Narrative Instructions_ MCH Block Grant Guidance _10_26_2020-FINAL
Narrative Instructions_ MCH Block Grant Guidance _10_26_2020-FINAL.docx
Maternal and Child Health Services Block Grant Application/Annual Report Guidance
Narrative Instructions_ MCH Block Grant Guidance _10_26_2020-FINAL
OMB: 0915-0172


TITLE V MATERNAL AND CHILD HEALTH SERVICES BLOCK GRANT TO STATES PROGRAM
GUIDANCE AND FORMS FOR THE
TITLE V APPLICATION/ANNUAL REPORT
OMB NO: _________
EXPIRES: __________
U.S. Department of Health and Human Services
Health Resources and Services Administration
Maternal and Child Health Bureau
Division of State and Community Health
5600 Fishers Lane, Room 18N33
Rockville, MD 20857
(Phone 301-443-2204 FAX 301-443-9354)

Public
Burden Statement: An agency may not conduct or sponsor, and a person
is not required to respond to, a collection of information unless it
displays a currently valid OMB control number. The OMB control
number for this project is XXXX-XXXX. Public reporting burden for
this collection of information is estimated to average 120 hours per
response, including the time for reviewing instructions, searching
existing data sources, and completing and reviewing the collection
of information. Send comments regarding this burden estimate or any
other aspect of this collection of information, including
suggestions for reducing this burden, to HRSA Reports Clearance
Officer, 5600 Fishers Lane, Room 14N39, Rockville, Maryland, 20857.
TITLE V MATERNAL AND CHILD HEALTH (MCH) SERVICES BLOCK GRANT TO STATES PROGRAM APPLICATION/ANNUAL REPORT GUIDANCE
NINTH EDITION
The Title V Maternal and Child Health (MCH) Services Block Grant to States Program (hereafter referred to as the MCH Block Grant) is a formula grant under which funds are awarded to 59 states and jurisdictions upon their submission of an acceptable plan that addresses the health services needs within a state for the target population of mothers, infants and children, which includes infants and children with special health care needs (CSHCN), and their families. As referenced in this Guidance, the population of CSHCN is inclusive of children and youth, ages one through 21 years. Through the MCH Block Grant, each state and jurisdiction supports and promotes the development and coordination of systems of care for the MCH population, which are family-centered, community-based and culturally appropriate.
The Application/Annual Report Guidance is used by the 50 states and nine jurisdictions in applying for their MCH Block Grants under Title V of the Social Security Act and in preparing the required Annual Report. States/jurisdictions report annually on national and state outcome/performance measures, which document their progress towards the achievement of established performance targets, ensure accountability for the ongoing monitoring of health status in women and children and lend support to the delivery of an effective public health system for the nation’s MCH population. Complementary to the reporting of outcome and performance measure data is the narrative description of the state/jurisdiction’s Title V program activities.
The ninth edition of the Title V Maternal and Child Health Services Block Grant to States Program Guidance consists of two documents: 1) Instructions to the states on completing the required Application/Annual Report and Reporting Forms; and 2) Appendix of Supporting Documents, which includes background program information and other technical resources. As with previous editions, this Guidance adheres to the specific statutory requirements outlined in Sections 501-509 of the Title V legislation and honors the rights of states to determine their individual MCH program priorities, to develop tailored strategies for addressing their unique MCH population needs and to assume accountability in achieving measurable progress towards stated program goals.
This edition of the Title V MCH Services Block Grant to States Program Guidance builds on and further refines the reporting structure and vision that was outlined in the previous edition. While retaining the organizational structure, performance measure framework, definition of family partnership and focus on the implementation of evidence-based or -informed strategies and measures, this edition recognizes the important role that State Title V programs play in providing leadership and infrastructural support to assure the delivery of gap-filling direct services, enabling services and public health services and systems for the MCH population. Greater emphasis is placed on capacity building and assessment related to the development of robust MCH data systems, a skilled and well-trained MCH workforce, and emergency preparedness planning that responds to MCH population needs.
States apply annually for MCH Block Grant funding using the online Title V Information System (TVIS). Administered by the Health Resources and Services Administration’s (HRSA) Maternal and Child Health Bureau (MCHB), the TVIS consists of two components: 1) MCH Block Grant Application/Annual Report Data Entry (used by state/jurisdictional MCH Block Grantees to submit their financial, program, and performance data); and 2) TVIS Reports (a Web-based interface that allows public users to generate reports from Title V data). Since its development in 2002, TVIS has contributed to numerous efficiencies in the Application/Annual Report submission process. Examples include the automatic calculations of ratios, rates, and percentages; capturing of past years’ narrative and data reporting; and assurance that the data presented in multiple tables are entered only once by the state. The TVIS Web Reports further contribute to program transparency and accountability in making the financial, program and performance data submitted by the 59 State MCH Block Grantees publicly available in a searchable database.
Questions and comments regarding this edition of the Application/Annual Report Guidance may be addressed to:
Michele H. Lawler, M.S., R.D.
Director, Division of State and Community Health
Maternal and Child Health Bureau
Health Resources and Services Administration
5600 Fishers Lane, Room 18N33
Rockville, Maryland 20857
Telephone: (301) 443-2204
Fax: (301) 443-9354
TABLE of CONTENTS
PART ONE: BACKGROUND AND ADMINISTRATIVE INFORMATION 1
Purpose of the Maternal and Child Health (MCH) Block Grant 1
Background and Brief History 2
Guiding Principles for the Development of the MCH Block Grant 2 Application/Annual Report Guidance
Public Health Services Systems Model for MCH Populations 3
Data Driven Programming and Performance Accountability 4 (National Performance Measure Framework)
Family Partnership 8
Legislative Requirements 9
Who Can Apply for Funds [Section 505(a)] 10
Use of Allotment Funds [Section 504]) 10
Application for Block Grant Funds [Section 505] 10
Annual Report [Section 506] 11
Administration of Federal and State Programs [Section 509] 12
PART TWO: APPLICATION/ANNUAL REPORT INSTRUCTIONS 13
General Requirements 13
Letter of Transmittal 13
Face Sheet 13
Assurances and Certifications 13
Table of Contents 13
Logic Model 13
Components of the Application/Annual Report 15
Executive Summary 16
Program Overview 16
How Federal Title V Funds Complement State-Supported 17
MCH Efforts
MCH Success Story 18
Overview of the State 18
Needs Assessment 19
Needs Assessment Update 19
Five-Year Needs Assessment Summary 20
Process Description 21
Findings 22
MCH Population Health Status 22
Title V Program Capacity 23
Title V Program Partnerships, Collaboration, 25
and Coordination
Identifying Priority Needs and Linking to Performance 26 Measures
D. Financial Narrative 27
Expenditures 27
Budget 28
Five-Year State Action Plan 29
Five-Year State Action Plan Table 30
State Action Plan Narrative Overview 31
State Title V Program Purpose and Design 31
State MCH Capacity to Advance Effective Public 32
Health Systems
MCH Workforce Development 32
Family Partnership 34
MCH Data Capacity 35
MCH Emergency Planning and Preparedness 38
Health Care Delivery System 39
State Action Plan Narrative by Domain 41
Public Input [Section 505(a)] 43
Technical Assistance 44
PART THREE: REPORTING FORMS 45
PART ONE: BACKGROUND AND ADMINISTRATIVE INFORMATION
Purpose of the Maternal and Child Health (MCH) Block Grant
As defined in section 501(a)(1) of the Title V legislation, the purpose of the MCH Block Grant is to enable each state:
To provide and to assure mothers and children (in particular those with low income or with limited availability of health services) access to quality MCH services;
To reduce infant mortality and the incidence of preventable diseases and handicapping conditions among children, to reduce the need for inpatient and long-term care services, to increase the number of children (especially preschool children) appropriately immunized against disease and the number of low income children receiving health assessments and follow-up diagnostic and treatment services, and otherwise to promote the health of mothers and infants by providing prenatal, delivery, and postpartum care for low income, at-risk pregnant women, and to promote the health of children by providing preventive and primary care services for low income children;
To provide rehabilitation services for blind and disabled individuals under the age of 16 receiving benefits under title XVI, to the extent medical assistance for such services is not provided under title XIX; and
To provide and to promote family-centered, community-based, coordinated care (including care coordination services, as defined in subsection (b)(3)) for children with special health care needs (CSHCN) and to facilitate the development of community-based systems of services for such children and their families.
This legislative purpose is further affirmed through the Title V Vision and Mission statements, as shown below.
Vision of Title V
Title V envisions a nation where all mothers, infants, children aged 1 through 21 years, including CSHCN, and their families are healthy and thriving.
Mission of Title V
The Mission of Title V is to improve the health and well-being of the nation’s mothers, infants, children and youth, including children and youth with special health care needs, and their families.
Background and Brief History
Since its original authorization in 1935, Title V of the Social Security Act has been amended several times to reflect an ongoing commitment to improving the health and well-being of our Nation's mothers, children and their families. Block-granted in 1981, with new accountability requirements added in 1989, Title V has remained a vitally important public health program for serving the MCH population. In 2015, an updated performance measure framework was introduced to reflect more clearly the contributions of Title V in improving health outcomes among the MCH population. A more complete history of Title V can be found in Appendix A of the Supporting Documents to the Title V MCH Block Grant Application/Annual Report Guidance.
The MCH Block Grant is a formula grant under which funds are awarded to 59 states and jurisdictions upon the submission of an acceptable plan that addresses the health services needs within a state for the target population of mothers, infants and children, including CSHCN. Through this process, each state and jurisdiction supports and promotes the development and coordination of systems of care for the MCH population.
Annual submission of an Application is required by law to entitle a state to receive MCH Block Grant funds (Section 505 of Title V of the Social Security Act). Per Section 506, a state is further required to submit an Annual Report on the expenditure of the previous year’s funds. In addition, Section 505(a) requires a state to conduct a comprehensive and statewide needs assessment every five years. The information and instructions for the preparation and submission of the Application/Annual Report and Five-Year Needs Assessment are contained in the Title V Maternal and Child Health Services Block Grant to States Program: Guidance and Forms for the Title V Application/Annual Report (hereafter referred to as the Application/Annual Report Guidance).
III. Guiding Principles for the Development of the MCH Block Grant Application/Annual Report Guidance
The development of the application/reporting structure for this edition of the Application/Annual Report Guidance incorporates key principles that are common to all state Title V programs. These principles are: 1) delivery of Title V services within a public health service model; 2) data-driven programming and performance accountability; and 3) partnerships with individuals/families/family-led organizations (hereafter referred to as family partnership) to ensure systems and services that support the interests of all MCH populations. These principles have contributed to the MCH Block Grants’ success in operationalizing the legislative requirements and in delivering public health services and systems of care that address the needs of the MCH population.
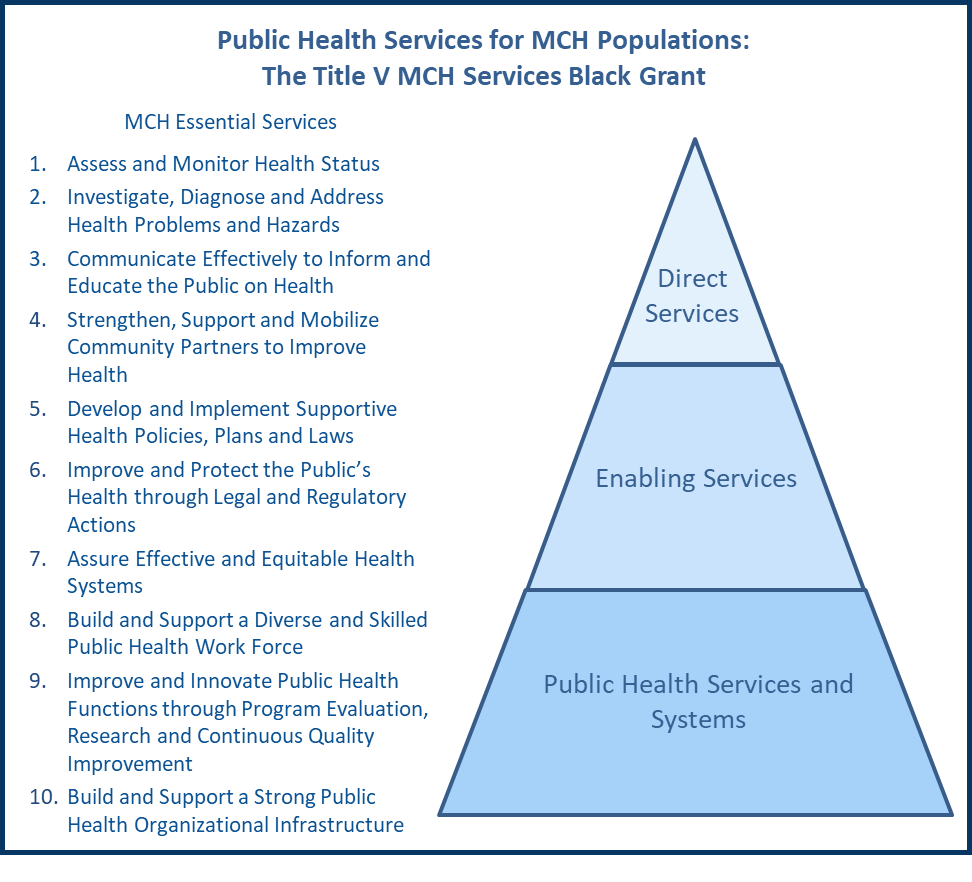
Public Health Services Systems Model for MCH Populations
A 1988 Institute of Medicine (IOM) Report1 defined the core functions of public health as assessment, policy development and assurance. In operationalizing the core public health functions and in ensuring that the unique needs of mothers and children were addressed, the MCH community worked with the Public Health Service and the IOM to identify ten (10) “Essential Public Health Services”2 in 1994. Since that time, the 10 Essential Public Health Services have provided a framework for the delivery of MCH services, as reflected in Figure 1 on the following page.
As part of the Futures Initiative, the Public Health National Center for Innovations (PHNCI) and the de Beaumont Foundation engaged the public health field in a 2020 review and update of the Ten Essential Public Health Services framework to better reflect current and emerging public health practice needs. The revised framework was released on September 9, 2020. More information on this work can be found on the PHNCI website at: https://phnci.org/national-frameworks/10-ephs.
A crosswalk of the 10 Essential Public Health Services with the purpose of the State MCH Block Grants, as defined in Section 501(a)(1) of Title V of the Social Security Act, yielded the following strategies for states to use in their program planning.
Conduct ongoing assessment of the changing health needs of the MCH population to drive priorities for achieving equity in access and positive health outcomes;
Expand surveillance and other data systems capacity to support rapid investigation of emerging health issues that affect the MCH population (e.g., Zika and Neonatal Abstinence Syndrome)
Inform and educate the public and families about the unique needs of the MCH population;
Mobilize partners, including families and individuals, at the federal, state and community levels in promoting shared vision for leveraging resources, integrating and improving MCH systems of care, promoting quality public health services and developing supportive policies;
Provide expertise and support for the formation and implementation of state laws, regulations and other policies pertaining to the health of the MCH population (e.g., perinatal regionalization/risk appropriate care and suicide prevention);
Integrate systems of public health, health care and related community services to ensure equitable access and coordination to achieve maximum impact;
Promote the effective and efficient organization and utilization of resources to ensure access to necessary comprehensive services for CSHCN and families through public health services, systems, and population health efforts.
Educate the MCH workforce to build the capacity to ensure innovative, effective programs and services and the efficient and equitable use of resources;
Support or conduct applied research resulting in evidence-based policies and programs;
Facilitate rapid innovation and dissemination of effective practices through quality improvement and other emerging methods; and
Provide services to address unmet needs in healthcare and public health systems for the MCH population (i.e., gap-filling services for individuals).
Figure 1.
B. Data Driven Programming and Performance Accountability (National Performance Measurement Framework)
The MCH Block Grant utilizes a three-tiered national performance measurement framework (Figure 2), which includes National Outcome Measures (NOMs), National Performance Measures (NPMs) and state-initiated Evidence-based or -informed Strategy Measures (ESMs). The framework provides flexibility to a state in identifying the best combination of measures to address the MCH priority needs that were identified based on the findings of the Five-Year Needs Assessment. A state must select a minimum of 5 NPMS, but states have the flexibility to select as many NPMs and State Performance Measures (SPMs) as necessary to address each of its priority needs. See Appendices B and C for detailed information about the NPM Framework, NOMs and NPMs.
The NPMs are a set of short-term and medium-term performance measures that utilize population-based, state-level data derived from national data sources and for which a state Title V program tracks prevalence rates and works towards demonstrated impact. They are intended to drive improved outcomes relative to one or more medium and long-term indicators of health status or access to quality health care (i.e., NOMs) for the MCH population. Thus, a state tracks the NOMs to monitor the impact of the NPMs.
Figure
2. Performance Measure Framework

National Outcome Measures |
|
National Performance Measures |
|
Evidence-based/Informed Strategy Measures |

Title V is responsible for promoting the health of all mothers and children, including CSHCN and their families. There are 15 NPMs, which address key MCH priority areas within five MCH population domains. These domains are: 1) Women/Maternal Health;
2) Perinatal/Infant Health; 3) Child Health; 4) Adolescent Health; and 5) CSHCN. The NPM framework also applies the life course theory, which identifies critical stages (i.e., beginning before a child is born and continuing throughout life) that can influence lifelong health and well-being.
A sixth domain addresses Cross-cutting and Systems Building needs. While there are currently no NPMs included in this last domain, a state may choose to develop one or more SPMs to address a priority need that is related to program capacity and/or systems-building (e.g., applies to all MCH population domains). A state is not required to identify a measure for this domain. If a SPM is developed, the state should define strategies for determining success. Examples of topics addressed by SPMs in this domain are:
Partnerships with individuals, families, and family-led organizations ;
Social determinants of health;
Health Equity;
Workforce development; and
Enhanced data infrastructure
An overview of the NPMs, by MCH population health domain, is displayed in Table 1.
It should be noted that the five MCH population health domains reflected in the NPM framework are contained within the three legislatively-defined MCH populations [Section 505(a)(1)]. For example, the first two domains are included under “preventive and primary care services for pregnant women, mothers and infants up to age one,” which is the first of the three defined MCH populations. Child and adolescent health are included in the second defined MCH population, specifically “preventive and primary care services for children.” CSHCN is the third legislatively defined MCH population. This latter population is inclusive of children and youth with special health care needs.
Table 1: NPMs and Domains
NPM # |
MCH Population Domains |
Cross-cutting/ Systems Building Domain Optional |
|||||
Women/Maternal Health |
Perinatal/ Infant Health |
Child Health |
Adolescent Health |
Children with Special Health Care Needs |
|||
1 |
Well-woman visit |
|
|
|
|
|
States have the option to develop a state performance measure (SPM) that is Cross-cutting/Systems Building. Examples of measure topic areas include but are not limited to:
|
2 |
Low-risk cesarean delivery |
|
|
|
|
|
|
3 |
Risk-appropriate perinatal care |
|
|
|
|
|
|
4 |
Breastfeeding++ |
|
|
|
|
|
|
5 |
Safe sleep++ |
|
|
|
|
|
|
6 |
Developmental screening |
|
|
|
|
|
|
7 |
Injury hospitalization* |
|
|
|
|
|
|
8 |
Physical activity * |
|
|
|
|
|
|
9 |
Bullying |
|
|
|
|
|
|
10 |
Adolescent well-visit |
|
|
|
|
|
|
11 |
Medical home* |
|
|
|
|
|
|
12 |
Transition* |
|
|
|
|
|
|
13 |
Preventive dental visit *++ |
|
|
|
|
|
|
14 |
Smoking *++ |
|
|
|
|
|
|
15 |
Adequate insurance * |
|
|
|
|
|
|
* NPM with multiple domains (Note: States may choose to target children and adolescents without special health care needs, in addition to children and adolescents with special health care needs for NPM #11 and NPM #12.)
++ NPMs that have multiple sub-measures (e.g., have an “A” and “B” component)
The 15 NPMs remain the same as in the eighth edition of the MCH Block Grant Application/Annual Report Guidance, being distributed within the five population health domains. As noted above, a state must choose a minimum of five (5) NPMs. At least one NPM must be selected for each of the five (5) MCH population domains, but a state may opt to select additional NPMs based on its identified priority needs. There is no maximum for the number of NPMs that a state can select.
States should note that the same measure selected in multiple domains (NPM #7, NPM #8, NPM #11, NPM #12, NPM #13, NPM #14 and NPM #15) will only count once toward the minimum of five (5) NPMs. For example, if a state selects NPM #14 in both the Women/Maternal Health Domain and the Child Health Domain, this measure would only count once towards the required minimum of five NPMs. The state would need to select another measure in either the Women/Maternal Health Domain or the Child Health Domain to satisfy the requirement of one NPM per population domain. NPM #11 (medical home) and/or NPM #12 (transition) are core performance measures for achieving desired systems of services for CSHCN. As such, a state that selects NPM #11 and/or NPM #12 must address children with special health care needs (i.e., CSHCN domain). States may choose to also reflect NPM #11 in either the Child Health Domain or the Adolescent Health Domain or to reflect NPM #12 in the Adolescent Health Domain. The four scenarios presented in Figure 3 on the following page provide further explanation regarding the available options to a state in the selection of NPMs to meet the minimum requirements.
Figure 3. Scenarios for Assuring Selection of NPMs Across Domains
Scenario
4:
A state selects NPM #15 for the Adolescent Health Domain and the
CSHCN Domain. While the measure targets different population
groups, NPM #15 counts as only one measure. The state may choose to
count this measure as the selected NPM in either the Adolescent
Health Domain or the CSHCN Domain. The state must choose a
different NPM for the second domain.
Scenario
1:
A state selects NPM #7 for both the Child Health Domain and the
Adolescent Health Domain. In selecting a NPM for each of the five
population domains, as required, the state can choose to count NPM
#7 as the selected measure in either of the two domains. The state
must then select a second NPM for the other domain.
Scenario
2:
A state selects NPM #11 for the Child Health Domain, which is an
optional target population. In selecting this measure, the state
must also address the CSHCN Domain. The state may choose to count
this measure in either the CSHCN Domain or the Child Health Domain.
If selected as the NPM for the Child Health Domain, the state must
select a second NPM from the CSHCN Domain.
Scenario
3: A
state selects NPM #13.1 for the Women/Maternal Health Domain and NPM
#13.2 for the Child Health Domain. While the measure targets
different population groups, NPM #13 counts as only one measure.
The state can choose to select this measure for either of the two
domains. The state will need to select a different NPM for the
second domain. A state can select NPM #13.1 without selecting NPM
#13.2, or vice versa.
C. Family Partnership
Building the capacity of women and children, including CSHCN, and their families to partner in decision-making with Title V programs at federal, state and community levels is a critical strategy in helping states to achieve the identified MCH priorities. Title V’s commitment to these partnerships are strong, as states expand and strengthen family engagement activities in all MCH population domains.
Traditionally, state Title V programs have partnered with families in a variety of program activities. Specific examples include:
Contracting with Family-Led Organizations;
Paid Program Staff;
Advisory Committees/Task Forces;
Agency Decision-Making and Policy Development;
Program Outreach;
Training; and
Peer Support.
For purposes of the MCH Block Grant, family partnership is defined as, “patients, families, their representatives, and health professionals working in active partnership at various levels across the health care system – direct care, organizational design and governance, and policy making—to improve health and health care.3 This partnership is accomplished through the intentional practice of working with families for the ultimate goal of positive outcomes in all areas through the life course.”4 Relevant resources include, but are not limited to, the National Consensus Standards for Systems of Care for Children and Youth with Special Health Care Needs, authored by the Association of Maternal and Child Health Programs (AMCHP, 2014); a series of reports and case studies entitled, Sustaining and Diversifying Family Engagement in Title V MCH and CYSHCN Programs (AMCHP, 2016); and the Family Engagement in Systems Assessment Tool (FESAT) and Family Engagement in Systems (FES) Toolkit developed and released by Family Voices in 2019/2020 . See Appendix D for more information.
This edition of the Application/Annual Report Guidance emphasizes the need for a state to demonstrate the value of family partnerships in improving health outcomes across all sectors of the MCH population. In addition, a state should:
Assure families and individuals are key partners in health care decision-making at all levels across the health care system and the services that support them, especially those who are vulnerable and medically underserved;
Provide training, both in orientation and ongoing professional development, for program staff, family leaders, volunteers, contractors and subcontractors in the areas of unconscious bias and cultural/linguistic competence; and
Collaborate with community leaders/organizations and families of every background in needs/assets assessments, program planning, service delivery and valuation/monitoring/quality improvement activities.
Appendix D includes additional information to assist a state in strengthening the family partnership and leadership within its Title V program.
The MCH Block Grant is authorized under Title V of the Social Security Act, which is the longest-standing public health legislation in American history. More than 85 years later, the law continues to support efforts to improve the health of the nation’s women and children. The law can be viewed at: https://www.ssa.gov/OP_Home/ssact/title05/0500.htm . A general overview of the legislative requirements and the way in which these requirements are implemented by MCHB is set out below.
The Application/Annual Report shall be developed by, or in consultation with, the state MCH agency and shall be made public within the state in such manner as to facilitate comment from any person (including any federal or other public agency) during its development and after its transmittal.
Use of Allotment Funds [Section 504]
The state may use its MCH Block Grant funds for the provision of health services and related activities (including planning, administration, education, and evaluation) consistent with its Application. In addition, the state may request supplemental funds from the MCHB to support identified technical assistance needs. Related to technical assistance, the state should plan for and allot funds for the MCH and CSHCN Directors to attend two required meetings each year in person. One of these meetings is the required MCH Block Grant Application/Annual Report review, which is held at a site designated annually by the Division of State and Community Health (DSCH) in HRSA’s MCHB. The other meeting is a MCH Federal-State Partnership Meeting, which aims to: 1) update State MCH and CSHCN Directors on relevant legislation and MCHB initiatives; 2) convene leaders, disseminate best practices and share innovations in the field of MCH; and 3) provide opportunities for information exchange, networking, and collaboration among states and with MCHB. States should plan for this meeting to be held in Washington, DC.
The MCH Block Grant funds may not be used for cash payments to intended recipients of health services or for purchase of land, buildings, or major medical equipment. Other restrictions apply, as specified in Section 504(b).
Application for MCH Block Grant Funds [Section 505]
Each state is required to conduct a statewide Needs Assessment once every five years. A detailed overview of the MCH Five-Year comprehensive statewide Needs Assessment process is presented in Appendix E. The Needs Assessment findings will be integrated into that year’s Application/Annual Report as a Five-Year Needs Assessment Summary. During the four interim years of the five-year reporting period, a state will submit an annual update of its ongoing needs assessment activities and findings in the appropriate section of the state Application/Annual Report. By law, the Application/Annual Report will contain information that is consistent with the health status goals and national health objectives regarding the need for:
Preventive and primary care services for all pregnant women, mothers, and infants up to age one;
Preventive and primary care services for children; and
Services for CSHCN [as specified in section 501(a)(1)(D) "family-centered, community-based, coordinated care (including care coordination services) for children with special health care needs (CSHCN) and to facilitate the development of community-based systems of services for such children and their families"].
The state will organize its reporting on the three legislatively defined MCH populations in the context of five population health domains: 1) Women/Maternal Health;
2) Perinatal/Infant Health; 3) Child Health; 4) Adolescent Health; and 5) CSHCN. Although the Application/Annual Report Guidance defines children as ages 1 year through 21 years, a separate Adolescent Health domain is included in the NPM framework due to their unique health needs. Adolescents often require different strategies than the strategies used to address the needs of the broader child health population.
Each year, at least thirty percent (30%) of federal Title V funds must be used for preventive and primary care services for children and at least thirty percent (30%) for services for CSHCN, as specified in Section 505(a)(3). Such services include providing and promoting family-centered, community-based, coordinated care (including care coordination services) for CSHCN and facilitating the development of community-based systems of services for such children and their families. The thirty percent (30%) requirement may be waived as specified in Section 505(b)(1-2). A request for waiver
must be included in the Application letter of transmittal. In addition, of the amount paid to a state under Section 503 from an allotment for a fiscal year under
Section 502(c), not more than ten percent (10%) may be used for administering the funds paid under this section. [Section 504(d)].
The state must maintain the level of funds being provided solely by such state’s MCH programs at the level provided in fiscal year 1989. [Section 505(a)(4)].
Other requirements for allocation of funds, charging for services, maintenance of a toll-free hotline, and coordination of services with other programs are found in Section 505.
Annual Report [Section 506]
An Annual Report must be submitted to the MCHB each year in order to evaluate and compare the performance of different states assisted under Title V and to assure the proper expenditure of funds. The Annual Report will include a description of program activities, a complete record of the purposes for which funds were spent, the extent to which the state has met its goals and performance objectives, as well as the national health objectives, and the extent to which funds were expended consistent with the state's Application. The Action Plan includes the Annual Report narrative on the state’s Title V program strategies and activities. States will utilize the Action Plan section of the Application/Annual Report to provide narrative discussion on the progress (by population health domain) achieved during the reporting year relative to the implementation of planned activities and gains in meeting the established performance measure targets. The standardized format of the Annual Report, as described, will allow for consistency in reporting and will facilitate the preparation of a report to Congress [Section 506(a)(3)].
As required in Section 509(a)(5), the MCHB has made a substantial effort to not duplicate other federal data collection efforts. The MCHB will collect and provide National Outcome and Performance measure data, as well as Other State Data (OSD), for the individual states, as available. Given that limited data are available from the National Center for Health Statistics (NCHS) and other federal sources for Puerto Rico, Guam, the Republic of the Marshall Islands, Federated States of Micronesia, Republic of Palau, Commonwealth of the Northern Mariana Islands, American Samoa and Virgin Islands, HRSA’s MCHB developed an MCH Jurisdictional Survey. The first round of data was collected in the eight jurisdictions between May 2019 and January 2020, which enabled jurisdictions to utilize survey data for the first time in reporting on selected National Performance and Outcome measures in their FY 2021 MCH Block Grant Applications/FY 2019 Annual Reports. Similar to the National Survey of Children’s Health (NSCH), the MCH Jurisdictional Survey collects information on factors related to the well-being of children. These factors include health status, visits to health care providers, health care costs, and health insurance coverage. In addition, the MCH Jurisdictional Survey collects information on factors related to the well-being of mothers, such as health risk behaviors, health conditions, and preventive health practices.
Administration of Federal and State Programs [Section 509]
The MCHB in HRSA is the organizational unit responsible for the administration of
Title V. Within the Bureau, DSCH has responsibility for the day-to-day operation of the State MCH Block Grants. Applicants may obtain additional information regarding administrative, technical and program issues concerning the Block Grant Application/Annual Report by contacting:
Division of State and Community Health
Maternal and Child Health Bureau
Health Resources and Services Administration
5600 Fishers Lane, Room 18N33
Rockville, Maryland 20857
Telephone: (301) 443-2204; Fax: (301) 443-9354
Within each state, the state health agency is responsible for the administration (or supervision of the administration) of programs carried out with Title V allotments.
PART TWO: APPLICATION/ANNUAL REPORT INSTRUCTIONS
General Requirements
Letter of Transmittal
An electronic letter of transmittal from the responsible state health agency official must be the first page of the MCH Block Grant Application/Annual Report. The letter must also contain the documentation for waiver of a 30 percent allotment, if the state is so requesting. The letter of transmittal is uploaded in TVIS as an image to Section I.A. of the Application/Annual Report.
Each section of the Application Face Sheet (Standard Form 424) must be completed and submitted electronically along with the rest of the Application/Annual Report.
The appropriate Assurances and Certifications for the State MCH Block Grants, which include Application Form Standard Form (SF)-424B, Assurances for Non-Construction Programs and Certifications for debarment and suspension, drug free work place, lobbying, program fraud and tobacco smoke, are included in Appendix F. The state does not have to submit these forms as part of the Application/Annual Report, but they must be maintained on file in the state’s MCH program’s central office. TVIS provides capability for the state to certify that the required assurances/certifications are maintained on file and the state can provide them at HRSA’s request.
The Table of Contents is automatically generated by TVIS, and conforms to the headings in the different Parts/Sections of this Guidance.
In follow-up to a legislatively required comprehensive Five-Year Needs Assessment, the state develops a five-year Title V program plan. Consistent with the block grant concept, the state has flexibility in the types of programs and activities that it implements to address the unique needs of their individual MCH populations. As depicted by the process flow diagram in Figure 4, a state’s priority needs should “drive” the development of a five-year program plan that is responsive to the needs identified and is performance driven.
Figure 4. MCH Block Grant Logic Model
SSTEP
1
STEP
1
Conduct a comprehensive Title V MCH program Five-year Needs Assessment |
|
STEP
2
Review and summarize MCH Population Needs, Program Capacity, and Partnerships/ Collaborations |
|
STEP
3
Identify
(7-10) State Title V Program priority needs, which |
|
STEP
4
Develop program strategies to address the identified priority needs during the five-year reporting period
|
|
STEP
5
Identify areas of alignment between the state priorities/ strategies and the NOMs
|
|
|
|
|
|
|
|
|
|
STEP
6
Based on priorities and strategies, select five of the 15 NPMs (one per each of the five population domains) for programmatic focus |
|
STEP
7
Establish SPMs to address each priority need that is not being addressed by one of the five selected NPMs
|
|
STEP
8
Review the selected NPMs and SPMs to ensure that every identified priority need is being addressed through one or more of the NPMS or SPMs
|
|
STEP
9
Develop one or more ESMs for each of the five selected NPMS
|
|
STEP
10
At the state’s discretion, consider the need to develop one or more SOMs
|
|
|
|
|
|
|
|
|
|
STEP
11
Establish five-year performance objectives for each selected NPM, SPM, and, SOM, if applicable
|
|
STEP
12
Report performance indicators for NPMs, ESMs, SPMs and SOMs in Annual Report/ Application
|
|
STEP
13
Analyze annual and multi-year performance trends
|
|
STEP
14
In interim year, Annual Reports/ Applications, reassess and update strategies and objectives for selected NPMs, SPMS, & SOMs, if applicable, to achieve desired outcomes |
|
STEP
15
Conduct a comprehensive Title V MCH program Five-year Needs Assessment
|









The state begins each five-year cycle by conducting a comprehensive Title V Five-Year Needs Assessment. This Needs Assessment includes a comprehensive review of MCH population needs, program capacity, and partnerships/collaborations that are critical components of a state’s system of care for addressing the needs of its MCH population. Based on the findings of the Five-Year Needs Assessment, the state identifies 7-10 Title V MCH priority needs. Using the State Action Plan Table as a working tool, the state develops strategies and overarching five-year objectives to address the identified priority needs. The state examines areas of potential alignment between its MCH priority needs and the Title V NOMs and NPMs, which informs the selection of at least one NPM in each of the five population domains for programmatic focus over the five-year cycle. Priority needs not addressed by the selected NPMs will require the development of a targeted SPM. The state can chose to develop as many SPMs as needed to ensure that each priority need is addressed either by a SPM or by a NPM. While not required, the state may choose to also develop a SOM to complement the NOMs. For each NPM selected, the state is required to develop at least one ESM that further defines how the state plans to monitor and assess its annual progress in addressing the selected NPMs. In the four interim year Application/Annual Reports, the state reports on its ongoing needs assessment efforts, its success in implementing the five-year Title V program plan and its progress in achieving the established performance objectives for each selected NPM, SPM and ESM.
By July 15 of each year, states and jurisdictions are required to submit an Application/Annual Report for the federal funds they receive through the MCH Block Grant. In addition, the state is required to conduct and report on a comprehensive, statewide Needs Assessment every five years. See Appendix G for the Application/Annual Report Timeline. The findings of this Needs Assessment and the priority needs identified as a result of this process provide the basis for the development of a five-year Action Plan for the state Title V program. As new findings become available through the state’s ongoing/updating needs assessment efforts and the analyses of annual performance data, the state may refine its Action Plan (e.g., performance objectives) in interim years to achieve targeted outcomes in state and national MCH priority areas. These changes may include the substitution of new or revised strategies, ESMs and/or SPMs for existing strategies and measures. States are encouraged not to change the selected NPMs during the five-year reporting cycle. If a state determines that a NPM needs to be changed, clear justification must be provided to the MCHB Project Officer.
The state’s narrative Application/Annual Report includes the following sections:
Executive Summary;
Overview of the State;
Needs Assessment;
Financial Narrative;
Five-Year State Action Plan;
Public Input;
Technical Assistance.
States should structure the narrative discussion of the Application/Annual Report to include the sections cited above. A detailed explanation of the specific discussion points that the state should include in each section is provided below.
Comprised of three sections, the Executive Summary is intended to be a standalone document that enables the reader to acquire a clear understanding of the state’s
Title V program without having to read the entire MCH Block Grant Application/Annual Report. Limited to no more than five printed pages, the Program Overview (Section III.A.1) is the main narrative section in the Executive Summary. While limited to no more than one printed page per section, , the remaining two sections (Section III.A.2 and Section III.A.3) enable a state to reflect on the value and impact of the MCH Block Grant program in promoting the health and well-being of its MCH population.
In addition to serving as an introduction to the state’s MCH Block Grant Application/Annual Report, the Executive Summary serves as the narrative portion of the TVIS State Snapshot. Publicly available as a TVIS Web report, this document serves as a quick point of reference for policy makers, national MCH leadership associations and programs, local and state MCH stakeholders, state Title V programs, families, academia and other interested individuals. The State Snapshot incorporates key information contained in the State’s MCH Block Grant Application/Annual Report into a formatted document that states can use in their Title V program outreach and health promotion efforts.
1. Program Overview
The goal of the Program Overview section is to convey key descriptors about the state’s Title V program (i.e., operational framework, needs assessment findings, MCH priorities, program goals and strategies, five-year action plan and performance monitoring) in a concise, yet substantive, overview. While a state can update its Executive Summary annually, the overall content should reflect the state’s five-year action plan.
Specifically, the state should address the following components as part of the narrative discussion in this section.
A brief introduction to the state’s Title V program and its operational framework;
A high level overview of the working framework used by the state to carry out its needs assessment, program planning and performance reporting activities;
A concise summary of the state’s needs assessment findings (i.e., 2020 Five-Year Needs Assessment and interim year needs assessment updates), which includes a description of the state’s MCH population needs, emerging needs, Title V program capacity and internal/external partnerships;
A synopsis of the state Title V program’s identified MCH priorities and Five-Year State Action Plan, which addresses the selected NPMs and established SPMs in the context of a state’s identified MCH priority needs;
The role of the state Title V program in supporting and assuring comprehensive, coordinated and family-centered services, including services for CSHCN; and
A description of program evaluation efforts, noted accomplishments and ongoing challenges, with a focus on the implementation of evidence-based or -informed practices and the effectiveness of current program strategies in improving MCH outcomes.
2. How Federal Title V Funds Complement State-Supported MCH Efforts
The Title V MCH Block Grant is a federal/state partnership with 59 states and jurisdictions, which enables each state/jurisdiction to address the individual health service needs of the mothers, infants and children, including CSHCN, in the state. Consistent with the block grant concept, states have discretion in determining how to best invest their federal Title V funds to most effectively complement state-supported efforts in meeting their unique MCH needs.
The purpose of this section is to allow a state the opportunity to reflect on the critical role of federal Title V funds in supporting the state’s overall MCH efforts. In its narrative discussion, the state should clearly demonstrate the federal-state partnership in action. The state should identify specific programming areas in which federal Title V funds have served to complement state-led efforts in assuring the health and well-being of the MCH population while contributing to a strong public health infrastructure. Specific discussion points for demonstrating the impact of federal Title V funds on state-led MCH efforts may include, but are not limited, to the following:
Augmentation of State and other non-federal funds to assure the delivery of core MCH services;
Comparison of federal Title V expenditures with state Title V expenditures, by service level of the MCH Pyramid, to demonstrate how federal Title V funds complement state funds in providing a range of MCH services;
Comparison of federal Title V expenditures with state Title V expenditures, by individual MCH populations, to illustrate how federal Title V funds support gap-filling services, specialty services and other initiatives targeted at specific MCH populations or sub-populations;
Core support for the state’s MCH program capacity and public health infrastructure, which includes enhancing the Title V program management structure, securing an adequate and well-trained MCH workforce, investing in family partnerships and navigator services, improving MCH data analytics and facilitating other systems-building efforts; or
Expansion of State and local agency MCH services.
3. MCH Success Story
This section provides an opportunity for the State Title V program to highlight an MCH success. While the success story may have been achieved through multiple partnerships and funding sources, the specific contributions of the Title V program in achieving the successful outcome should be clearly documented. The success story may be specific to one or more MCH population domains or related to a state’s cross-cutting and systems-building efforts. Capacity and systems-building successes should be framed in the context of how they ultimately impacted the lives of mothers, children and families in the state.
In selecting one success story to highlight, a state should consider the purpose of the Title V program and if the selected success story clearly reflects this purpose. Consideration in selecting the success story should be given to how clearly it demonstrates the value of the Title V program and if the noted success could have been achieved in the absence of Title V funding.
It is recognized that State Title V programs have numerous successes, and it may be difficult for a state to decide on one success story to highlight. A state has the option to present a different success story each year in its MCH Block Grant Application/Annual Report, which will provide for greater representation of the breadth and impact of Title V-funded services across the five-year reporting period.
Overview of the State
The intended purpose of this overview is to introduce a reader to the applicant state. Principal characteristics of the state, such as its demographics, geography, economy and health care environment, should be succinctly summarized to provide the reader with needed context for understanding the Title V program structure and approaches described in the Application/Annual Report.
Specifically, the State Overview should include a description of:
The state’s demographics, geography, economy and urbanization;
The state’s unique strengths and challenges (e.g., availability and access to health
care services) that impact the health status of its MCH population, including CSHCN;
The defined roles, responsibilities and targeted interests of the state health agency and how they influence the delivery of Title V services;
Components of the state’s systems of care for meeting the needs of underserved and vulnerable populations, including CSHCN. This discussion may include, but is not limited to, the following descriptors:
Population served;
Health services infrastructure (e.g., number of children’s hospitals, pediatric specialists, accountable care organizational structure, etc.);
Integration of services, such as medical, physical, behavioral and mental health, social services and education; and
Financing of services (e.g., managed care arrangements and Medicaid eligibility).
Specific state statutes and other regulations that have relevance to the MCH Block Grant authority and impact the state’s MCH and CSHCN programs.
An organizational chart should be included as an attachment.
The Title V legislation (Section 505(a)(1)) requires the state, as part of the Application, to prepare and transmit a comprehensive statewide Needs Assessment every five years that identifies (consistent with the health status goals and national health objectives) the need for:
Preventive and primary care services for pregnant women, mothers and infants up to age one;
Preventive and primary care services for children; and
Services for children with special health care needs.
Findings from the Five-Year Needs Assessment serve as the cornerstone for the development of a five-year Action Plan for the State MCH Block Grant. The three-year period covered by this Guidance will include Interim Year Applications/Annual Reports for FY 2022-2024/2020-2022, which represent Years 02-04 of the Five-Year State Action Plan developed in response to the 2020 Five-Year Needs Assessment. States will submit the next Five-Year Needs Assessment Summary as part of the FY 2026 MCH Block Grant Application/FY 2024 Annual Report on July 15, 2025.
Needs Assessment Update
The changing MCH population demographics, emerging health trends and shifting program capacity require that states routinely engage in selected steps of the Needs Assessment process. During any interim year when a state is not reporting on its Five-Year Needs Assessment, a state should reference and summarize the findings from its ongoing needs assessment activities in the Needs Assessment Update section of the Application/Annual Report. This update should include a discussion of the following items:
A brief description of the state’s ongoing needs assessment activities (e.g., MCH data collection and analyses, program evaluation, key informant interviews, customer satisfaction surveys, advisory councils, and other approaches for soliciting individual feedback and conducting ongoing performance monitoring and assessment) and the extent to which families, individuals and other stakeholders were engaged in the process;
Noted changes in the health status and needs of the state’s MCH population, as compared to the identified priority needs for the MCH Block Grant;
Noted changes in the state’s Title V program capacity or its MCH systems of care, particularly for CSHCN, and the impact of these changes on MCH services delivery;
The breadth of the state’s Title V partnerships and collaborations with other federal, tribal, state and local entities that serve the MCH population;
Efforts undertaken by the state to operationalize its Five-Year Needs Assessment process and findings; and
Changes in organizational structure and leadership.
The needs assessment update should include a dedicated section that describes emerging public health issues and the state’s capacity and resources to address them.
Five-Year Needs Assessment Summary
States will not be required to submit a Five-Year Needs Assessment Summary during the three-year period covered by this Application/Annual Report Guidance. This section is included to provide reference information and context for the state’s current Five-Year State Action Plan, which was developed in follow-up to the 2020 Five-Year Needs Assessment.
The mechanism for states to report on the legislatively required, comprehensive and statewide Five-Year Needs Assessment is the Needs Assessment Summary, which is submitted as part of the first year Application/Annual Report of a new five-year cycle. The state should present a concise summary (up to 20 printed pages) of the Five-Year Needs Assessment process, methodology and findings, as described below. Given that the findings inform the development of the state MCH Block Grant’s five-year State Action Plan, the Needs Assessment Summary is retained in its original form as part of the four subsequent interim year Applications/Annual Reports. As it reflects a point-in-time, the state does not update the Five-Year Needs Assessment Summary in the interim years. Such updates are presented in the Needs Assessment Update section of the interim year Applications/Annual Reports. Each annual update, along with the original Five-Year Needs Assessment Summary, is prepopulated in each year’s Application/Annual Report across the five-year reporting cycle.
The Needs Assessment Summary is intended to emphasize only the key findings of the state’s Five-Year Needs Assessment. Given the scope and comprehensive nature of the Five-Year Needs Assessment, a state’s findings may exceed the required content for the Needs Assessment Summary. States may opt to develop a more detailed and complete Five-Year Needs Assessment document, which is tailored to meet their individual MCH program needs. If such a document is created by the state and made accessible on a public website, the state is encouraged to cite the URL for the website as part of its Application/Annual Report discussion. States may also choose to submit more detailed documentation on their Five-Year Needs Assessment findings as an attachment for this section.
Process Description
This description of the overall process/methodologies used by the state in conducting its Title V Five-Year Needs Assessment provides context for the interpretation of the reported findings and the priority needs subsequently identified. A report 5 prepared for MCHB on the needs assessment process cited four characteristics for states to consider in moving from a solely data-driven needs assessment effort to conducting a comprehensive assessment of its priority issues and stakeholder needs. These characteristics are:
A clear leadership structure for assembling data from both public and private sources;
Engagement of stakeholders for soliciting meaningful programmatic input;
A structured and inclusive priority-setting process; and
Collaborative program planning.
In describing the Five-Year Needs assessment process, states should provide a high-level summary that includes:
Goals, framework and methodology that guided the Needs Assessment process;
Level and extent of stakeholder involvement, including families, individuals and family-led organizations;
Quantitative and qualitative methods that were used to assess the strengths and needs of the MCH population in each of the five identified population health domains, MCH program capacity and supportive partnerships/collaborations;
Data sources utilized to inform the Needs Assessment process; and
Interface between the collection of Needs Assessment data, the finalization of the state’s Title V priority needs and the development of the state’s Action Plan.
Findings derived from the comprehensive Five-Year Needs Assessment serve to inform the Title V program’s strategic planning, decision-making and resource allocation efforts. These findings also provide a benchmark against which states can compare and assess the progress that they have achieved during the five-year reporting period.
The Needs Assessment Summary should highlight the state’s noted MCH strengths/needs in three main areas:
MCH Population Health Status
Title V Program Capacity
Title V Program Partnerships, Collaboration and Coordination
The state should clearly describe the health status of the MCH population within each of the five population health domains (i.e., Women/Maternal Health, Perinatal/Infant Health, Child Health, Adolescent Health, and CSHCN), based on the quantitative and qualitative analyses conducted. Specific discussion points should include:
A summary of the noted strengths and needs in the overall MCH population and in specific MCH sub-population groups;
A concise description of the state’s successes, challenges and gaps related to major morbidity, mortality, health risks or wellness for each of the five population health domains. At a minimum, the discussion should include the major health issues reflected in the state’s priority needs relative to the MCH population as a whole or specific sub-populations when stratified by age, income, geography, frontier/rural/urban status, or other relevant characteristics; and
An analysis of current MCH Block Grant efforts in addressing the needs of its MCH population to determine areas of success and areas in which new or enhanced strategies/activities are needed.
A state’s assessment of its Title V program capacity should examine current resources, staffing and organizational structure, state agency coordination and family partnerships. States should summarize the findings from their Five-Year Needs Assessment relative to each of these categories in the following sections.
In reporting on the organizational structure of the Title V program, the state should:
Describe the organizational structure and placement of the Governor, state health agency and the Title V MCH and CSHCN programs in the state government.
Clarify how the state health agency is "responsible for the administration (or supervision of the administration) of programs carried out with allotments” under Title V [Section 509(b)]. This description should include all of the programs that are funded by the federal-state MCH Block Grant.
In summarizing the state Title V program capacity, the state should describe the state Title V agency's capacity to promote and protect the health of all mothers and children, including CSHCN. Included in this description should be a discussion of the steps taken by the MCH and CSHCN programs to ensure a statewide system of services that reflect the components of comprehensive, community-based and family-centered care. The state should also describe the extent to which the Title V program collaborates with other state agencies, health services entities and private organizations to support health services delivery at the community level.
Specifically, the state’s summary on Title V program capacity should include the following:
A description of the state’s Title V capacity to provide and assure services within each of the five population health domains.
An expanded discussion on the state’s capacity for serving CSHCN, which includes the Title V program’s ability to provide rehabilitation services for blind and disabled individuals under the age of 16 receiving benefits under Title XVI (the Supplemental Security Income Program), to the extent that medical assistance for such services is not provided under Title XIX (Medicaid). If applicable, states may describe their capacity to serve CSHCN and their families by referencing the National Consensus Standards for Systems of
Care for Children and Youth with Special Health Care Needs as a guiding framework (AMCHP, 2014)6.
State Title V program efforts to implement the core public health functions (assessment, policy development and assurance) and to achieve increased accountability through ongoing performance measurement and monitoring require an adequately sized and skilled workforce. In reporting on their Title V program capacity, states should describe the strengths and needs of their MCH and CSHCN workforce. Specifically, the state should include the following information in its MCH workforce summary:
Number, location and full-time equivalents (FTEs) of state and local staff who work on behalf of the state Title V programs;
Names and qualifications (briefly described) of senior level management employees who serve in lead MCH-related positions and program staff who contribute to the state’s planning, evaluation, and data analysis capabilities;
Number of parent and family members, and youth including CSHCN and their families, who are on the state’s Title V program staff and a brief description of their roles (e.g., paid consultant or volunteer);
Additional MCH workforce information, such as the tenure of the state MCH workforce and projected shifts in the MCH and CSHCN workforce over the five-year reporting period, that aligns
workforce capacity with the achievement of Title V program goals; and
Additional information that briefly describes the workforce capacity of key MCH partners (external to the State Title V program), which are essential to the implementation of the State Action Plan.
Title V programs partner with a range of federal, state and local entities to further supplement state agency capacity in meeting the needs of its MCH population. In summarizing these partnerships as well as the engagement of stakeholders in programmatic decisions, the state should describe relevant organizational relationships that serve to expand the capacity and reach of a state Title V program in meeting the needs of its MCH population, including CSHCN. The state should reference formal and informal collaboration processes and partnerships with the public and private sector and with state and local levels of government. In addition, the state should describe the process for involving stakeholders and their contributions to the Title V program.
In summarizing the strengths and weaknesses of its partnership building and collaboration efforts, the state should describe its partnerships and relationships with such programs as:
Other MCHB investments, which include the State System Development Initiative (SSDI) Grants; Family-to-Family Health Information Centers; MCHB investments related to newborn and early childhood screenings, epilepsy, genetics, blood disorders; Maternal, Infant, and Early Childhood Home Visiting (MIECHV) Grants; Healthy Start Grants; Early Childhood Systems of Care (ECCS) Grants; MCH Training programs; and MCHB investments relating to injury prevention, autism, developmental disabilities, adolescent health, workforce development, oral health, bullying and emergency medical services for children;
Other Federal investments (e.g., ACF, CDC and USDA-funded programs, such as immunizations, infant and child death reviews and WIC);
Other HRSA programs (e.g., community health centers and HIV/AIDS/AIDS programs and Area Health Education Centers);
State and local MCH programs (e.g., local health departments and urban MCH programs);
Other programs within the State Department of Health (e.g., chronic disease, prevention and health promotion, immunization, vital records and health statistics, injury prevention, behavioral and mental health and substance abuse);
Other governmental agencies (e.g., Medicaid, CHIP, Education, Social Services/Child Welfare, Social Security Administration, Corrections and Vocational Rehabilitation Services);
Tribes, Tribal Organizations and Urban Indian Organizations;
Public health and health professional educational programs and universities; and
Other state and local public and private organizations that serve the state’s MCH population.
c. Identifying Priority Needs and Linking to Performance Measures
Consistent with Figure 4 on page 14, findings from the Five-Year Needs Assessment should drive the state’s identification of its seven to ten highest MCH priority needs for the five-year reporting cycle. The selected priorities may address the defined MCH population groups and/or cross-cutting/ systems building areas, and they should reflect the unique needs of the state. In addition, the identified priority needs should address areas in which a state believes that targeted interventions can result in needed improvements to its health care delivery systems. Once identified, the priority needs inform the selection of a minimum of five NPMs, one in each of the MCH population health domains, and the development of SPMs. Collectively, the NPMs and SPMs should address the state’s identified priority needs.
TVIS will prepopulate the priority needs provided in the previous year. States should review their priority needs to ensure alignment within the State Action Plan where priorities are linked with the existing National Outcome Measures (NOMs), NPMs, SPMs and ESMs. States can classify priority needs as New, Continued, or Revised under the following conditions:
New: Priority Need is added
Revised: Description is changed for a Priority Need provided in the previous interim year
Continued: No changes for a Priority Need provided in the previous interim year.
The TVIS will record up to 10 priority needs, but a state can include additional priorities in a field note, if desired.
The narrative discussion supplements the listing of the final priority needs by providing a rationale for how the priority needs were determined and how they link with the selected national and state performance measures. Specifically, this discussion should include:
Methodologies used to rank the broad set of identified needs and the state’s process for selecting its final seven to ten priorities;
Emerging issues or other frequently cited needs that were not included in the final list of priority needs and a rationale for why they were not selected;
Factors that contributed to changes in the state’s priority needs since the previous five-year reporting cycle; and
Relationship between the priority need and the selected national and/or state performance measures in driving improvement.
Financial Narrative
The development and implementation of a workable State Action Plan requires careful analysis and utilization of available funding and resources. Building on the assessment of state MCH population needs and Title V program needs, the state should present a budget plan for the Application year that aligns its proposed Title V program activities with the identified MCH needs. In addition, the state should report and reflect on its MCH Block Grant expenditures for the Annual Report year. This reflection should include a comparison of planned, budgeted activities with actual expenditures for that fiscal year and link the allocation of financial resources with outcomes achieved relative to the State’s Title V program plan.
The combined Expenditure and Budget narrative sections should demonstrate accountability in the state’s use of its federal and state MCH Block Grant funds to meet the program’s legislative intent, i.e., “to improve the health of all mothers and children” [Section 501(a)]. States should reflect on whether the Title V program efforts and outcomes discussed in the State Action Plan and other sections of the Application/Annual Report could have been achieved without federal MCH Block Grant funding support.
States should maintain expenditure and budget documentation for the MCH Block Grant, consistent with the requirements in Section 505(a) and Section 506(a). Per Section 506(b)(1), each state is required to conduct an audit of its expenditures every two years. Additional information to assist the state in its financial reporting can be found in Appendix H.
Expenditures
In describing its MCH Block Grant expenditures, states should reflect on the federal and non-federal monies that have been obligated and spent. This discussion is intended to provide the reader with an understanding of how the supported programs and services link with the state’s MCH priority needs and meet the requirements of Title V legislation.
The expenditure narrative should demonstrate the Federal/State partnership and how federal support complements the state’s total MCH investment, as reflected on Form 2, Lines 3-6 (i.e., reported State, Local, Other, and Program Income expenditures). States should monitor expenditures regularly to ensure compliance with legislative financial requirements. The state should document and explain how the reported expenditures comply with the 30%-30%-10% requirements, as specified in Section 504(d) and Section 505(a)(3). Significant variations of more than 10% in the expenditure data reported on Form 2 and Form 3, as compared to the state’s planned budget for that same fiscal year, should be explained in the narrative discussion. In addition, the state should reflect on the number/percent of the MCH population who are served by Title V, as reported on Form 5, and provide a description of the state’s efforts to expand its reach. Challenges faced by the state should be noted and addressed.
It is recognized that funds for the reporting year may be not be fully expended at the time of submission. Given that the state is required to submit a Federal Financial Report (FFR) with the final financial data within 3 months of the expiration of funds, the most recent expenditure data should be reported at the time of submission. The state may wish to utilize the form or field notes on Forms 2 and Form 3 to explain any discrepancies in its submitted financial data and work with its MCHB Project Officers in reporting final expenditures.
States report the federal and non-federal MCH Block Grant expenditures separately on the budget/expenditure forms. This breakdown should be further examined as part of the narrative discussion.
With respect to Medicaid, Title V should be the payer of last resort and MCH Block Grant funds cannot be used to reimburse a claim for a service that is otherwise covered under Medicaid. Additionally, service providers receiving MCH Block Grant funds are strongly encouraged to seek payment from other public and private insurance providers when applicable. The state should describe how services supported by the MCH Block Grant reflect services that were not covered or reimbursed through the Medicaid program or another provider.
Budget
In its budget narrative, the state should present a plan that describes how federal and non-federal Title V funds will be used to address the state’s priority needs, improve performance related to the targeted MCH outcomes and expand its systems of care for both the MCH and CSHCN populations. The budget narrative should also demonstrate and assure the state’s commitment to complying with the legislative financial requirements (e.g., 30%-30%-10% requirements) and block grant program regulations.
Similar to the narrative description that the state provided for its expenditures, the budget narrative should demonstrate the federal-state partnership and how federal MCH Block Grant support will be utilized to complement the state’s planned total match (i.e., State, Local, Other, and Program Income funds) for the Application year. The budget narrative should highlight the State’s MCH/CSHCN program and align with the identified MCH/CSHCN priorities. This discussion should clearly articulate how federal and non-federal MCH Block Grant funds will support the activities that are described in the State Action Plan for the upcoming budget period.
While the final federal MCH Block Grant allocation is not yet known, states should use the allocation for the current fiscal year as a basis for determining budget estimates for federal and non-federal MCH Block Grant funds in the Application year. In the budget narrative discussion, the state should describe sources of other federal MCH dollars (as noted on Form 2, Line 9), state matching funds and other state funds used by the agency in its Title V programming. This discussion should include how MCH Block Grant funds support essential services, as defined by the Title V MCH Services Block Grant Pyramid (Figure 1), for the three legislatively defined populations. The narrative discussion should provide an explanation of how the planned funding will support the budget estimates for individuals served and types of services provided, as reported on Form 3a and Form 3b.
Significant variations in the budgeted amounts reported by a state on Form 2 and Form 3, as compared to previous years’ reporting, should be explained. Any budget notes provided on Form 2, Form 3a, and Form 3b should be further clarified in the narrative discussion.
The state should describe its plan to meet and monitor the required match requirements, which includes a $3 match in non-federal funds for every $4 of federal MCH Block Grant funds expended [Section 503(a)] and the maintenance of effort from 1989 [Section 505(a)(4)]. The state should also briefly describe any continuation funding for special projects [Section 505(a)(5)(C)(i)] or consolidated health programs as defined in Section 501(b)(1), and how funding will only be used consistent with Title V nondiscrimination provisions [Section 505(a)(5)(B)].
States are reminded that “any amount payable to a state under this title from allotments for a fiscal year, which remains unobligated at the end of such year, shall remain available to such state for obligation during the next fiscal year. No payment may be made to a state under this title from allotments for a fiscal year for expenditures made after the following fiscal year” [Section 503(b)]. While states apply annually for MCH Block Grant funding, a state has two years in which to expend the federal MCH Block Grant allocation awarded in any fiscal year.
Five-Year State Action Plan
States shall develop a five-year State Action Plan in follow-up to the Five-Year Needs Assessment. This Action Plan serves as the Application/Annual Report narrative discussion for the state on their planned activities for the Application year and the activities that were implemented in the Annual Report year. Activities should be discussed relative to the pertinent domain, state priority need, Title V program goal, evidence-based or -informed strategies and national and state-specific performance and outcome measures. Building on its needs assessment, financial planning and performance reporting, the state’s five-year action planning begins with the completion of the State Action Plan Table.
Based on the logic model presented in Figure 4, the State Action Plan Table (Figure 5) is intended to serve as a planning tool for states to use in identifying key strategies, objectives and relevant performance measures to align with the selected priority needs. Organized by the five MCH population health domains (i.e., Women/Maternal Health, Perinatal/Infant Health, Child Health, Adolescent Health and CSHCN) and the sixth cross-cutting and systems building domain, the State Action Plan Table should include the following components.
Priority Needs – Title V legislation directs states to conduct a state-wide MCH Needs Assessment every 5 years to identify the need for preventive and primary care services for pregnant women, mothers, infants, children, and CSHCN. From this assessment, states select seven to ten priorities for focused programmatic efforts over the five-year reporting cycle.
Strategies – Strategies are the general approaches taken to achieve the objectives; activities are specific actions to implement the strategies. Program activities for implementing the identified strategies will be discussed and updated annually as part of the State Action Plan narrative.
Objectives – An objective is a statement of intention with which actual achievement and results can be measured and compared. SMART objectives are Specific, Measurable, Achievable, Relevant and Time-phased.
Performance Measures – For purposes of the MCH Block Grant, performance measures include both national and state-specific measures (i.e., NPMs, ESMs,
SOMs, and SPMs). States select performance measures that align with their identified strategies, and to the NOMs and SOMs.
States should update the Five-year State Action Plan Table as needed for each year’s Application/Annual Report.
Figure 5. Five-Year State Action Plan Table
Priority Needs |
Strategies |
Objectives |
National and State Performance Measures |
Evidence–Based or –Informed Strategy Measures |
National and State Outcome Measures |
Women/Maternal Health |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
Perinatal/Infant Health |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
Child Health |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
CSHCN |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
Adolescent Health |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
Cross-cutting/Systems Building |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
State Action Plan Narrative Overview
State Title V Program Purpose and Design
Each state Title V program is unique in its organizational and fiscal structure; operating statutes and regulations; available resources; targeted MCH needs; established performance goals; and portfolio of supported programs and services. States should provide a “big picture” overview of their Title V program to give context to the activities and approaches that are described in the State Action Plan. Noted discussion points should include:
The Title V program’s partnership and leadership roles in accomplishing the MCH Block Grant’s goals and mission;
The Title V program’s framework (e.g., life course model) and strategic approach to addressing the identified MCH priorities while considering program successes, ongoing challenges and emerging issues;
The purpose and commitment of the Title V program in providing a foundation for family and community health across the state and in assuring access to the delivery of quality health care services for mothers, infants and children, including CSHCN.
Given the uniqueness of each state, the Title V program has flexibility in writing a narrative description that best conveys the elements it considers to be the most critical in giving context to the Title V program. This description should respond to the question, “What does a reader need to know about the Title V program to understand the activities and approaches that are described in the State Action Plan?” Most relevant to this discussion is the Title V program’s demonstrated leadership in such areas as:
Serving as a convener, collaborator and partner in addressing MCH issues;
Supporting coordinated, comprehensive and family-centered systems of services at state and local levels, which may include the implementation of AMCHP’s National Consensus Standards for Systems of Care for Children and Youth with Special Health Care Needs or other population health strategies7;
Developing and utilizing innovative and evidence-based or -informed approaches to address cross-cutting issues that impact the health status of specific MCH populations and sub-populations, such as social determinants of health; and
Implementing the core public health functions of assessment, assurance and policy development through program efforts that are supported by the MCH Block Grant.
State MCH Capacity to Advance Effective Public Health Systems
In developing the Action Plan, the state should describe state MCH capacity (e.g., workforce, family partnerships and integrated health care delivery partnerships) that influence the Title V program’s ability to meet its planning goals and objectives.
MCH Workforce Development
Successful implementation of the five-year State Action Plan requires a workforce that is adequate in size, effectively trained and properly supported. As noted in Section III.C.1, the state should provide an update on its MCH program capacity, which includes workforce capacity, as part of the discussion in the Needs Assessment Update section of interim year MCH Block Grant Applications/Annual Reports. In this narrative section, the state should describe its progress in implementing a plan to strengthen the MCH workforce and advance a future MCH workforce vision (e.g., types of personnel and skill sets needed). Specific activities to meet the following four workforce goals, along with other state-identified goals, should be discussed.
Recruitment and retention of a qualified Title V program staff;
Assessment of training and professional development needs for new and seasoned Title V program staff and family leaders;
Current and anticipated training needs of key MCH partners (external to the Title V program), as relevant; and
Innovations in staffing structures, including key partnerships that enhance the capacity of Title V to meet its goals and objectives and support training of the State Title V workforce (i.e., partnerships with academic institutions, other training providers, student internships, etc.).
In addition to the required narrative discussion on the state’s MCH workforce activities, a state may find the sample worksheet in Figure 6 on the following page to be helpful in organizing and annually assessing its MCH workforce data and training information. This worksheet is provided as a sample tool only. The state is not required to complete the worksheet presented in Figure 6 as part of its MCH Block Grant Application/Annual Report.
Appendix J lists several tools/resources to assist state Title V programs in assessing the training and professional development needs of their staff and in identifying learning opportunities.
Figure 6. Sample State Title V Workforce Information Sheet
-
Title V Program Workforce FTEs
Title V-Funded Positions
Total Number of FTEs: ______
New Title V-Funded Staff Onboarded in Past Year
Total Number of New FTEs: ______
Types of Position:
____________
____________
____________
____________
____________
Title V-Funded Positions Currently Vacant
Total Number of Vacant FTEs: ______
Types of Position/Length of Time Position Has Been Vacant:
____________/____________
____________/____________
____________/____________
____________/____________
____________/____________
Training Needs and Resources
Current or Anticipated Title V Professional Development and Training Needs
____________
____________
____________
____________
____________
Key Resources/Partners Needed to Meet Title V Professional Development and Training Needs
____________
____________
____________
____________
____________
Family Partnership
As discussed on page 8, family partnership is defined in the MCH Block Grant as: “the intentional practice of working with families for the ultimate goal of positive outcomes in all areas through the life course. Family engagement reflects a belief in the value of the family leadership at all levels from an individual, community and policy level.”
The state should provide an overarching discussion of its organizational capacity and vision for partnering with families, individuals and family-led organizations in all aspects of their Title V Action Plan development and implementation across all population domains. Descriptions of partnership activities may include, but are not limited to, the following areas:
Advisory Committees;
Strategic and Program Planning;
Quality Improvement;
Workforce Development and Training;
Block Grant Development and Review;
Materials Development; and
Program Outreach and Awareness
Training activities that serve to strengthen and advance family partnership in the Title V program, both in orientation and ongoing professional development, which are conducted for staff, family leaders, volunteers, contractors and subcontractors should be discussed. The state should describe the contributions of family and community leaders to Title V program processes, such as assessment of needs/assets, program planning, MCH and CSHCN services delivery, and evaluation/monitoring/quality improvement activities. This discussion should include the state’s efforts to partner with families and individuals who are representative of the MCH communities being served to ensure that their needs are properly identified and appropriately addressed.
The state should further address specific roles and responsibilities of families, individuals and family-led organizations at the direct care, organizational and governance, and policymaking levels and describe the outcomes and impacts of its established family partnerships on Title V program policies and activities Specific impacts of family partnership on each of the five MCH populations and on the Title V program’s cross-cutting and systems building activities should be included in the appropriate MCH domain narrative discussion.
MCH Data Capacity
Collection and reporting of accurate, timely and relevant MCH data is essential to informed MCH program planning and implementation. Performance monitoring and quality assessment rely on such data. Comprehensive needs assessment and coordination of efforts across MCH-related programs are influenced, in part, by the state’s ability to collect, access, link, and analyze timely data across multiple systems and programs (e.g., vital records, child health surveys, MCH Jurisdictional Survey, newborn screening, Medicaid claims, immunization and birth defects registries, hospital discharges and WIC).
MCH Epidemiology Workforce
Ability to use MCH data relies on having a workforce trained in epidemiology, data analysis, and MCH data systems. In this section, the state should briefly describe its workforce capacity related to the management and analysis of MCH data in the Title V program. Included in the description should be the number of dedicated FTEs (e.g., epidemiologists) responsible for managing/analyzing MCH data, funding structure (e.g., solely funded through Title V, SSDI, or another public health program, or funded through multiple programs), levels of education and training, and designated roles/responsibilities. The state should reflect on its current MCH epidemiology workforce capacity, the impact of organizational changes (e.g., organizational restructuring, integration/collaboration with the Title V program, shifts in staffing, emerging demands for new skillsets and training) on the state’s MCH data capacity, and planned areas for continued development or change.
State System Development Initiative (SSDI)
Launched in 1993, the purpose of SSDI is to develop, enhance, and expand state and jurisdictional Title V MCH data capacity for responding to the needs assessment activities and performance measure reporting requirements in the MCH Block Grant. Such enhanced MCH data capacity is intended to enable states and jurisdictional Title V programs to engage in informed decision-making and resource allocation that supports effective, efficient and quality programming for women, infants, children, including CSHCN, and their families. SSDI complements the MCH Block Grant by improving the availability, timeliness, and quality of MCH data in the 59 states and jurisdictions. Utilization of these data is central to state and jurisdictional reporting on their Title V program assessment, planning, implementation, and evaluation efforts, along with related investments, in the yearly MCH Block Grant Application/Annual Report.
States who receive SSDI funding should provide a high-level narrative summary (up to three printed pages) that describe how this grant funding supports MCH data collection and reporting in the MCH Block Grant. This description should highlight the contributions of the SSDI grant in improving cross-program MCH data linkages and assuring direct, annual access to timely, electronic MCH health data. If a state does not receive SSDI funding, a statement should be entered in this section to indicate that the state is not a SSDI grant recipient.
Specifically, the state should address the following items in their narrative discussion.
The state’s progress with emphasis on the contributions of the SSDI grant in building and supporting accessible, timely and linked MCH data systems, as documented on Form 12;
The role SSDI plays in enabling ongoing Title V program assessment, monitoring and reporting; and
A description of key SSDI program activities, including any products or resource materials that were developed, which served to support State Title V program efforts in addressing its identified MCH priority needs, conducting the Five-Year Needs Assessment, implementing the Five-Year State Action Plan, and advancing data-driven MCH programming (e.g., core/minimum data set).
Given that the intended purpose of SSDI is to build and support MCH data capacity in the State Title V programs, program successes are largely demonstrated in the state’s MCH Block Grant reporting. As such, this narrative section will serve as the primary annual performance reporting for the state’s SSDI grant. SSDI grantees will continue to submit an annual performance report and an annual progress report. However, the required content of these reports will be adjusted to ensure that the annual reporting complements, but does not duplicate, the narrative reporting in a state’s MCH Block Grant Application/Annual Report.
While the narrative reporting in this section focuses on the contributions of the SSDI grant in strengthening the State Title V program’s data capacity, states may choose (but are not required) to submit a more detailed and complete description of their SSDI program activities as an attachment to the MCH Block Grant Application/Annual Report.
Other MCH Data Capacity Efforts
In this section, states should describe Title V data capacity efforts funded by sources other than SSDI, which support up-to-date MCH data and information systems. This description should highlight the state’s MCH epidemiological and data enhancement activities and how they support Title V program activities, such as the Five-Year Needs Assessment, annual MCH Block Grant performance measure reporting/monitoring and data-driven programming. Such efforts may include, but are not limited to, activities such as the ones listed in the SSDI section above but not funded by SSDI, the state’s partnership and collaboration in implementing national surveys and monitoring systems, the availability/accessibility of state and local MCH data information systems, the collection and tracking of real-time data, creation of data review boards, provision and sharing of data with other state/local and external partners, and advances in information technology that facilitates automated data analyses and reporting. States should also describe key challenges they face in their efforts to improve the use of MCH data.
MCH Emergency Planning and Preparedness
In the face of natural disasters, outbreaks, pandemics and other emergency situations, State Title V programs are often called upon to provide leadership and support in delivering critical MCH services and in assisting local communities to respond to the emerging threats and needs. Such a role requires the State Title V program to be proactive in its emergency preparedness planning and to coordinate with partners at the state and local levels to develop emergency preparedness and response plans that include the needs of the MCH population.
In this section, State Title V programs should describe their involvement in the administering agency’s emergency preparedness and response planning activities. There is no expectation for Title V programs to develop a new or separate Emergency Operations Plan (EOP). The discussion in this section should focus on the extent to which MCH is integrated into the state’s EOP, the role of the Title V program in the state’s emergency structure, and its participation in emergency preparedness planning activities (e.g., data assessment and surveillance, training, development of communications plans, and coordination with other public health programs). Specifically, the state should speak to the following questions in their narrative reporting:
Does the state have a written EOP, and how often is this plan reviewed?
Does the state’s EOP specifically consider the needs of the MCH population, which includes at-risk and medically vulnerable women, infants, and children?
Were Title V program staff involved or consulted in the planning and development of the State’s EOP?
Is Title V leadership included in the State’s emergency preparedness planning before a disaster?
Is Title V leadership part of the Incident Management Structure (IMS)? If so, where are they located within the IMS?
Based on ongoing Title V program needs assessment efforts and lessons learned from previous emergency responses, were critical gaps in emergency preparedness and/or surveillance data identified that could impact the state’s ability to adequately assess and respond to MCH population and program needs in a future disaster or public health emergency?
To what extent has the Title V program participated in the development of emergency preparedness and response training, communication plans and tools/strategies to enhance statewide preparedness for addressing potential short- and long-term impacts of disasters and emerging threats on the MCH population?
To what extent has the Title V program participated in the development of coordination plans with public health programs (e.g., newborn screening, newborn hearing screening, immunization, home visiting, WIC, shelters and other MCH programs), to enhance statewide preparedness for addressing potential short- and long-term impacts of disasters and emerging threats on the MCH population?
This annual narrative reporting is intended to assist the State Title V program in annually assessing the adequacy of the existing EOP in responding to an emerging public health threat or disaster that impacts the MCH population.
Health Care Delivery System
Public and Private Partnerships
Organizational relationships and the leveraging of federal and state program resources contribute to the services delivery capacity of a State Title V program. States should provide a description of their collaborative work with other federal, state and non-governmental partners, and how this work complements Title V program efforts to provide a systems approach to ensure access to quality health care and needed services for the MCH population. In this section, the state should describe key strategies and opportunities for strengthening the integration of health care delivery systems that serve women and children, key partners, alignment of resources and shared program goals. Efforts to assess the effectiveness of the state’s health care delivery systems in meeting the needs of women and children and the state’s consideration of new, innovative health care delivery models should also be discussed.
Title V MCH - Title XIX Medicaid Inter-Agency Agreement (IAA)
Within a state, the Title V program and Title XIX Medicaid program share a common goal in working to improve the overall health of the MCH population through affordable health care delivery systems and expanded coverage. Partnership and collaboration between these two programs allow for the effective leveraging of federal and state resources, which yields administrative efficiencies to help ensure that women and children are provided needed preventive services, health examinations, treatments and follow-up care. Section 509(a)(2) of Title V of the Social Security Act cites the need to promote “coordination at the Federal level of activities authorized under this title [Title V] and under title XIX….” Also, Section 1902(a)(11) of Title XIX requires State Medicaid agencies to enter into Inter-Agency Agreements (IAAs) with state Title V agencies. This provision further clarifies that Medicaid funds are to be used to reimburse expenditures made by the Title V agency for Medicaid-covered services to Medicaid recipients, as appropriate, (i.e., that Medicaid should be the first payer.)
The Code of Federal Regulations (CFR) further sets forth specific requirements for Medicaid State plans to describe coordination with relevant agencies, which includes Title V. (See Figure 7 below.)
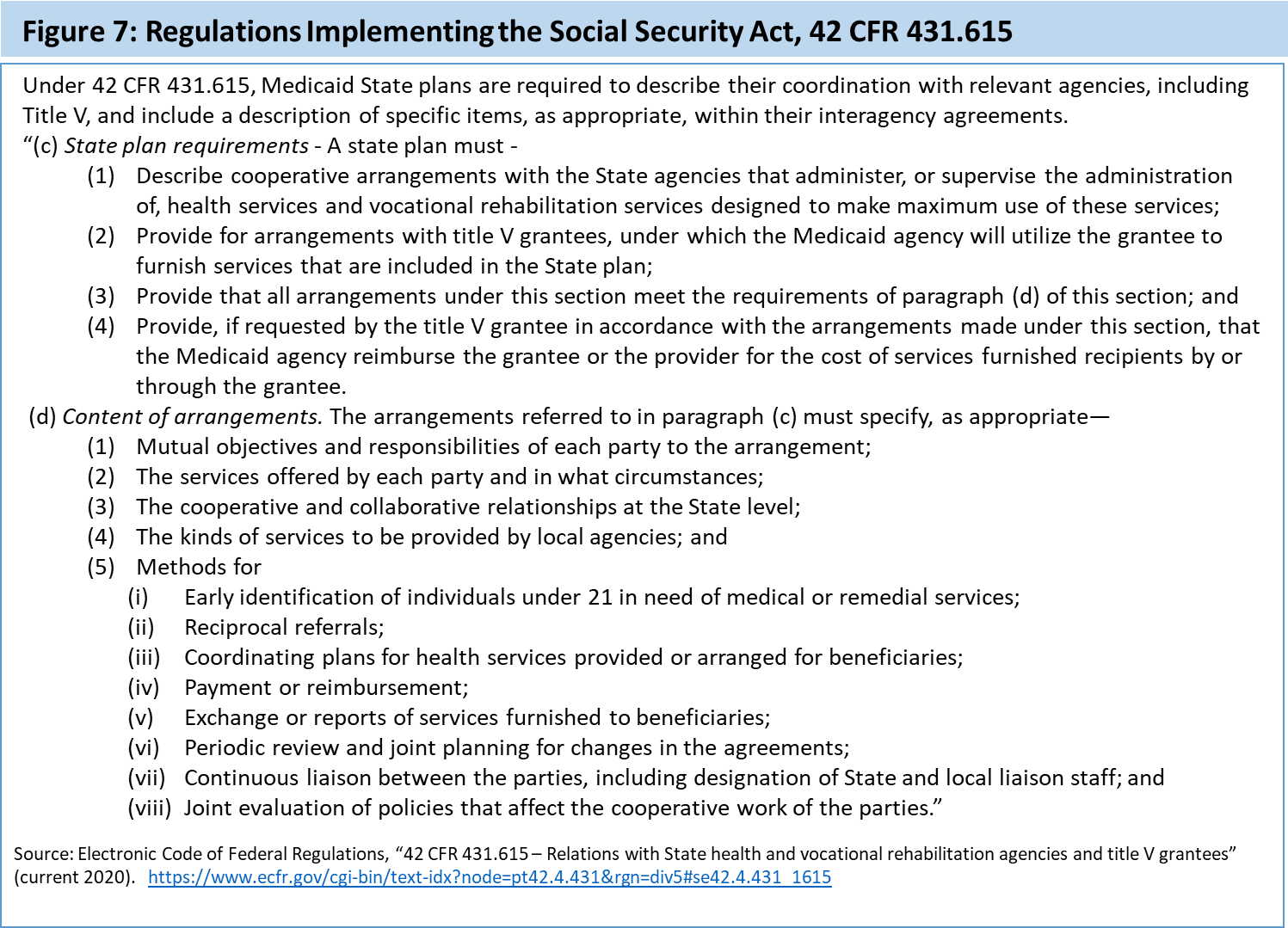
The state should provide a detailed description of the existing relationship between the Title V program and the Medicaid program, which builds on the noted areas of coordination and collaboration in the IAA/Memorandum of Understanding (MOU). A copy of the most recently signed IAA/MOU is a required attachment for this Application/Annual Report.
The state’s narrative discussion should address areas of defined coordination between the two programs and the benefits that have been realized. At a minimum, the discussion should address Title V program impacts in the following areas:
Program outreach and enrollment;
Health care financing (e.g., the percent of services delivered by managed care organizations (MCO), primary care case management (PCCM) and fee for service, if applicable);
Waivers or state plan amendments that influence health care delivery for the MCH population, particularly CSHCN; and
Joint policy level decision making on issues related to MCH services delivery and coverage, particularly for CSHCN.
In working to strengthen their Title V – Title XIX IAAs, states may wish to consider the strategies developed by the National Academy of State Health Policy (NASHP) under funding support provided by the HRSA/MCHB.8
c. State Action Plan Narrative by Domain
Supplemental to the overarching State Action Plan narrative discussion is the state’s detailed reporting, by MCH domain, on its specific Title V program activities for the Annual Report year and for the Application year. The order of the narrative reporting is organized to allow states to discuss their strategies, achievements and performance trends, relevant to the specific MCH domain, in the Annual Report year prior to presenting the planned activities and performance objectives for the Application year. The six MCH domains are:
Five MCH Population Domains
Women/Maternal Health
Perinatal/Infant Health
Child Health
Adolescent Health
CSHCN
Optional Domain
Cross-cutting/Systems Building
The state should include a discussion of the selected NPM and related ESM(s), along with any SPMs and/or SOMs, in each of the five MCH population domains. While there is not an associated NPM in the Cross-cutting/Systems Building domain, the state should report on any state-initiated activities or established SPMs/SOMs that fall within this domain. This discussion will likely build on the high-level presentation in the State Action Plan Narrative Overview and include more detailed descriptions of such Title V program efforts as strengthening family partnerships, addressing social determinants of health, expanding MCH data capacity, enhancing public health surveillance/reporting systems and securing a qualified and well-trained MCH workforce. A state may opt to insert a brief introduction (up to one printed page) prior to the domain-specific narrative discussions, if helpful in providing needed context. However, this introductory section is not required.
The domain-specific State Action Plan narrative discussion should focus on the alignment of the strategies, objectives and performance measures for a corresponding priority need, as outlined in the State Action Plan Table. This discussion should primarily include strategies and activities for which the Title V program has a leadership role in administering the activity. Critical partnerships with other MCHB-supported programs (e.g., MIECHV, MCH Training Programs, Healthy Start programs and CoIINs) should be highlighted, along with family partnerships, in the relevant MCH domain narrative discussions.
For the Annual Report year, the state should:
Provide an analysis that gives context to the state of this population domain;
Summarize programmatic efforts and the use of evidence-based or -informed approaches to address each of the identified priority needs;
Re-assess the alignment of the selected NPMs, ESMs, SPMs and SOMs, if applicable, with its related priority need;
Analyze the state’s progress in achieving its established performance measure targets along with other programmatic impacts;
Note challenges and emerging issues that have resulted in changes to the State Action Plan; and
Assess the overall effectiveness of the implemented program strategies and approaches in addressing the identified MCH population needs and in promoting continuous quality program improvement.
For the Application year, the state should:
Describe the planned activities for the Application year, with ongoing emphasis on their relevance to the identified priority needs;
Align planned activities with the priority needs that were identified based on the Five-Year Needs Assessment and the annual needs assessment updates;
Assess if new priorities have emerged that take precedence over the established priority needs;
Assess the relevance of the current ESM(s) for a selected NPM and determine if a new ESM needs to be established;
Assess if changes are needed in the established SPMs and SOMs, if applicable; and
Discuss updates to the Five-year Action Plan Table that reflect new or revised priority needs, evidence-based or -informed strategies or performance measures for driving improved performance.
The Application/Annual Report should provide a comprehensive understanding of the role of Title V in the state. As such, MCH strategies and activities that reflect ongoing efforts and support the overall system of care for the MCH population but do not directly align with a State’s identified priority needs should be discussed in the relevant MCH domain. For example, State Title V program support for newborn screening and for maternal mortality reviews should be described in the narrative discussion for Perinatal/Infant Health and
Women/Maternal Health, respectively, regardless if there is a related priority need.
In its Application/Annual Report, the state should describe its process for making the Application/Annual Report available to the public for comment during its development and after its transmittal. This discussion should include efforts by the state to solicit public comments during the development of the Application/Annual Report. The number and nature of the comments received and how they were addressed in the final Application/Annual Report should be noted for each year. The state should clearly identify specific activities for engaging families and other stakeholders prior to, during and after the Application process. Such activities may include:
Public Hearings;
Advisory Council Review;
Web Posting;
Social Media;
Public Notices;
Other Use of Media; and
Outreach to Specific Stakeholders (e.g., MCH Training Grantees)
States should describe potential areas of needed technical assistance as they work to implement their five-year Action Plan. In accordance with the responsibilities specified in Section 509 of the Title V legislation, the MCHB makes available to states and jurisdictions needed technical support and resources, as determined by a state. The state must complete and submit a Technical Assistance Request Form to receive MCHB-supported technical assistance. This form is available upon request from the MCHB Project Officer.
1 Institute of Medicine. (1988). The Future of Public Health. Washington, D.C.: National Academy Press.
2 Public Health in America. (1994), Washington, DC: US Public Health Service. Essential Public Health Services Working Group of the Core Public Health Functions Steering Committee.
3 Carman K., Dardess, P., Maurer, M., Sofaer, S., Adams, K., Bechtcl, C., Sweeney, J. “Patient and Family Engagement: A framework for understanding the elements and developing interventions and policies.” Health Affairs. 2013; 32:223-231.
4 Ibid
5 Gabor, V., Noonan, G., Anthony, J. and Gordon, E. “Review of the Title V 5-Year Needs Assessment Process in the States and Jurisdictions.” Final Report, Health Systems Research, Inc. (Altarum), December 15, 2006.
7 A population health strategy for CSHCN intends to improve the health and well-being of an entire group or subgroup. These strategies occur at the policy or systems level and are measurable over time. They are designed to improve health equity and often focus on social and environmental factors. For more information, please visit Appendix I.
8 Wirth, B. and Van Landeghem, K. “Strengthening the Title V-Medicaid Partnership: Strategies to Support the Development of Robust Interagency Agreements between Title V and Medicaid.” April 2017.
http://nashp.org/wp-content/uploads/2017/04/Strengthening-the-Title-V-Updated.pdf.
| File Type | application/vnd.openxmlformats-officedocument.wordprocessingml.document |
| Author | Michele Lawler |
| File Modified | 0000-00-00 |
| File Created | 2021-01-13 |
© 2026 OMB.report | Privacy Policy