-2 levels of assurance (LOA). All collected data will be stored in a Transparent Data Encryption (TDE) database with the additional layer of column –level encryption for Personally Identifiable Information fields.
VII. RISKS AND BENEFITS:
A. Assessment of Potential Benefits
There are no direct benefits from participating in the NFR. However, firefighters will indirectly benefit from participating in the NFR by contributing to a knowledge base that could influence practices and policies aimed at preventing cancer in firefighting for generations to come. For example, the NFR could find that certain control measures are related to a reduced risk of cancer, which would provide additional evidence and support for fire departments to implement these measures.
B. Assessment of Potential Risks
The risk to participants in this study is minimal. There is a slight risk of unintended disclosure of the personal information for participants in this study. Participants may also experience emotional stress by participating in a study focused on cancer or answering questions related to cancer. However, these risks will be minimized as summarized below.
C. Description of Measures Taken to Minimize Potential Risks
Several steps are being taken to protect participants’ confidentiality and prevent unintended disclosure of personal information at each step along the registration, cancer diagnosis matching, data sharing, and dissemination processes.
Participants will only be able to enter their information, answer questions, and/or see previously entered responses after successfully logging in using MFA.
If a firefighter is uncomfortable answering a question, he or she can skip the question. All questions are optional.
Once the participants submit their questionnaire, their responses are uploaded to an on-premise secure and encrypted database. Their questionnaire and responses are then cleared from the web portal and can no longer be accessed by them, with the exception of the information that is part of their profile page or dashboard for possible future updating. This information includes firefighter’s name, current physical address, current email address, mobile phone number, current or most recent fire department, position, and employment status (Appendix E). This information will be editable from their profile page but can only be accessed after successfully logging in using MFA.
Following controls listed in NIST Special Publication 800-53, Security and Privacy Controls for Federal Information Systems and Organizations, data will be encrypted at rest and in transit.
3. Matching to State Cancer Registries and the National Death Index
Identifiable information provided to state cancer registries or the NDI for linkage will not be kept by those programs. State cancer registry data and NDI data are protected by Assurances of Confidentiality within the NIOSH Division of Field Studies and Engineering which restrict release of the data. Under the Assurance for death certificate data, NIOSH is allowed to share de-identified individual-level data with external investigators under an approved protocol and within a secure data enclave such as a National Center for Health Statistics - Research Data Center (RDC). The current AoC for cancer registry data does not permit NIOSH to share these data with external investigators. However, NIOSH is exploring an update to this AoC that would function in a manner similar to the death certificate Assurance and could permit sharing of de-identified individual-level data with external investigators via RDCs, if permitted by the state cancer registry.
4. Sharing Data with External Investigators
The NFR Team will be the stewards of the collected data. Individually identifiable data will not be shared with external researchers. External researchers will be able to request access to indirectly identifiable NFR data through an RDC as outlined in the Assurance of Confidentiality section (above).
Results will be published in academic peer-reviewed journals or NIOSH publications. All dissemination products will be reviewed following NIOSH publication guidelines. After NIOSH publication clearance and submission to the academic journal, results and findings will be further disseminated via trade magazine articles, presentations, and in other products through fire service stakeholders. Only summary aggregate data that cannot be linked back to an individual will be disseminated.
The NFR will include current or former U.S. firefighters and will exclude prisoners and children under the age of 18 as specified in the consent form. However, former prisoners who were once part of a wildland fire prison crew would be eligible to voluntarily register (open cohort). Because the web portal provides an opportunity for any firefighter to register, it is likely that our participant population will be diverse and include firefighters of both sexes and every race and ethnicity and socioeconomic background. Pregnant women are eligible to be included in the NFR. We are providing no incentives to participate in the NFR.
It is possible that firefighters will feel obligated to participate if their superiors were to tell them participation is required. In working with fire department management (and local unions) we will convey that the NFR is entirely voluntary. The voluntary nature of the NFR is also clearly noted in the recruiting flyer and consent form. If a fire department were to ask us who has registered from their department, NIOSH would only provide summary statistics (e.g., percent of their active firefighters who registered) that could not be used to identify specific people or subgroups.
E. Risk versus Benefit Evaluation
Information gleaned from this study is likely to result in better understanding of cancer in the fire service and improved protections for firefighters as a whole. The risks associated with this study are considered to be minimal. The primary risk is unintended disclosure of private information, and numerous safeguards will be in place to minimize that risk. The anticipated benefits are thought to outweigh the potential harm and discomfort to the study participants.
VIII. FUNDING: The NFR is funded annually by Congress as authorized in the Firefighter Cancer Registry Act of 2018 (H.R.931).
REFERENCES:
Abreu, A.C., C.; Silva, S.; Morais, S.; Pereira, M.; et al.
Wood smoke exposure of Portuguese wildland firefighters: DNA and oxidative damage evaluation.
J Toxicol Environ Health, 80 (2017)
Adetona, O.S., C.; Li, Z.; Sjodin, A.; Calafat, A.; Naeher, L.
Hydroxylated
polycyclic aromatic hydrocarbons as biomarkers of exposure to wood
smoke in wildland firefighters.
J
Expo Sci Environ Epidemiol, 27 (2017), pp.78-83
Adetona,
O.S., C.; Onstad, G.; Naeher, L.
Exposure
of wildland firefighters to carbon monoxide, fine particles, and
levoglucosan.
Ann
Occup Hyg, 57 (2013) pp. 979-991
Ahn,
Y.S.; Jeong, K.S.; Kim, K.S.
Cancer
morbidity of professional emergency responders in Korea.
Am
J Ind Med, 55 (2012), pp. 768-778
Alexander,
B.M.; Baxter, C.S.
Flame
Retardant Contamination of Firefighter Personal Protective Clothing -
a Potential Health Risk for Firefighters.
J
Occup Environ Hyg, (2016), pp. 1-26
Amadeo,
B.M., J.; Moisan, F.; Donnadieu, S.; Gaelle, C.; Simone, M.; Lembeye,
C.
French
firefighter mortality: analysis over a 30-year period.
Am
J Ind Med, 58 (2015), pp. 437-443
Andersen,
M.H.G.; Saber, A.T.; Clausen, P.A.; Pedersen, J.E.; Lohr, M.;
Kermanizadeh, A.; Loft, S.; Ebbehoj, N.; Hansen, A.M.; Pedersen,
P.B.; Koponen, I.K.; Norskov, E.C.; Moller, P.; Vogel, U.
Association
between polycyclic aromatic hydrocarbon exposure and peripheral blood
mononuclear cell DNA damage in human volunteers during fire
extinction exercises.
Mutagenesis,
(2017)
Aronson,
K.T., G.; Smith, L.
Mortality
among fire fighters in metropolitan Toronto.
Am
J Ind Med, 26 (1994), pp. 89-101
Bao, Y.; Bertoia, M. L.; Lenart, E. B.; Stampfer, M. J.; Willett, W. C.; Speizer, F. E.; Chavarro, J. E.
Origin, Methods, and Evolution of the Three Nurses' Health Studies
Am J Public Health, 106 (2016), pp. 1573-1581
Baris,
D.G., T.; Telles, J.; Heineman, E.; Olshan, A.; Zahm, S.
Cohort
mortality study of Philadelphia firefighters.
Am J Ind Med, 39 (2001), pp. 463-476
Bates,
M.N.; Fawcett, J.; Garrett, N.; Arnold, R.; Pearce, N.; Woodward, A.
Is
testicular cancer an occupational disease of fire fighters?
Am
J Ind Med, 40 (2001), pp. 263-270
Beaumont,
J.C., G.; Jones, J.; Schenker, M.; Signelton, J.; Piantanida, L.;
Reiterman, M.
An
epidemiologic study of cancer and other causes of mortality in San
Francisco firefighters.
Am
J Ind Med, 19 (1991), pp. 357-372
BLS.
Employed persons by detailed occupation, sex, race, and Hispanic or Latino ethnicity (2019).
Bolstad-Johnson,
D.M.; Burgess, J.L.; Crutchfield, C.D.; Storment, S.; Gerkin, R.;
Wilson, J.R.
Characterization
of firefighter exposures during fire overhaul.
AIHAJ,
61 (2000), pp. 636-641
Broyles,
G.
Wildland
Firefighter Smoke Exposure.
US
Forest Service (2013)
Casjens, S.; Brüning, T.; Taeger, D.
Cancer risks of firefighters: a systematic review and meta-analysis of secular trends and region-specific differences.
Int Arch Occup Environ Health, 93 (2020), pp. 839-852
Checkoway, H.; Pearce, N.E.; Crawford-Brown, D.J.
Research Methods in Occupational Epidemiology.
New York: Oxford University Press (1989)
Chlebowski, R. T.; Luo, J.; Anderson, G. L.; Barrington, W.; Reding, K.; Simon, M. S.; Manson, J. E.; Rohan, T. E.; Wactawski-Wende, J.; Lane, D.; Strickler, H.; Mosaver-Rahmani, Y.; Freudenheim, J. L.; Saquib, N.; Stefanick, M. L.
Weight loss and breast cancer incidence in postmenopausal women.
Cancer, 125 (2019), pp. 205-212
Congress.
U.S.
Firefighter Cancer Registry Act of 2018.
Daniels,
R.D.; Bertke, S.; Dahm, M.M.; Yiin, J.H.; Kubale, T.L.; Hales, T.R.;
Baris, D.; Zahm, S.H.; Beaumont, J.J.; Waters, K.M.; Pinkerton, L.E.
Exposure-response
relationships for select cancer and non-cancer health outcomes in a
cohort of US firefighters from San Francisco, Chicago and
Philadelphia (1950-2009).
Occup
Environ Med, 72 (2015), pp. 699-706
Daniels,
R.D.; Kubale, T.L.; Yiin, J.H.; Dahm, M.M.; Hales, T.R.; Baris, D.;
Zahm, S.H.; Beaumont, J.J.; Waters, K.M.; Pinkerton, L.E.
Mortality
and cancer incidence in a pooled cohort of US firefighters from San
Francisco, Chicago and Philadelphia (1950-2009).
Occup
Environ Med, 71 (2014), pp. 388-397
Demers,
P.A.C., H.; Vaughan, T.; Weiss, N.; Heyer, N.; Rosenstock, L.
Cancer
incidence among firefighters in Seattle and Tacoma, Washington
(United States).
Cancer
Causes Control, 5 (1994), pp. 129-135
Demers,
P.A.H., N.; Rosenstock, L.
Mortality
among firefighters from three northwestern United States cities.
Br J Ind Med, 49 (1992), pp. 664-670
Dreij,
K.M., A.; Jarvis, I.; Lim, H.; Hurkmans, J.; Gustafsson, J.;
Bergvaill, C.; Westerholm, R.; Johansson, C.; Stenius, U.
Cancer
Risk Assessment of Airborne PAHs Based on in Vitro Mixture Potency
Factors.
Environ
Sci Technol. 51 (2017), pp. 8805-8814
Easter,
E.; Lander, D.; Huston, T.
Risk
assessment of soils identified on firefighter turnout gear.
J
Occup Environ Hyg, 13 (2016), pp. 647-657
Ellis,
L.C., A.; Spiegel, D.; Ladabaum, U.; Haile, R.; Gomez, S.
Racial
and Ethnic Disparities in Cancer Survival: The Contribution of Tumor,
Sociodemographic, Institutional, and Neighborhood Characteristics.
J
Clin Oncol, 1 (2018), pp. 25-33
Fent,
K.W.; Alexander, B.; Roberts, J.; Robertson, S.; Toennis, C.;
Sammons, D.; Bertke, S.; Kerber, S.; Smith, D.; Horn, G.
Contamination
of firefighter personal protective equipment and skin and the
effectiveness of decontamination procedures.
J
Occup Environ Hyg, (2017),
http://dx.doi.org/10.1080/15459624.15452017.11334904
Fent,
K.W.; Eisenberg, J.; Snawder, J.; Sammons, D.; Pleil, J.D.; Stiegel,
M.A.; Mueller, C.; Horn, G.P.; Dalton, J. Systemic
exposure to PAHs and benzene in firefighters suppressing controlled
structure fires.
Ann
Occup Hyg, 58 (2014), pp. 830-845
Fent,
K.W.; Evans, D.E.; Babik, K.; Striley, C.; Bertke, S.; Kerber, S.;
Smith, D.; Horn, G.P.
Airborne
contaminants during controlled residential fires.
J
Occup Environ Hyg, (2018), pp. 1-34
Fent,
K.W.; Mayer, A.; Bertke, S.; Kerber, S.; Smith, D.; Horn, G.P.
Understanding
airborne contaminants produced by different fuel packages during
training fires.
J
Occup Environ Hyg, 16 (2019a), pp. 532-543
Fent,
K.W.; Toennis, C.; Sammons, D.; Robertson, S.; Bertke, S.; Calafat,
A.M.; Pleil, J.D.; Geer Wallace, M.A.; Kerber, S.; Smith, D.L.; Horn,
G.P.
Firefighters' and instructors' absorption of PAHs and benzene during
training exercises.
Int
J Hyg Environ Health, 222 (2019b), pp. 991-1000
Freeman, M.; Pollack, L.; Rees, J.; Johnson, C.; Rycroft, R.; Rousseau, D.; Hsieh, M.
Capture and coding of industry and occupation measures: Findings from eight National Program of Cancer Registries states. Am J Ind Med, 60 (2017), pp. 689-695
Fritschi,
L.G., D.
Firefighters
and cancer: where are we and where to now?
Occup
Environ Med, 71 (2014), pp. 525-526
Glass,
D.D.M., A.; Pircher, S.; Vander Hoorn, S.; Sim, M.
Mortality
and cancer incidence at a fire training college.
Occup
Med (Lond), 66 (2016a), pp. 536-542
Glass,
D.D.M., A.; Pircher, S.; Vander Hoorn, S.; Sim, M.
Mortality
and cancer incidence in a cohort of male paid Australian
firefighters.
Occup
Environ Med, 73 (2016b), pp. 761-771
Glass,
D.D.M., A.; Pircher, S.; Vander Hoorn, S.; Sim, M.
Mortality
and cancer incidence among male volunteer Australian firefighters.
Occup Environ Med, 74 (2017), pp. 628-638
Glass,
D.D.M., A.; Pircher, S.; Vander Hoorn, S.; Sim, M.
Mortality
and cancer incidence among female Australian firefighters.
Occup
Environ Med, 76 (2019), pp. 215-221
Guidotti,
T.L.
Mortality
of urban firefighters in Alberta, 1927-1987.
Am
J Ind Med, 23 (1993), pp. 921-940
Guidotti,
T.L.
Evaluating
causality for occupational cancers: the example of firefighters.
Occup Med (Lond), 57 (2007), pp. 466-471
Harris,
M.K., T.; MacLeod, J.; Tjepkema, M.; Peters, P.; Demers, P.
Surveillance
of cancer risks for firefighters, police, and armed forces among men
in a Canadian census cohort.
Am
J Ind Med, 61 (2018), pp. 815-823
Hays, J.; Hunt, J. R.; Hubbell, F. A.; Anderson, G. L.; Limacher, M.; Allen, C.; Rossouw, J. E.
The Women's Health Initiative recruitment methods and results
Ann Epidemiol, 13 (2003), pp. S18-77
Heyer,
N.W., N.; Demers, P.; Rosenstock, L.
Cohort
mortality study of Seattle fire fighters: 1945-1983.
Am J Ind Med, 17 (1990), pp. 493-504
Hoppe-Jones,
C.B., S.; Burgess, J.; Snyder, S.; Flahr, L.; Griffin, S.
Use
of urinary biomarkers and bioassays to evaluate chemical exposure and
activation of cancer pathways in firefighters.
Occup
Environ Med, 75 (2018), pp. 412-413
Howlader,
N.N., A.; Krapcho, M.; Miller, D.; Brest, A.; Yu, M.; Ruhl, J.;
Tatalovich, Z.; Mariotto, A.; Lewis, D.; Chen, H.; Feuer, E.;
Cronin
K. SEER Cancer Statistics Review, 1975-2016.
Bethesda, MD: National Cancer Institute (2019)
IARC.
Painting,
Firefighting, and Shiftwork. IARC Monographs on the Evaluation of
Carcinogenic Risks to Humans Vol 98.
Lyon,
France: World Health Organization (2010)
IARC.
IARC
Working Group on the Evaluation of Carcinogenic Risks to Humans.
Personal habits and indoor combustions. Volume 100 E.
A review of human carcinogens ed (2012)
IARC.
Advisory
Group recommendations on priorities for the IARC Monographs.
Lancet
Oncol, 20 (2019), pp. 763-764
IARC.
IARC Monographs on the Identification of Carcinogenic Hazards to Humans: Agents classified by the IARC Monographs, Volumes 1–127. https://monographs.iarc.fr/list-of-classifications. (2020)
Jalilian,
H.Z., M.; Weiderpass, E.; Rueegg, C.; Khosravi, Y.; Kjaerheim, K.
Cancer
incidence and mortality among firefighters.
Int
J Cancer, 145 (2019), pp. 2639-2646
Jankovic,
J.; Jones, W.; Burkhart, J.; Noonan, G.
Environmental
study of firefighters.
Ann
Occup Hyg, 35 (1991), pp. 581-602
Jeong,
K.S.Z., J.; Griffin, S.; Jacobs, E.; Dearmon-Moore, D.; Zhai, J.; et
al.
MicroRNA
Changes in Firefighters.
J
Occup Environ Med, 60 (2018), pp. 469-474
Keir,
J.L.A.; Akhtar, U.S.; Matschke, D.M.J.; Kirkham, T.L.; Chan, H.M.;
Ayotte, P.; White, P.A.; Blais, J.M.
Elevated
Exposures to Polycyclic Aromatic Hydrocarbons and Other Organic
Mutagens in Ottawa Firefighters Participating in Emergency, On-Shift
Fire Suppression.
Environ
Sci Technol, 51 (2017), pp. 12745-12755
Kirk,
K.M.; Logan, M.B.
Structural
Fire Fighting Ensembles: Accumulation and Off-gassing of Combustion
Products.
J Occup Environ Hyg, 12 (2015), pp. 376-383
Lee, D. J., Koru-Sengul, T., Hernandez, M. N., Caban-Martinez, A. J., McClure, L. A., Mackinnon, J. A., & Kobetz, E. N. (2020). Cancer risk among career male and female Florida firefighters: Evidence from the Florida Firefighter Cancer Registry (1981-2014). American Journal of Industrial Medicine, (2020).
LeMasters,
G.K.; Genaidy, A.M.; Succop, P.; Deddens, J.; Sobeih, T.;
Barriera-Viruet, H.; Dunning, K.; Lockey, J. Cancer
risk among firefighters: a review and meta-analysis of 32 studies.
J Occup Environ Med, 48 (2006), pp. 1189-1202
Lewis,
S.B., H.; Faith, M.
Cancer
mortality among Los Angeles city firefighters.
Beverly
Hills, CA: Institute for Cancer and Blood Research (1982)
McClure, L.; Koru-Sengul, T.; Hernandez, MN.; Mackinnon, J.; Schaefer-Solle, N.; Caban-Martinez, A.; Lee, D.; Kobetz, E. Availability and accuracy of occupation in cancer registry data among Florida firefighters. Plos One, 14 (2019)
Muegge, C.M.; Zollinger, T.; Song, Y.; Wessel, J.; Monahan, P.; Moffatt, S.
Excess mortality among Indiana firefighters, 1985-2013
Am J Ind Med. 61 (2018); pp.961-967
Musk,
A.W.; Monson, R.R.; Peters, J.M.; Peters, R.K.
Mortality
among Boston firefighters, 1915--1975.
Br J Ind Med, 35 (1978), pp. 104-108
Naimi, A. I., Richardson, D. B., & Cole, S. R. Causal inference in occupational epidemiology: accounting for the healthy worker effect by using structural nested models. American Journal of Epidemiology, 178 (2013), pp. 1681-1686.
Navarro, K.K., M.; Mackay, C.; Reinhardt, T.; Balmes, J.; Broyles, G.; Ottmar, R.; Naher, L.; Domitrovich, J. Wildland firefighter smoke exposure and risk of lung cancer and cardiovascular disease mortality. Environ Res, (2019), pp. 462-468
NFPA.
U.S.
Fire Department Profile (2018)
Oliveira,
M.D.-M., C.; Morais, S.; Slezakova, K.; Pereira, MC.; Fernandes, A.
Levels
of urinary biomarkers of exposure and potential genotoxic risks in
firefighters.
Occupational Safety and Hygiene VI - Selected contributions
from the International Symposium Occupational Safety and Hygiene
2018;
Petersen,
K.P., J.; Bonde, J.; Ebbehoej, N.; Hansen, J.
Long-term
follow-up for cancer incidence in a cohort of Danish firefighters.
Occup Environ Med, 75 (2018a), pp. 263-269
Petersen,
K.P., J.; Bonde, J.; Ebbehøj, N.; Hansen J.
Mortality
in a cohort of Danish firefighters; 1970-2014.
Int Arch Occup Environ Health, 91 (2018b), pp. 759-766
Pinkerton, L.; Bertke, S.; Yiin, J.; Dahm, M.; Kubales, T.; Hales, T.; Purdue, M.; Beaumont, J.; Daniels, R. Mortality in a cohort of US firefighters from San Francisco, Chicago and Philadelphia: an update Occup Enviorn Med (2020)
Pukkala,
E.M., J.; Weiderpass, E.; Kjaerheim, K.; Lynge, E.; Tryggvadottir,
L.; Sparén, P.; Demers P.
Cancer
incidence among firefighters: 45 years of follow-up in five Nordic
countries.
Occup
Environ Med, 71 (2014), pp. 398-404
Schottenfeld,
D.F., J.
Cancer
epidemiology and prevention eds.
New
York, New York (2006)
Soteriades, E.S; Kim, J.; Christophi, C.; Kales, S.
Cancer Incidence and Mortality in Firefighters: A State-of-the-Art Review and Meta-Analysis. Asian Pac J Cancer Prev, 20 (2019), pp.3221-3231
Sritharan,
J.P., M.; Demers, P.; Harris, S.; Cole, D.; Parent, M.
Prostate
cancer in firefighting and police work: a systematic review and
meta-analysis of epidemiologic studies.
Environ
Health, 16 (2017), pp. 124
Stec,
A.A.; Dickens, K.E.; Salden, M.; Hewitt, F.E.; Watts, D.P.;
Houldsworth, P.E.; Martin, F.L.
Occupational
Exposure to Polycyclic Aromatic Hydrocarbons and Elevated Cancer
Incidence in Firefighters.
Sci
Rep, 8 (2018), pp. 2476
Tornling,
G.G., P.; Hogstedt, C.
Mortality
and cancer incidence in Stockholm fire fighters.
Am
J Ind Med, 25 (1994), pp. 219-228
Tsai,
R.J.; Luckhaupt, S.E.; Schumacher, P.; Cress, R.D.; Deapen, D.M.;
Calvert, G.M.
Risk
of cancer among firefighters in California, 1988-2007.
Am
J Ind Med, 58 (2015), pp. 715-729
Vena,
J.F., R.
Mortality
of a municipal-worker cohort: IV. Fire fighters.
Am
J Ind Med, 11 (1987), pp. 671-684
Wiencke,
J.
Impact
of race/ethnicity on molecular pathways in human cancer.
Nat Rev Cancer, 4 (2004), pp. 79-84
The Women's Health Initiative Study Group
Design of the Women's Health Initiative clinical trial and observational study. The Women's Health Initiative Study Group
Control Clin Trials, 19 (1998), pp. 61-109
Zahm,
S.F., J.
Racial,
ethnic, and gender variations in cancer risk: considerations for
future epidemiologic research.
Environ Health Perspect, 103 (1995), pp. 283-286
Zhou,
J.; Jenkins, T.G.; Jung, A.M.; Jeong, K.Y.; Zhai, J.; Jacobs, E.T.;
Griffin, S.C.; Dearmon-Moore, D.; Littau, S.R.; Peate, W.F.; Ellis,
N.A.; Lance, P.; Chen, Y.; Burgess, J.L.
DNA
methylation among firefighters.
PLOS One, 14(3) (2019), e0214282
ADDENDICES
Appendix A – NFR Design Flowcharts
Appendix B – NFR Promotional Campaign
Appendix C – List of Stakeholders
Appendix D – Informed Consent Document
Appendix E – User Profile Questions
Appendix F – Enrollment Questionnaire
Appendix G – Assurance of Confidentiality
Appendix A – NFR Design Flowcharts
A.1. Participant Population Recruitment (Overall, Targeted Cohort, and Open Cohort)
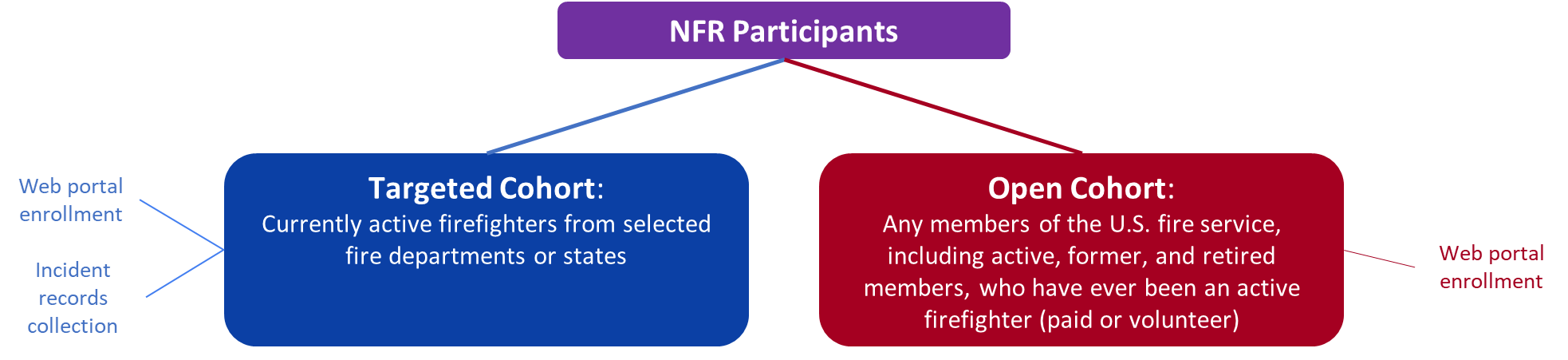
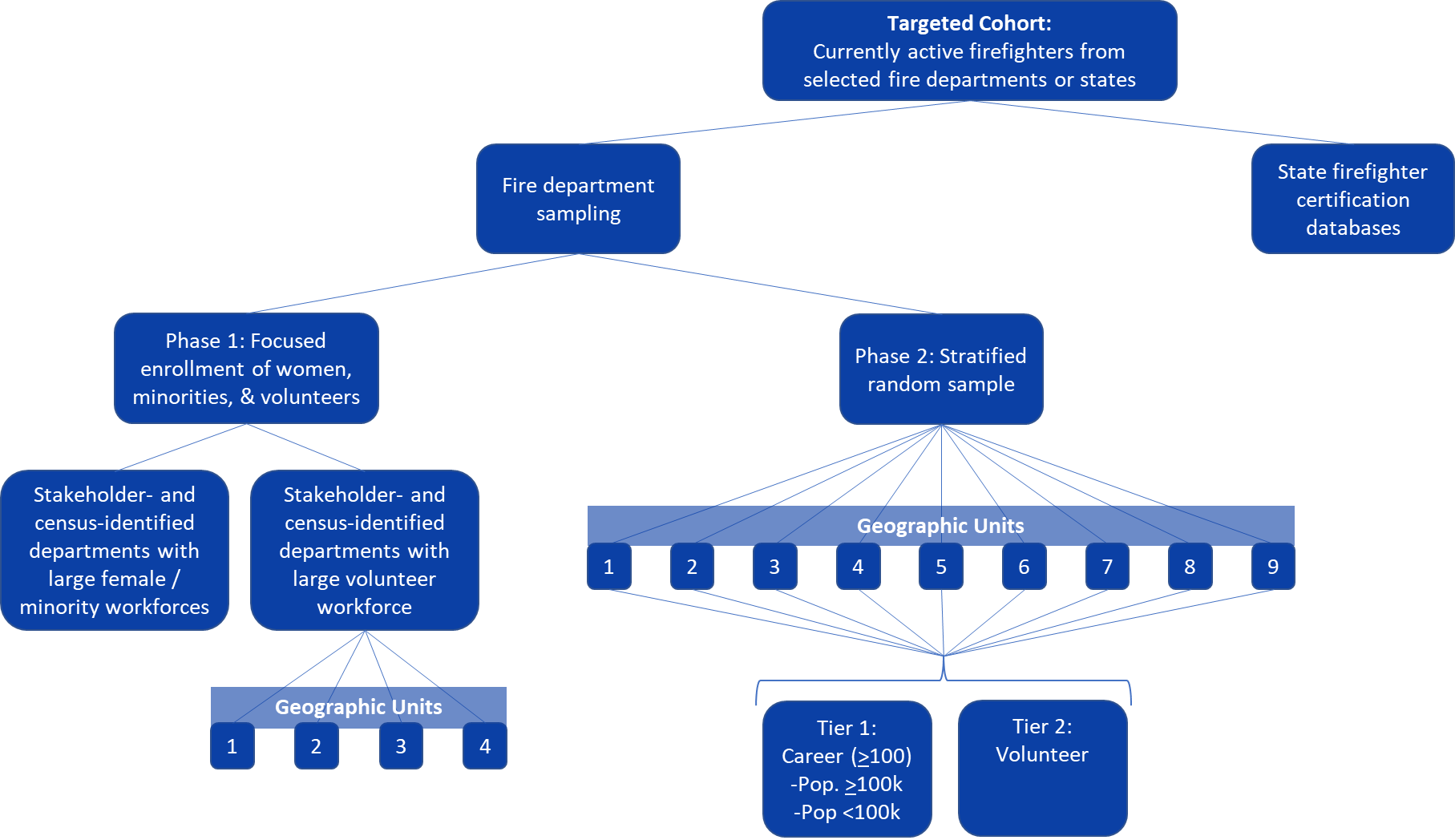
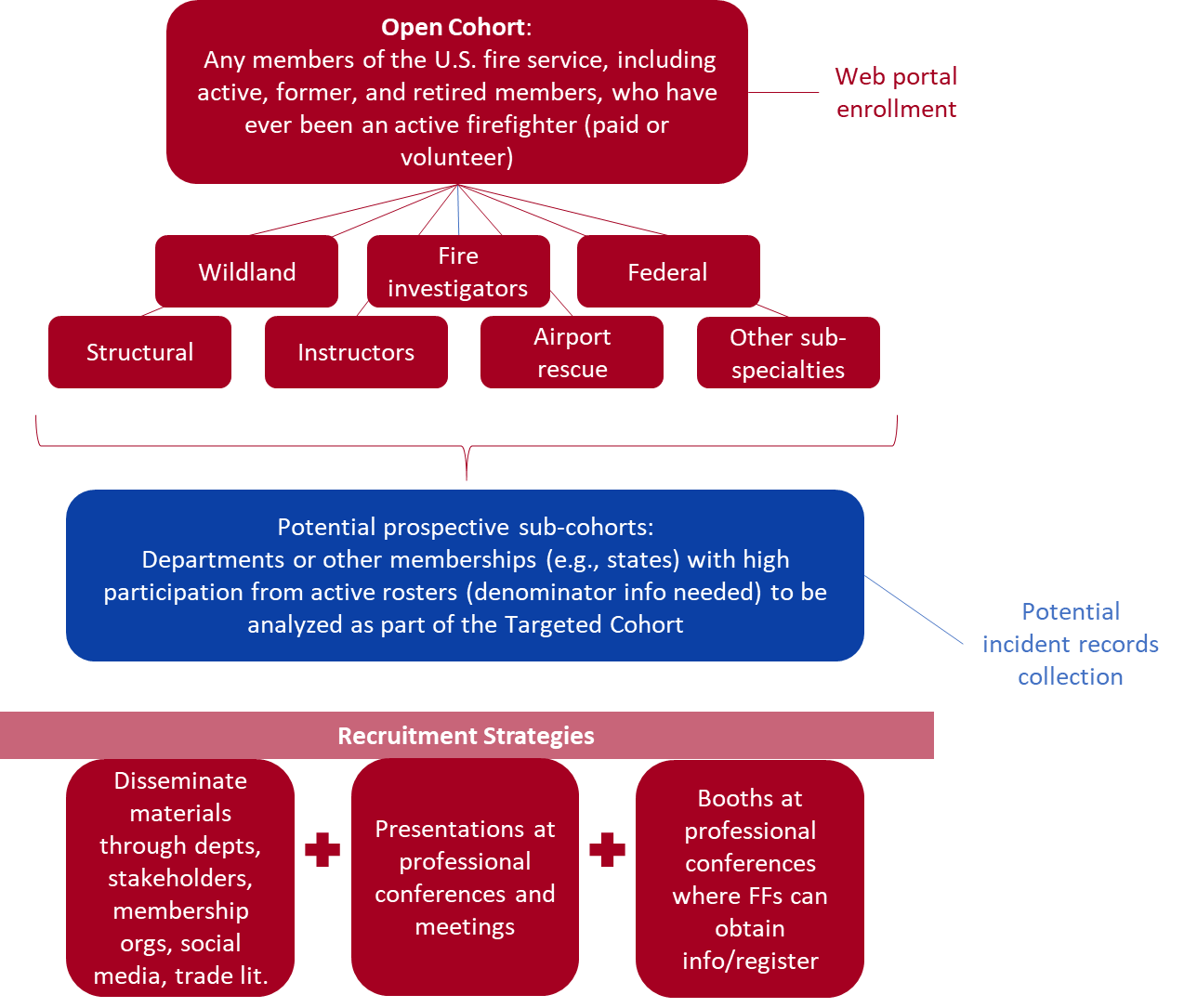
A.2. Enrollment Process
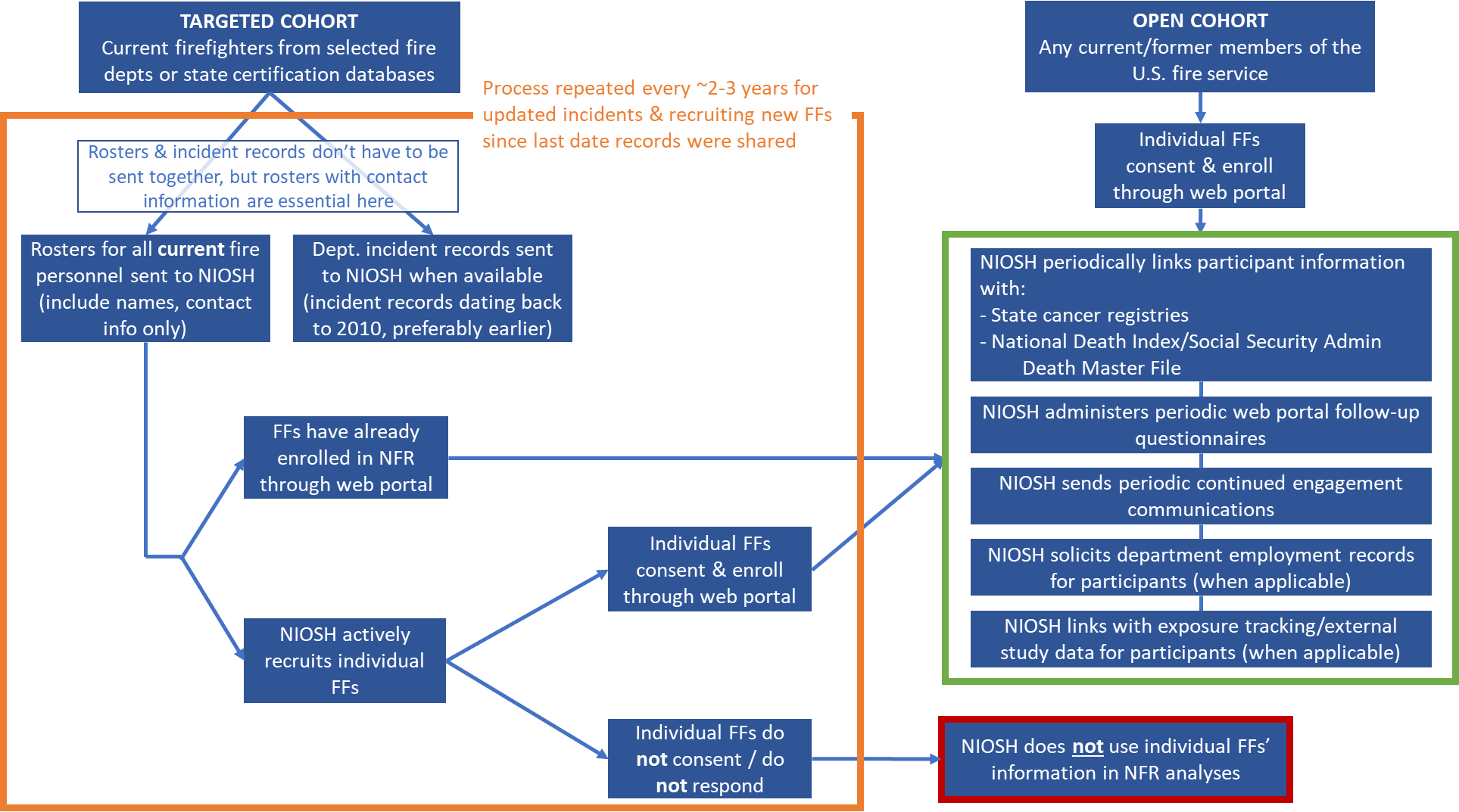
Appendix B – NFR Promotional Campaign*
*Previously cleared by DFSE 7/2/2020, this promotional brochure is pending final design, which will be updated to reflect the NFR’s new logo and color scheme.

Appendix C – Self-Identified List of Stakeholders*
*This is a list of organizations that participated in conversations with NIOSH or were otherwise involved in planning during the development of the NFR and is not meant to be an exhaustive list of all related stakeholders. This list will be updated periodically by NIOSH as the NFR progresses and new partnerships are established.
Organization |
Boston Fire Department |
Bureau of Indian Affairs |
Cal Fire |
California Department of Public Health |
Cancer Institute and Infusion Center |
Chicago Fire Department |
Commonweal Biomonitoring Resource Center |
Congressional Fire Services Institute |
Fire Department Instructors Conference |
Fire Department of New York (FDNY) |
Firefighter Cancer Support Network |
Firehouse Magazine |
First Responder Center for Excellence for Reducing Occupational Illness, Injuries and Deaths, Inc. |
Idaho Cancer Registry |
Illinois Fire Service Institute |
International Association of Black Professional Fire Fighters |
International Association of Fire Chiefs |
International Association of Fire Fighters |
International Association of Fire Fighters Wildfire Division |
International Association of Wildland Fire |
International Association of Women in Fire & Emergency Services (Women in Fire) |
Johns Hopkins University Bloomberg School of Public Health |
Lebanon Fire District |
Loveland-Symmes Fire Department |
National Association of Hispanic Firefighters |
National Fallen Firefighter Foundation |
National Fire Protection Association |
National Volunteer Fire Council |
Nebraska Department of Health and Human Services |
New York State Fire Prevention and Control |
North American Association of Central Cancer Registries |
Oakland Fire Department |
Portsmouth, New Hampshire Office of the Mayor |
Rutgers School of Public Health |
San Antonio Fire Department |
Skidmore College |
Tucson Fire Department |
Underwriters Laboratories (UL) Firefighter Safety Research Institute |
United States Department of Interior |
United States Fire Administration |
United States Forest Service |
University of Arizona |
University of Miami |
University of Southern California |
Wildfire Today |
Yale School of Public Health |
|
| File Type | application/vnd.openxmlformats-officedocument.wordprocessingml.document |
| Author | Siegel, Miriam (CDC/NIOSH/DFSE/FRB) |
| File Modified | 0000-00-00 |
| File Created | 2021-01-13 |
© 2026 OMB.report | Privacy Policy