Public Comments - 60d FRN
Att 2b Public Comments.docx
National Health Interview Survey
Public Comments - 60d FRN
OMB: 0920-0214
Attachment 2b Public Comments
From: Jean Public <jeanpublic1@yahoo.com> Sent: Monday, August 21, 2017 9:26 AM
To: OMB-Comments (CDC); americanvoices@mail.house.gov; info@njaciv.org; info@taxpayer.net; media@cagw.org; info@njtaxes.org; info@afphq.org
Subject: Re: pubic comment on federal register
regulatoins.gov does not accept comments on this at all. this lousy agency issending the public on a hunt for something that doesnt exist under either number in regulatoins.gov
they do that on purpose so they dont get many public comments. it is part of the ugly plan of this awful agency.
nobody believes the statistics of the cdc. they are manipulated for the fat cat bureaucratic ends of this wasteful agency. they are not honest statitsics. they maniupulate them like with theflu where they call deaths from multiple reasons deaths from flue. they do that so that their big pharma and big medical pals make alot of money pushing vaccines. the lies about vaccines are numerous. nobody at this agency tells the truth about vaccines.
nobody can trus this agency. it needs to be cleane dout with honesty.
also no tapayers hsould be paying for this to be done eery year. it shows no movement when it is done every year. do it every 5 years where it can be watched and utilized.
this every year crap is just wasted american tax dolalrs for dishonest staistics. this comment is for the public record. plese receipt. jean publiee jeanpublic1!gmail.com

October 17, 2017
Leroy A. Richardson
Information Collection Review Office Centers for Disease Control and Prevention 1600 Clifton Road NE.
MS-D74
Atlanta, Georgia 30329
Submitted through the Federal eRulemaking portal
RE: DEPARTMENT OF HEALTH AND HUMAN SERVICES; Centers for Disease
Control and Prevention; Proposed Collection; Comment Request (National Health Interview Survey) (82 F.R. 39586) (Docket No. CDC-2017-0063)
Dear Mr. Richardson:
We are grateful for the opportunity to comment on the National Health Interview Survey (NHIS). We are scholars at the Williams Institute, an academic research center at UCLA School of Law dedicated to conducting rigorous and independent research on sexual orientation and gender identity, including on heath disparities and discrimination facing lesbian, gay, bisexual, and transgender (LGBT) people. Williams Institute scholars have extensive experience in designing and evaluating measures of sexual orientation and gender identity within population- based surveys, and have produced widely-cited best practices.1 Williams Institute scholars have long worked with federal agencies, including the Centers for Disease Control and Prevention and the National Center for Health Statistics, to improve data collection on the U.S. population.
The NHIS is a crucial data collection, because it is a major source of health and wellbeing statistics in the United States, including information about medical conditions, health insurance coverage, and health behaviors. The NHIS data may be classified by sex, age, race, ethnicity, sexual orientation, marital status, family composition, educational level, employment status, health status, and other characteristics. Therefore, the NHIS data provide crucial insight on a wide range of topics relevant to racial and ethnic minorities, women, older and younger people, and other subpopulations in the United States. As the Federal Register notice observes, “NHIS data have long been used by government, academic, and private researchers to evaluate both general health and specific issues, such as smoking, diabetes, health care coverage, and access to health care. The survey is also a leading source of data for the Congressionally- mandated ‘Health US’ and related publications, as well as the single most important source of statistics to track progress toward Departmental health objectives.” 82 F.R. 39586.

1 See Sexual Minority Assessment Research Team, Williams Institute, Best Practices for Asking Questions about Sexual Orientation on Surveys (2009), https://williamsinstitute.law.ucla.edu/wp-content/uploads/SMART-FINAL- Nov-2009.pdf; Gender Identity in U.S. Surveillance Group, Williams Institute, Best Practices for Asking Questions to Identify Transgender and Other Gender Minority Respondents on Population-Based Surveys (2014), https://williamsinstitute.law.ucla.edu/wp-content/uploads/geniuss-report-sep-2014.pdf.
We share a commitment to the development of data-informed policies that promote health and wellbeing for all Americans. In this comment, we address the importance of maintaining the sexual orientation measure on, and adding a transgender-inclusive gender identity measure to, the NHIS. The NHIS’s existing sexual orientation measure enhances, and a gender identity measure would enhance, the quality, utility, and clarity of the information collected, because the sexual orientation measure is providing invaluable data about the health and well-being of LGB people (as compared to non-LGB people) and a gender identity measure would provide crucial information about the nation’s transgender population (as compared to cisgender people). Like other personal demographic data already collected on the NHIS, the sexual orientation data strengthens the ability of the Department, state and local health departments, policymakers, healthcare providers, patients, advocates, and others to address unique issues facing the LGB population. Adding a gender identity measure would extend this capacity to cover transgender populations as well. Existing evidence finds that LGBT people face discrimination in healthcare settings and experience health disparities as compared to their non-LGBT counterparts, making continued inclusion of the sexual orientation measure and the addition of a gender identity measure on the NHIS all the more important.
The NHIS Should Continue to Collect Sexual Orientation Data
Like an increasing number of federal and state surveys,2 the NHIS successfully collects information on respondents’ sexual orientation identity, among other personal demographic information. The continued collection of such data is crucial to the ability to measure and track a wide variety of health indicators and outcomes as they apply to sexual minority populations. For example, researchers from the National Center for Health Statistics have analyzed NHIS data and found that LGB people are more likely to be current cigarette smokers than their straight counterparts; bisexuals report a higher rate of serious psychological distress in the past 30 days than people who identify as straight; and lesbians aged 18 to 64 are more likely to report not obtaining needed medical care in the past year due to cost than their straight counterparts.3 Williams Institute and other researchers have also analyzed the NHIS data stratified by sexual orientation to study, for example, food insecurity and SNAP participation;4 insurance coverage and binge drinking;5 and health indicators for older sexual minorities.6 Continued collection of
2 Federal Interagency Working Group on Improving Measurement of Sexual Orientation and Gender Identity in Federal Surveys, Current Measures of Sexual Orientation and Gender Identity in Federal Surveys (2016), https://s3.amazonaws.com/sitesusa/wp- content/uploads/sites/242/2014/04/WorkingGroupPaper1_CurrentMeasures_08-16.pdf.
3 Brian W. Ward et al., Sexual Orientation and Health Among U.S. Adults: National Health Interview Survey, 2013 NATIONAL HEALTH STATISTICS REPORTS, (2014), https://www.cdc.gov/nchs/data/nhsr/nhsr077.pdf.
4 Taylor N.T. Brown et al., Williams Institute, Food Insecurity and SNAP Participation in the LGBT Community (2016), https://williamsinstitute.law.ucla.edu/wp-content/uploads/Food-Insecurity-and-SNAP-Participation-in-the- LGBT-Community.pdf.
5 Mitchell R. Lunn et al., Sociodemographic Characteristics and Health Outcomes Among Lesbian, Gay, and Bisexual U.S. Adults Using Healthy People 2020 Leading Health Indicators, 4 LGBT HEALTH 283 (2017).
6 Christina N. Dragon et al., “Health indicators for older sexual minorities: National health interview survey, 2013- 2014,” 4 LGBT Health 1 (2017).
2
sexual orientation data on the NHIS will allow researchers to track increases or decreases in disparities between sexual minority and heterosexual populations as well as within subgroups in the LGB community. Such research helps to inform policy making and resource allocation based on the specific needs of these communities.
Measuring Gender Identity on the NHIS Would Enhance the Quality, Utility, and Clarity of the Information Being Collected
We urge the CDC to revise the existing NHIS gender item by adding the two-step approach to measuring gender identity, which would allow researchers to analyze health disparities facing the transgender population. The CDC’s HIV case report, the National Crime Victimization Survey, the California Health Interview Survey, and other population-based surveys have successfully added gender identity questions that measure transgender status, indicating that NHIS could do so as well. The documentation of pervasive discrimination against transgender people in the United States, including in healthcare contexts, makes the NHIS a critical survey for understanding healthcare access, utilization experiences, and the health profile of the transgender population. Thus, adding a transgender-inclusive gender identity measure to the NHIS would enhance the quality and utility of CDC data.
Research has shown that a two-step question format receives high response rates and tends to more accurately identify transgender people than single item question.7 In the two-step format, respondents answer one question about their sex assigned at birth, and a second question about their current gender identity (and are provided a transgender response option or options). The second question allows for the identification of respondents who identify as transgender; the questions together allow for identification of respondents whose sex assigned at birth is different than their gender identity but who do not identify as transgender. Williams Institute scholars would welcome the opportunity to assist the CDC in the development of a two-step gender identity measure on the NHIS.
As scholars who analyze data and are committed to producing reliable estimates, we appreciate that there may be methodological challenges related to the small size of the transgender population. However, the NHIS appears to have a large enough sample to get meaningful data on the transgender population. Moreover, the NHIS could oversample transgender people in order to produce reliable estimates and/or could pool data over several administrations of the NHIS. Furthermore, population-based surveys have shown that younger people are more likely to identify as transgender than older people at every age group.8 This means that as younger generations of transgender people enter adulthood, the size of the
7 David Grant et al., UCLA Center for Health Policy Research, Williams Institute, Putting the ‘T’ in LGBT: A Pilot Test of Questions to Identify Transgender People in the California Health Interview Survey; Sari L. Reisner et al., Monitoring the Health of Transgender and Other Gender Minority Populations: Validity of Natal Sex and Gender Identity Survey Items in a U.S. National Cohort of Young Adults, 14 BMC PUBLIC HEALTH 1224 (2014); Charlotte Chuck Tate et al., A Two-Question Method for Assessing Gender Categories in the Social and Medical Sciences, 50
J. SEX RESEARCH 767 (2013); Kristen Schilt & Jenifer Bratter, From Multiracial to Transgender? Assessing Attitudes toward a Transgender Category on the Census, 2 TRANSGENDER STUDIES QUARTERLY 77 (2015).
8 Jody L. Herman et al., Williams Institute, Age of Individuals Who Identify as Transgender in the United States
(2017), https://williamsinstitute.law.ucla.edu/wp-content/uploads/TransAgeReport.pdf.
3
transgender population identifiable on surveys will likely grow. In sum, it appears that the NHIS could generate useful data that would allow researchers, policymakers, and service providers to assess and address the health needs of transgender Americans.
Conclusion
Collecting sexual orientation and gender identity data on the NHIS would provide useful information about LGBT healthcare access and health status, information that would enhance the ability of the Department to achieve its mission of enhancing the health and well-being of Americans by providing for effective health and human services and by fostering sound, sustained advances in the sciences underlying medicine, public health, and social services. Thank you for your consideration. Please direct any correspondence to romero@law.ucla.edu.
Respectfully Submitted,
Adam P. Romero, JD
Director of Legal Scholarship and Federal Policy, and Arnold D. Kassoy Scholar of Law Williams Institute, UCLA School of Law
M.V. Lee Badgett, PhD Williams Distinguished Scholar
Williams Institute, UCLA School of Law Professor of Economics
University of Massachusetts, Amherst
Kerith J. Conron, ScD
Blachford-Cooper Distinguished Scholar and Research Director
Williams Institute, UCLA School of Law
Andrew Flores, PhD Visiting Scholar
Williams Institute, UCLA School of Law Assistant Professor of Government
Mills College
Amira Hasenbush, JD, MPH
Jim Kepner Law and Policy Fellow Williams Institute, UCLA School of Law
Jody L. Herman, PhD Scholar of Public Policy
Williams Institute, UCLA School of Law
Christy Mallory, JD
Director of State and Local Policy Williams Institute, UCLA School of Law
Ilan H. Meyer, PhD
Williams Distinguished Senior Scholar of Public Policy
Williams Institute, UCLA School of Law
Bianca D.M Wilson, PhD
Rabbi Barbara Zacky Senior Scholar of Public Policy
Williams Institute, UCLA School of Law
4

Name:
Anonymous Anonymous
FDA,
I watched the conference on live stream and came away impressed by what I feel is about to become a reality! You have the capabilities to save the next generations lives and help with nicotine addiction for those battling the habit now. Key points you made were that this is capable as 'Science is the backbone'. I did my research and your science mastermind is 22nd century group! You stated that nicotine was your top priority, so I ask you before 5.6 million children die prematurely from tobacco use directly or indirectly next year and the years to come to implement VLN now. Again, nicotine may not cause the cancer in the cigarette but it causes the addiction that leads to cancer causing deaths due to smoking. Thank you for working tirelessly for my children, your children and the children that don't have a voice.
Sincerely,
An educator for 20 years:)
Name:
Anonymous Anonymous
Dear FDA,
As a Physical Education teacher for 20 years meaning 20x I have done "Just say No to Tobacco" in my school. I came across an article that blew my mind and felt like I needed to write you and thank you. Each year I do statistics of the harm tobacco does to our youth. This year I focused on the addiction side of tobacco/cigarettes and I came across a study that you helped develop with 22nd Century Group,Inc. I can't believe what this can mean for our youth/society. You are changing the world making it healthier for the generations to come. I grew up with second hand smoke can you imagine the innocent lives who don't have a voice yet and you can save now by reducing the nicotine level to 5%!! Why isnt this bringing attention to the media yet? This is life changing and I thank you for creating a safer place for the children who are dealing with second hand smoke, the youth for now they may not become "addicted" and to the elders who maybe wanting to quit now have an alternative solution to stop.
I applaud you!!
Name:
Anonymous Anonymous
FDA,
Thank you for protecting the youth of generations to come. Limiting the nicotine in tobacco is an astonishing achievement that I would never thought to see in my lifetime. 22nd century, inc. science will save the lives of the children starting tomorrow. You hold the key to make this a reality. Science has already proven they can do this, now it is up to you to put it into the law. Please I beg of you to do this sooner rather than later.
Thank you for making tomorrow healthier.


Leroy A. Richardson
Information Collection Review Office Centers for Disease Control and Prevention 1600 Clifton Road NE., MS-D74
Atlanta, Georgia 30329
Friday, October 20, 2017
National Health Interview Survey Questionnaire Redesign Docket No. CDC-2017-0063
Dear Mr. Richardson,
We would like to thank the Centers for Disease Control and Prevention (CDC) for providing this opportunity to offer comments on the proposed National Health Interview Survey (NHIS) redesign. Collecting data on sexual orientation and gender identity is of great importance to us, as researchers and advocates for the LGBT community. The National Health Interview Survey is the federal government’s primary survey of Americans’ health and it plays a significant role in informing public health policy, including policies that impact LGBT communities. The Center for American Progress (CAP) is writing to urge the CDC to include question(s) on gender identity in the NHIS in order to ensure that LGBT health care needs are properly evaluated. We applaud the CDC’s inclusion of a NHIS question collecting sexual orientation data in the annual core content for sample adults and believe those efforts can be expanded. We encourage the inclusion of a question on gender identity and we believe the wording of the sexual orientation question can be improved to elicit more accurate results from bisexual respondents.
CAP is a nonprofit, nonpartisan think tank dedicated to evidence-based public policy that serves the needs of all communities. As a leading expert on data collection and the disparities facing LGBT communities, CAP is well-suited to address the need for increased data collection to identify the issues and unique needs of those communities.
Developing high-quality data that more fully explore and facilitate understanding of LGBT health is essential if federal, state, local, and nongovernmental entities are to adequately and efficiently serve LGBT individuals and their families. The absence of a question on gender identity in federal data collection instruments such as NHIS keeps invisible the experiences of the transgender community and leaves the Federal government blind to its unique needs. Similarly, the current wording of the sexual orientation question could lead some bisexual respondents to unintentionally misreport themselves as straight.
LGBT data collection has become an issue of pressing concern because the current federal administration has shown an intent to abandon it. For example, the U.S. Department of Health and Human Services (HHS) proposed removing LGBT people from two critical surveys back in March, only restoring a sexual orientation question to one survey after a large outcry from the public.1 The Census Bureau continues to exclude sexual orientation and gender identity from
1 Sejal Singh, Laura E. Durso, and Aaron Tax, “The Trump Administration Is Rolling Back Data Collection on LGBT Older Adults,” Center for American Progress, March 20, 2017, available at https://www.americanprogress.org/issues/lgbt/news/2017/03/20/428623/trump- administration-rolling-back-data-collection-lgbt-older-adults/. Center for American Progress, “STATEMENT: Following Widespread Backlash, HHS Reverses Course and Restores Sexual Orientation Question to Key Survey, Says CAP’s Laura E. Durso,” (2017) available at https://www.americanprogress.org/press/statement/2017/06/23/434914/statement-following-widespread-backlash-hhs-reverses-course- restores-sexual-orientation-question-key-survey-says-caps-laura-e-durso/. Agency Information Collection Activities; Submission for OMB Review; Comment Request; Revision of a Currently Approved Collection (ICR Rev); National Survey of Older Americans Act Participants (NSOAAP), 82 Fed. Reg. 28491 (June 22, 2017).

the American Community Survey, despite a clear programmatic need for such data collection.1 Most recently, the Census Bureau planned to remove a sexual orientation question from the 2020 Census Barriers, Attitudes and Motivators Survey, deciding to keep it after drawing attention from advocates and legislators.2 Accurate data collection on sexual orientation and gender identity allows us to understand the specific disparities facing the LGBT community, and sub-populations within it. Understanding disparities allows us to fully and appropriately advocate for specific policy changes to remedy those disparities.
The following are our recommendations to bolster the collection of data regarding sexual orientation and gender identity through the National Health Interview Survey.
The National Health Interview Survey Should Include a Transgender-Inclusive Gender Question
An estimated 1.4 million adults in the US identify as transgender, along with a large number of transgender children and adolescents.3 Several key federal surveys, including the National Crime Victimization Survey (NCVS), National Inmate Survey (NIS), Survey of Prison Inmates (SPI), and National Adult Tobacco Survey (NATS) all use transgender- inclusive measures, and a majority of states in the Behavioral Risk Factor Surveillance System do so as well.4 The Federal Interagency Working Group on Improving Measurement of Sexual Orientation and Gender Identity in Federal Surveys has so far produced working papers cataloguing existing LGBT-inclusive survey questions and evaluations of those questions.5 The NCVS provides perhaps the best example of how the CDC can successfully identify transgender individuals in the NHIS.6 The method used in the NCVS is the well-vetted two-step approach to collecting information about gender identity endorsed by Gender Identity in U.S. Surveillance Group.7 This two-step gender identity question has also been used in the California Health Interview Survey.8
The National Health Interview Survey’s gender question is currently not transgender-inclusive. We recommend that the CDC replace the existing question on sex with a two-part question, asking separately for an individual’s sex assigned at birth (i.e., on their original birth certificate), and how they would currently describe their gender. This question design is already being used in surveys such as the CDC’s HIV case report form, the California Health Interview Survey, and in many electronic health records systems, including those participating in the CMS Meaningful Use of Electronic Health Records Incentive Program.9 Research has shown that this two-part question garners high response rates and is highly accurate in identifying when a person is transgender.10 In addition, the use of a two-part question reduces the likelihood of errors in identifying transgender people within a survey, as evidence shows that transgender individuals are less likely to choose “transgender” when the term is presented alongside other response choices.11
Transgender people experience disparities across multiple areas of our society. According to the 2015 U.S. Transgender Survey, 31% experienced public accommodation discrimination, 20% have participated in the underground economy for income, 23% experienced housing discrimination, and 29% were living in poverty.12 Survey respondents were also four times less likely to own a home and three times more likely to be unemployed compared to the U.S. population.13 It is crucial to properly survey transgender Americans in order to address their unique health needs.
2

The burden on respondents to the NHIS will also be minimal. Studies have found that refusal rates for SOGI questions are actually much lower than refusal rates for questions on income.18 Another recent study at community health centers supports these results, finding that a majority of people agreed that collecting SOGI data is important and will respond to such questions.19 Additional questions to identify transgender people will likely not add significant time to the survey administration process.
The National Health Interview Survey’s Question on Sexual Orientation Should Be Kept, But Amended to Capture Data that Better Reflect the American Public
We are grateful that the NHIS will again include a question about sexual orientation. Retaining that question is very important. There remain, however, some concerns about the efficacy of the question for bisexual respondents, particularly given findings from the 2013 NHIS on the proportion of adults identifying as bisexual which diverge from previous research.20 The diverging findings might result from the response description for “straight” being positioned as being opposed to “gay/lesbian or gay.” Given that several earlier studies have found the majority of LGB people identify as bisexual,21 this categorization, especially as the second option available, may result in some bisexual respondents incorrectly choosing “straight, that is not gay,” because they are not necessarily sure if there will be a “bisexual” category. It also perpetuates the notion that sexuality is a binary between gay/lesbian and straight. The National Survey of Sexual Health and Behavior22 and the California Health Interview Survey currently use questions that do not position “gay/lesbian” and “straight” as opposing.23 In fact, they do not define the terms at all. The National LGBT Health Education Center also recommends not using oppositional definitions in electronic health records.24
Conclusion
Thank you for the opportunity to comment on the proposed NHIS redesign. We are prepared to offer input, guidance, and feedback as the survey moves forward and are excited about increased efforts to collect data on sexual orientation and gender identity.
Sincerely,
Center for American Progress
1 Hansi Lo Wang, “U.S. Census to Leave Sexual Orientation, Gender Identity Questions Off New Surveys,” NPR, March 29, 2017, available at http://www.npr.org/sections/thetwo-way/2017/03/29/521921287/u-s-census-to-leave-sexual-orientation-gender-identity-questions-off-new- surveys. Hansi Lo Wang, “Collecting LGBT Census Data Is ‘Essential’ to Federal Agency, Document Shows,” NPR, June 20, 2017, available at http://www.npr.org/2017/06/20/533542014/collecting-lgbt-census-data-is-essential-to-federal-agency-document-shows.
2 Dan Avery, “US Census Bureau Agrees to Keep Sexual Orientation Question in Upcoming Survey,” New Now Next, September 28, 2017, available at http://www.newnownext.com/us-census-bureau-agrees-to-keep-sexual-orientation-question-in-upcoming-survey/09/2017/. See also U.S. Census Bureau, “U.S. Census Bureau Statement on Asking Sexual Orientation Question On Census Barriers, Attitudes and Motivators Survey,” September 28, 2017, available at https://www.census.gov/newsroom/press-releases/2017/sexual-orientation.html.
3 See Flores, A.R., et al., How Many Adults Identify as Transgender in the United States?, Williams Institute (2016).
4 See Baker & Hughes, Sexual Orientation and Gender Identity Data Collection in the Behavioral Risk Factor Surveillance System, Center for American Progress (2016).
3

4
6 NCVS currently fields the follow following questions: What sex were you assigned at birth, on your original birth certificate? Male, Female, Refused, Don’t Know. Do you currently describe yourself as male, female, or transgender? Male, Female, Transgender, None of these. Federal Interagency Working Group on Improving Measurement of Sexual Orientation and Gender Identity in Federal Surveys, “Current Measures of Sexual Orientation and Gender Identity in Federal Surveys” (August 2016), available at https://s3.amazonaws.com/sitesusa/wp- content/uploads/sites/242/2014/04/WorkingGroupPaper1_CurrentMeasures_08-16.pdf.
7 Survey administrators ask people their sex assigned at birth followed by their current gender identity. See Williams Inst., Best Practices for Asking Questions to Identify Transgender and Other Gender Minorities on Population-based Surveys. Available at http://williamsinstitute.law.ucla.edu/wp-content/uploads/geniuss-report-sep-2014.pdf
8 Regents of the University of California, “California Health Interview Survey 2015,” available at
http://healthpolicy.ucla.edu/chis/design/Documents/CHIS2015AdultQuestionnaire.pdf.
9 See Ctrs. For Disease Control, Adult HIV Confidential Case Report Form, CDC 50.42A (rev. June 2016); 45 C.F.R. §170.207(n)-)(o) (2015); Grant, D., et al., Putting the ‘T’ in LGBT: A pilot test of questions to identify transgender people in the California Health Interview Survey, UCLA Center for Health Policy Research, The Williams Institute, UCLA School of Law, 2015.
10 Grant, et al., Putting the ‘T’ in LGBT: A pilot test of questions to identify transgender people in the California Health Interview Survey. See also Reisner S.L., et al., “Monitoring the health of transgender and other gender minority populations: Validity of natal sex and gender identity survey items in a U.S. national cohort of young adults,” BMC PUBLIC HEALTH, November 26, 2014. See also Tate, C.C., Ledbetter, J.N., & Youssef, C.P., “A Two-Question Method for Assessing Gender Categories in the Social and Medical Sciences,” THE JOURNAL OF SEX RESEARCH, September 18, 2012. In contrast, a one-step question asking about gender identity or transgender status is likely to miss a large number of transgender people who have a gender identity different than the sex they were assigned at birth but either do not describe themselves as transgender or will refuse to choose between being counted as transgender and being counted as a man or woman. See Schilt, K., & Bratter, J. (2015). From Multiracial to Transgender? Assessing Attitudes toward a Transgender Category on the Census, TSQ: THE TRANSGENDER STUDIES QUARTERLY (2015).
11 See Schilt, K., & Bratter, J. (2015). From Multiracial to Transgender? Assessing Attitudes toward a Transgender Category on the Census, TSQ: THE TRANSGENDER STUDIES QUARTERLY (2015).
12 James, S. E., Herman, J. L., Rankin, S., Keisling, M., Mottet, L., & Anafi, M. (2016). Executive Summary of the Report of the 2015 U.S. Transgender Survey. Washington, DC: National Center for Transgender Equality.
13 James, S. E., Herman, J. L., Rankin, S., Keisling, M., Mottet, L., & Anafi, M. (2016). Executive Summary of the Report of the 2015 U.S. Transgender Survey. Washington, DC: National Center for Transgender Equality.
14 Baker, K., Durso, L. E., and Ridings, A., “How to Collect Data About LGBT Communities,” Center for American Progress, March 15, 2016, available at https://www.americanprogress.org/issues/lgbt/reports/2016/03/15/133223/how-to-collect-data-about-lgbt-communities/.
15 Baker, K. and Durso, L. E., “Filling in The Map: The Need for LGBT Data Collection,” September 16, 2015. Washington, DC: Center for American
Progress. Available at https://www.americanprogress.org/issues/lgbt/news/2015/09/16/121128/filling-in-the-map-the-need-for-lgbt-data- collection/.
16 Baker, K., Durso, L. E., and Ridings, A., “How to Collect Data About LGBT Communities,” Center for American Progress, March 15, 2016, available at https://www.americanprogress.org/issues/lgbt/reports/2016/03/15/133223/how-to-collect-data-about-lgbt-communities/.
17 Gender Identity in U.S. Surveillance, “Best Practices for Asking Questions to Identify Transgender and Other Gender Minority Respondents on Population-Based Surveys,” September 2014, available at https://williamsinstitute.law.ucla.edu/wp-content/uploads/geniuss-report-sep- 2014.pdf.
18 Ortman, J. M. et al. (April 2017). Optimizing Self and Proxy Response to Survey Questions on Sexual Orientation and Gender Identity. 2016 Joint Program in Survey Methodology (JPSM) Practicum. Available at http://bit.ly/2vYCmsr. See also VanKim, N. et al. (December 2010). Adding Sexual Orientation to Statewide Public Health Surveillance: New Mexico’s Experience. American Journal of Public Health, 100(12): 2392–2396. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2978164/.
19 Cahill S, Singal R, Grasso C, King D, Mayer K, et al. (2014) Do Ask, Do Tell: High Levels of Acceptability by Patients of Routine Collection of Sexual Orientation and Gender Identity Data in Four Diverse American Community Health Centers. PLoS ONE 9(9): e107104. doi:10.1371/journal.pone.0107104.
20 See Ward et al., (2014). Sexual Orientation and Health Among U.S. Adults: National Health Interview Survey, 2013, National Health Statistics Reports, 77.
21 Movement Advancement Project, Invisible Majority: The Disparities Facing Bisexual People and How to Remedy Them (2016) http://lgbtmap.org/policy-and-issue-analysis/invisible-majority.
22 National Survey of Sexual Health and Behavior (NSSHB), Center for Sexual Health Promotion, School of Health, Physical Education, and Recreation, Indiana University, Bloomington. http://www.nationalsexstudy.indiana.edu/.
23 UCLA Center for Health Policy Research, “CHIS Questionnaires,” available at
http://healthpolicy.ucla.edu/chis/design/Pages/questionnairesEnglish.aspx (last accessed October 19, 2017).
24 Collecting Sexual Orientation and Gender Identity Data in Electronic Health Records, National LGBT Health Education Center, Fenway Institute (2016) http://www.lgbthealtheducation.org/wp-content/uploads/Collecting-Sexual-Orientation-and-Gender-Identity-Data-in-EHRs-2016.pdf.


October 20, 2017
Leroy A. Richardson
Information Collection Review Office Centers for Disease Control and Prevention 1600 Clifton Road NE. MS-D74
Atlanta, Georgia 30329
Submitted through the Federal eRulemaking portal
RE: DEPARTMENT OF HEALTH AND HUMAN SERVICES; Centers for Disease Control and Prevention; Proposed Collection; Comment Request (National Health Interview Survey) (82 F.R. 39586) (Docket No. CDC-2017-0063)
The National Center for Transgender Equality (NCTE) offers these comments on the National Health Interview Survey (NHIS). NCTE was founded in 2003 to advocate for fairness, opportunity, and well- being for transgender people across the United States. In 2015, NCTE conducted the national U.S. Transgender Survey, which identified health and other disparities among more than 27,000 transgender adults in all 50 states, U.S. territories, and U.S. military bases abroad.1 NCTE has long worked with federal agencies, including the CDC and other Department of Health and Human Services components, to improve data collection and inform policy affecting gay, lesbian, bisexual, and transgender (LGBT) Americans.
NHIS data provide crucial insights on the American population and inform funding, policy, and programming decisions across all levels of government and non-government activities related to health and well-being. NHIS data on demographic subgroups of population allows for targeted efforts to address health disparities. Accurate demographic information on LGBT Americans improve—and in the case of transgender people, would improve—the quality, utility, and clarity of NHIS data.
NHIS Should Continue to Collect Sexual Orientation Data
NHIS is one of a growing number of federal and state surveys successfully collecting sexual orientation data using validated measures. NHIS data regarding sexual orientation and health and economic disparities has helped inform the efforts of the Department, states, and local communities to improve health and well-being, and will allow researchers and policymakers to assess the impact of policy and program efforts. We strongly urge CDC to maintain the current sexual orientation measure.
1 James, S. E., Herman, J. L., Rankin, S., Keisling, M., Mottet, L., & Anafi, M. (2016). The Report of the 2015 U.S.
Transgender Survey. Washington, DC: National Center for Transgender Equality.
1133 19th Street NW 202 642 4542
Suite 301 www.TransEquality.org
Washington, DC 20036
Page
2
A Measure of Gender Identity Would Enhance the Quality, Utility, and Clarity of NHIS Data
Scholars have estimated that 1.4 million American adults, and hundreds of thousands of children and adolescents, are transgender.2 A substantial body of research (including the US Transgender Survey) now indicates that transgender Americans face significant social, economic, and health disparities. Yet the absence of gender identity measures in major population-based surveys such as NHIS makes it difficult to generalize data or compare it to general population findings in order to inform policy, program, and funding decisions.
Fortunately, some key population-based surveys have incorporated gender identity measures, and NHIS should do so as well, as these surveys have shown that these measures can be added successfully and allow for important findings about a vulnerable but less well-understood population. Experience has shown that a two-step gender measuring gender assigned at birth and current gender identity performs well in terms of response rates and accuracy and is preferable to a single question. We urge the CDC to work with scholars who study the transgender population to develop a two-step gender measure for NHIS.
Conclusion
The LGBT population are a significant part of the American population and existing research indicates a need for national, population-based data on this population’s life experiences. Collecting data about this population would enhance the ability of the Department, as well as health care providers, programs, and policymakers around the country to achieve the mission of improving population health and well- being.
Thank you for your consideration of these comments. Please contact Director of Policy Harper Jean Tobin, hjtobin@transequality.org, or (202) 804-6047 with any questions.
2 Herman, J.L., Flores, A.R., Brown, T.N.T., Wilson, B.D.M., & Conron, K.J. (2017). Age of Individuals who Identify as Transgender in the United States. Los Angeles, CA: The Williams Institute.

October 20, 2017
Centers for Disease Control and Prevention (CDC), Department of Health and Human Services (HHS) Docket No. CDC-2017-0063
National Health Interview Survey (NHIS) (OMB Control No. 0920-0124, Exp. 12/31/2019)—Revision— National Center for Health Statistics (NCHS), Centers for Disease Control and Prevention (CDC)
Statement of Interest
Services and Advocacy for Gay, Lesbian, Bisexual and Transgender Elders (“SAGE”) is the country’s oldest and largest organization dedicated to improving the lives of lesbian, gay, bisexual, and transgender (“LGBT”) older adults. In conjunction with 28 affiliates in 21 states, SAGE offers supportive services and consumer resources to LGBT older adults and their caregivers, advocates for public policy changes that address the needs of LGBT older people, and provides training for agencies and organizations that serve LGBT older adults.
Pursuant to a grant from the Department of Health and Human Services’ Administration for Community Living (ACL), SAGE – in collaboration with 18 leading organizations nationwide – operates the National Resource Center on LGBT Aging (NRC), which is the country’s first and only technical assistance resource center aimed at improving the quality of services and supports offered to LGBT older adults. The NRC provides training, technical assistance, and educational resources to aging providers, LGBT organizations, and LGBT older adults. To date, the NRC has trained 15,745 professionals, representing 1,968 aging organizations located in every State and the District of Columbia. In addition, the NRC has published, and made widely available, best practice guides, including Inclusive Questions for Older Adults: A Practical Guide to Collecting Data on Sexual Orientation and Gender Identity.
SAGE hereby submits these comments in response to the Notice that the Department of Health and Human Services’ (HHS) Centers for Disease Control and Prevention (CDC) published in the Federal Register on August 21, 2017. In the Notice, the CDC seeks comments regarding the National Health Interview Survey (NHIS). The annual National Health Interview Survey is a major source of general statistics on the health of the U.S. population.
LGBT Older Adults Have a Heightened Risk of Greatest Social and Economic Need
HHS’s Administration for Community Living (ACL) has previously recognized that LGBT older adults are at particular risk of greatest social need. Indeed, in 2012, ACL’s Administration on Aging (AoA) stated that older LGBT individuals may be among the populations with “greatest social need” because “in some communities . . . isolation due to sexual orientation or gender identity may restrict a person’s ability to
perform normal daily tasks or live independently.”1 Indeed, LGBT older adults have a heightened risk of greatest economic and social need. As many as four million American adults age 60 and over identify as LGBT.2 As a group, LGBT older adults have poorer physical and mental health outcomes than other older adults.3 At the same time, many LGBT older adults have weaker social support systems than their contemporaries.4 LGBT older adults also have higher rates of poverty than other older adults.5
As a Group, LGBT Older Adults are More Likely to Have Physical and Mental Health Disabilities than Other Older Adults
Poorer physical health. LGBT people – and especially LGBT older adults – tend to be in poorer physical health than their peers. Studies have found that there are “higher rates of diabetes, hypertension [and] disability . . . among aging gay men, lesbians, and bisexual people than among older straight adults.”6 Other “[s]tudies suggest higher levels of chronic and other health problems among LGBT older adults, including asthma, diabetes, HIV/AIDS, obesity, rheumatoid arthritis, and certain illnesses such as cancer.”7
HIV/AIDS has had a disproportionate effect on the LGBT community. Thirty-five years after it was first recognized, “[t]he HIV epidemic . . . continues to have a lasting impact on the older generation physically, emotionally, and psychologically.”8 The Centers for Disease Control has estimated that one-quarter of
1 AoA made this statement in a response to a Frequently Asked Question. The AoA FAQ response is available at https://aoa.acl.gov/aoa_programs/oaa/resources/Faqs.aspx#State.
2 Soon Kyu Choi and Ilan H. Meyer, LGBT Aging: A Review of Research Finds, Needs, and Policy Implications 2 (Williams Inst. Aug. 2016), available at http://williamsinstitute.law.ucla.edu/wp-content/uploads/LGBT-Aging- White-Paper.pdf (“Williams LGBT Aging Report”) (citing Administration on Aging, U.S. Department of Health and Human Services, Administration for Community Living, Lesbian, Gay, Bisexual and Transgender (LGBT) (2014), available at www.aoa.acl.gov/AoA_Programs/Tools_Resources/diversity.aspx#LGBT)).
3 Id. at 24 (citing Fredriksen-Goldsen, K.I., Kim, H-J., Barkan, S.E., Muraco, A., Hoy-Ellis, C.P., American Journal of Public Health 103(10), Health Disparities Among Lesbian, Gay, and Bisexual Older Adults: Results from a Population-Based Study 1802-1809 (2013)); Addis, S., Davies, M., Greene, G., MacBride-Stewart, S., & Shepherd, M., Health and Social Care in the Community 17(6), The Health, Social Care, and Housing Needs of Lesbian, Gay, Bisexual and Transgender Older People: A Review of the Literature 647-658 (2009); Fredriksen-Goldsen, K. I., Kim, H.-J., Emlet, C. A., Muraco, A., Erosheva, E. A., Hoy-Ellis, C.P., Goldsen, J., Petry, H., Seattle: Institute for Multigenerational Health, The Aging and Health Report: Disparities and Resilience Among Lesbian, Gay, Bisexual, and Transgender Older Adults (2011)).
4 Williams LGBT Aging Report, supra n.2, at 8 (citing LGBT Movement Advancement Project & Services and Advocacy for Gay, Lesbian, Bisexual and Transgender Elders (MAP & SAGE), Improving the Lives of LGBT Older Adults (2010), available at www.lgbtmap.org/file/improving-the-lives-of-lgbt-older-adults.pdf; Barker, J.C., Herdt, G., & de Vries, B., Sexuality Research & Social Policy: Journal of NSRC. 3(2), Social Support in the Lives of Lesbians and Gay Men at Midlife and Later 1–23 (2006)).
5 Id. at 10 (citing Goldberg, N.G.; The Williams Institute, The Impact of Inequality for Same-Sex Partners in Employer-Sponsored Retirement Plans (2009); LGBT Movement Advancement Project & Services and Advocacy for Gay, Lesbian, Bisexual and Transgender Elders (MAP & SAGE), Improving the Lives of LGBT Older Adults (2010), available at www.lgbtmap.org/file/improving-the-lives-of-lgbt-older-adults.pdf).
6 Erin Fitzgerald, No Golden Years at the End of the Rainbow, Nat’l Gay & Lesbian Task Force, 12 (Aug. 2013),
available at www.thetaskforce.org/static_html/downloads/reports/reports/no_golden_years.pdf.
7 Movement Advancement Project (MAP), et al., LGBT Older Adults And Health Disparities, 2 (Sept. 2010),
available at www.lgbtmap.org/file/lgbt-older-adults-and-health-disparities.pdf.
8 Williams LGBT Aging Report, supra n.2, at 27 (citing Friend, R. A., Journal of Homosexuality, 20(3-4), Older Lesbian and Gay People: A Theory of Successful Aging, 99-118 (1991); Emlet, C.A., Fredriksen-Goldsen, K.I, Kim,
those living with HIV in the United States are over 55.9 Another study found that nine percent of the LGBT older adults surveyed were living with HIV, and that HIV rates are higher for African Americans and Hispanic LGBT older adults than other LGBT older adults.10
Worse mental health outcomes. As a group, LGBT people – and especially LGBT older adults – also “have worse mental health outcomes than their heterosexual counterparts.”11 Indeed, according to one study, LGBT people are three times more likely than other people to have a mental health problem during their lifetime.12 This reflects the fact that LGBT people have endured “stressors and challenges not experienced by heterosexuals,” such as discrimination, rejection, difficulty accepting their sexual orientation, and the need to conceal their orientation from others.13
LGBT Older Adults are More Likely to Face Cultural, Social or
Geographic Isolation
Scholarly studies have shown that “[i]solation and fear of loneliness are major concerns of LGBT older individuals.”14 In one study, nearly 60 percent of the LGBT older adults “reported feeling a lack of companionship, and over 50 percent reported feeling isolated from others.15 Another study found that 32 percent of LGBT older adults reported being very or extremely concerned about “being lonely and growing old alone,” compared to 19 percent of non-LGBT older adults.16
Perhaps the most significant reason why LGBT older adults have a heightened risk of isolation is the fact that they often do not have as strong a social support network as their peers. As people age, many come to rely increasingly on family members, especially spouses and children, for assistance with medical and financial matters. Prior to 2003, no State allowed same-sex couples to marry, and it took another twelve years until the Supreme Court struck down the remaining State prohibitions. As a result, LGBT individuals are less likely to be married than heterosexuals. Roughly 16 percent of LGBT adults are currently married
H., & Hoy-Ellis, C., Journal of Applied Gerontology, The Relationship Between Sexual Minority Stigma and Sexual Health Risk Behaviors Among HIV-Positive Older Gay and Bisexual Men 1-22 (2015).
9 Centers for Disease Control and Prevention, HIV Among People 50 and Over, available at
www.cdc.gov/hiv/group/age/olderamericans/index.html.
10 Williams LGBT Aging Report, supra n.2, at 27 (citing Fredriksen-Goldsen, K. I., Kim, H.-J., Emlet, C. A., Muraco, A., Erosheva, E. A., Hoy-Ellis, C.P., Goldsen, J., Petry, H., Seattle: Institute for Multigenerational Health, The Aging and Health Report: Disparities and Resilience among Lesbian, Gay, Bisexual, and Transgender Older Adults (2011)).
11 Richard Wright, Am. J. of Public Health 103(2), Same-Sex Legal Marriage and Psychological Well-Being: Findings From the California Health Interview Survey, 339 (Feb. 2013).
12 National Alliance on Mental Illness, Find Support, LGBTQ, available at www.nami.org/Find-Support/LGBTQ.
13 Richard Wright, Am. J. of Public Health, Same-Sex Legal Marriage and Psychological Well-Being, supra n.11, at 339.
14 Id. at 6 (citing Fredriksen-Goldsen, K. I., Kim, H.-J., Emlet, C. A., Muraco, A., Erosheva, E. A., Hoy-Ellis, C.P., Goldsen, J., Petry, H., Seattle Institute for Multigenerational Health, The Aging and Health Report: Disparities and Resilience Among Lesbian, Gay, Bisexual, and Transgender Older Adults (2011)).
15 Id.
16 SAGE, Out and Visible: The Experiences and Attitudes of Lesbian, Gay, Bisexual and Transgender Older Adults, Ages 45-75, 12, available at www.sageusa.org/files/LGBT_OAMarketResearch_Rpt.pdf.
compared to about 50 percent of adults in the general public.17 Further, many States permit restrictions on the ability of LGBT people to adopt.18 In addition, many LGBT elders remain estranged from their families of origin.19 Consequently, LGBT elders are twice as likely to live alone, half as likely to have close relatives to call for help, and four times less likely to have children to assist them.20
LGBT Older Adults are More Likely to Have Incomes at or Below the Poverty Line
Contrary to popular belief, LGBT people – especially LGBT older adults – are underrepresented at the top of the income pyramid and over-represented at the bottom.21 One study reported that 15.9 percent of single gay men over 65 lived in poverty, compared to just 9.7 percent of single heterosexual men their age.22 While older LGBT couples are less likely to live in poverty than LGBT singles, they are still more likely to be poor than their heterosexual peers. For example, 6.0 percent of lesbian couples 65 years of age and older have incomes below the poverty line, compared to 3.5 percent of heterosexual married couples in the same age group.23
The Need for Transgender Data is Especially Great
The need to collect data on transgender older adults is especially great. Based on what limited data we do have, we know that transgender older adults are even more likely than other LGBT older adults to: suffer from physical disabilities and poor mental health; face cultural, social or geographic isolation; and have an income level at or below the poverty line. At the same time, for transgender older adults, the shortage of culturally competent providers and fear of discrimination are especially acute. As a result, transgender older adults are at a particularly high risk of not receiving the services and supports that they need to live independently. By having more data, we can learn more about the challenges transgender older adults face, and we can find a way to address them.
17 Id. at 6 (citing Pew Research Center, A Survey of LGBT Americans: Attitudes, Experiences and Values in Changing Times (2013), available at www.pewsocialtrends.org/2013/06/13/a-survey-of-lgbtamericans/).
18 Movement Advancement Project (MAP), Foster and Adoption Laws, available at www.lgbtmap.org/equality- maps/foster_and_adoption_laws.
19 Williams LGBT Aging Report, supra n.2, at 6 (citing Movement Advancement Project, et al., Improving the Lives of Older Adults, 6-7 (Mar. 2010)).
20 See Movement Advancement Project (MAP), Improving the Lives of Older Adults, 6-7 (2010), available at www.lgbtmap.org/file/improving-the-lives-of-lgbt-older-adults.pdf. In one study, nearly one-quarter of LGBT older adults reported that they had “no one” to rely on when they are ill. See Still Out, Still Aging The MetLife Study of Lesbian, Gay, Bisexual, and Transgender Baby Boomers, at 15 (Mar. 2010), available at www.metlife.com/assets/cao/mmi/publications/studies/2010/mmi-still-out-still-aging.pdf; see also SAGE, Out and Visible: The Experiences and Attitudes of Lesbian, Gay, Bisexual and Transgender Older Adults, Ages 45-75, supra n.16, at 17-18 (collecting statistics comparing isolation experienced by LGBT and non-LGBT older adults).
21 Gary J. Gates and Frank Newport, GALLUP, Special Report 3.4% of U.S. Adults Identify as LGBT, 2 (Oct. 12, 2012), available at www.gallup.com/poll/158066/special-report-adults-identify-lgbt.aspx (35 percent of LGBT adults had annual incomes under $24,000, compared to 24 percent of the total adult population; 16 percent of LGBT adults earned more than $90,000 a year, compared to 21 percent of the general population).
22 M.V. Lee Badgett, et al., Williams Inst. 9-10, New Patterns of Poverty in the Lesbian, Gay and Bisexual Community (June 2013) available at http://williamsinstitute.law.ucla.edu/research/census-lgbt-demographics- studies/lgbt-poverty-update-june-2013/.
23 Id. at 15.
Transgender Older Adults Have an Especially High Risk of Greatest Social and Economic Need
Transgender older adults are even more likely than other LGBT older adults to have physical and mental health disabilities
Poorer physical health. Transgender older adults have an even higher risk than other LGBT older adults of poor physical health and disability.24 Transgender women, in particular, have a high prevalence of HIV, which not only presents health challenges, but also increases their difficulty finding social support, and creates additional barriers to care.25
Worse mental health outcomes. Transgender older adults also report even higher rates of psychological distress and depression,26 and are even more likely to have suicidal thoughts,27 than other LGBT older adults. These poor mental health outcomes reflect the victimization, discrimination, lack of support, and stigma associated with gender non-conformity.28
Transgender older adults are even more likely than other LGBT older adults to face cultural, social or geographic isolation
While all LGBT older adults face a heightened risk of cultural or social isolation, transgender older adults are especially at risk. Transgender older adults are even less likely than other LGBT older adults to have support networks comprised of friends, family, and children – the networks on which many other older adults rely on as they age. For instance, only 35 percent of transgender women age 50 and over are married or partnered, compared to 50 percent of lesbians in the same age group.29
The process of “transitioning” one's gender presentation and/or sex characteristics to align with a gender identity that differs from the one assigned at birth often leads to significant social isolation. Twenty percent of transgender older adults above the age of 65 report having a spouse or partner end the relationship with them because of their transgender identity.30 At the same time, many mental health professionals continue to advise married transgender people, as part of their transition plan, to divorce
24 Williams LGBT Aging Report, supra n.2, at 3.
25 Id. at 27-28; Movement Advancement Project (MAP) and Services and Advocacy for LGBT Elders (SAGE), Understanding Issues Facing LGBT Older Adults, at 15 (2017), available at http://www.lgbtmap.org/file/understanding-issues-facing-lgbt-older-adults.pdf.
26 Williams LGBT Aging Report, supra n.2, at 3, 15.
27 Id. at 3.
28 Id. at 27.
29 Movement Advancement Project (MAP) and Services and Advocacy for LGBT Elders (SAGE), Understanding Issues Facing LGBT Older Adults, at 12 (2017), available at http://www.lgbtmap.org/file/understanding-issues- facing-lgbt-older-adults.pdf.
30 National Center for Transgender Equality 2015 U.S. Transgender Survey, available at
their spouse, move to a new area, and/or construct a new identity that fits with the person’s changed gender identity,31 thereby compounding social isolation.32
Transgender older adults are even more likely than other LGBT older adults to have incomes at or below the poverty line
Transgender older adults are even more likely than other LGBT older adults to have incomes near or below the poverty line. Indeed, while 26 percent of LGBT older adults ages 65 and older live at or below 200 percent of the federal poverty level, this percentage rises to 48 percent for transgender older adults.33 Transgender individuals also report high rates of unemployment and low wages.34 This reflects the particular challenges that many transgender people face in areas of such as employment, housing, and education.35
Transgender older adults are even less likely than other LGBT older adults to receive the services and supports that they need to live independently
Transgender older adults not only have an especially high risk of greatest social and economic need, but they also are especially unlikely to receive the services and supports they need to live independently. This reflects both the especially acute shortage of culturally competent providers able to meet the specialized needs of transgender older adults and the especially great fear of discrimination faced by this population.
Transgender elders have especially great difficulty finding culturally competent providers
Many transgender older adults report experiencing “a lack of culturally competent health services.”36 Transgender people generally face particular challenges because “many health providers ‘may lack knowledge about transgender and intersex anatomy . . . .’”37 Moreover, transgender older adults often need different types of support and expertise, such as transition-related medical care, than other LGBT older adults.38 Older adults who transition later in life face added health challenges in accessing care and
31 Williams LGBT Aging Report, supra n.2, at 6.
32 Richard Wright, Am. J. of Public Health, Same-Sex Legal Marriage and Psychological Well-Being, supra n.11, at 339.
33 Movement Advancement Project (MAP) and Services and Advocacy for LGBT Elders (SAGE), Understanding Issues Facing LGBT Older Adults, at 10 (2017), available at http://www.lgbtmap.org/file/understanding-issues- facing-lgbt-older-adults.pdf.
34 Williams LGBT Aging Report, supra n.2, at 10.
35 See Williams Institute, Best Practices for Asking Questions to Identify Transgender and Other Gender Minorities on Population-based Surveys, at 1 (2014), available at http://williamsinstitute.law.ucla.edu/wp- content/uploads/geniuss-report-sep-2014.pdf
36 SAGE, Out and Visible: The Experiences and Attitudes of Lesbian, Gay, Bisexual and Transgender Older Adults, Ages 45-75, at 13, available at www.sageusa.org/files/LGBT_OAMarketResearch_Rpt.pdf.
37 Movement Advancement Project (MAP), Improving the Lives of LGBT Older Adults, at 35 (2010) (quoting Public Advocate for the City of New York, Improving Lesbian, Gay, Bisexual and Transgender Access to Health Care at New York City Health and Hospitals Corporation Facilities (2008)), available at www.lgbtmap.org/file/improving- the-lives-of-lgbt-older-adults.pdf.
38 Williams LGBT Aging Report, supra n.2, at 3.
support.39 For example, because older adults have often developed chronic medical conditions, including high blood pressure and cardiovascular disease, gender reassignment surgeries are riskier, and could exacerbate their preexisting conditions.40
Fear of discrimination is especially likely to deter many transgender older adults from accessing healthcare and using available services
Transgender older adults are even more likely than other LGBT older adults to be deterred from obtaining the services and supports they need due to fear of discrimination.41 For example, while 20 percent of LGBT older adults between the ages of 45 and 75 fear that their relationships with healthcare providers (including hospital or nursing home staff) would be adversely affected if their sexual orientation were known, 44 percent of transgender older adults fear that disclosing their gender identity would impair their relationship with their healthcare providers.42
The fear that many transgender older adults experience is compounded by the fact that, unlike their other LGBT counterparts, many transgender individuals do not have the option to conceal their sexual minority status from health professionals, as their body may reveal scars or other evidence of their gender identity.43 Because of this, transgender individuals are more susceptible to discrimination and abuse by health professionals. This is especially true for transgender older adults, who seek more frequent and intimate healthcare due to age-related physical conditions and disabilities.44 The fear of discrimination that many transgender older adults experience is often well-founded.45 Over one-third of transgender older adults have reported experiencing discriminatory events such as the denial of healthcare.46
Less Data is Available About Transgender Older Adults Than About Other LGBT Older Adults
Despite the especially great need that many transgender older adults experience, research about this population is limited.47 Transgender older adults are absent from many of the relevant studies that have been conducted about the LGBT community. Moreover, those studies that do include transgender older
39 Movement Advancement Project (MAP) and Services and Advocacy for LGBT Elders (SAGE), Understanding Issues Facing LGBT Older Adults, at 4 (2017), available at http://www.lgbtmap.org/file/understanding-issues- facing-lgbt-older-adults.pdf.
40 Carina Storrs, CNN, Gender transitioning for seniors has unique challenges (June 3, 2015), available at
http://www.cnn.com/2015/06/03/health/senior-gender-transition/index.html.
41 Williams LGBT Aging Report, supra n.2, at 1.
42 Movement Advancement Project (MAP) and Services and Advocacy for LGBT Elders (SAGE), Understanding Issues Facing LGBT Older Adults, at 19 (2017), available at http://www.lgbtmap.org/file/understanding-issues- facing-lgbt-older-adults.pdf.
43 Williams LGBT Aging Report, supra n.2, at 8.
44 Id.
45 Movement Advancement Project (MAP) and Services and Advocacy for LGBT Elders (SAGE), Understanding Issues Facing LGBT Older Adults, at 18 (2017), available at http://www.lgbtmap.org/file/understanding-issues- facing-lgbt-older-adults.pdf.
46 Williams LGBT Aging Report, supra n.2, at 14.
47 Id. at 3.
adults use small sample sizes and focus their analysis on measures that are applicable to all LGBT older adults.48
The NHIS Should Collect Data on Sexual Orientation and Gender Identity; Models Exist for Transgender-Inclusive Data Collection at the Federal Level
As outlined above, LGBT older adults face numerous barriers to successful aging. The more we know about these challenges, the more we can do to address them. The current iteration of the NHIS collects much needed data on sexual orientation. It fails, however, to collect data on gender identity. SAGE urges the CDC to begin collecting much needed data on gender identity in the NHIS.
The CDC has a unique opportunity to improve the quality of its data collection efforts by collecting gender identity data. 49 There are a number of ways in which the CDC could fulfill this obligation. One possibility would be to adopt the sexual orientation and gender question currently contained in the Behavioral Risk Factor Surveillance System (“BRFSS”), which the CDC, in coordination with HHS, already conducts.50
The text of the BRFSS module reads as follows:
CDC-approved
SOGI module for BRFSS The
next two questions are about sexual orientation and gender identity. Do
you consider yourself to be: Straight Lesbian
or gay Bisexual Other Don’t
know/Not
sure Refused
Do you consider yourself to be transgender?
Yes,
Transgender,
male-to-female Yes,
Transgender,
female-to-male Yes,
Transgender, gender
non-conforming
48 Id.at 33-34.
49 OMB has previously recognized that “Attempts to measure both sexual orientation and gender identity with one question or a series of questions tend to conflate the concepts and reduce resulting information quality. These two concepts are distinct as should be measured separately.” Federal Interagency Working Group on Improving Measurement of Sexual Orientation and Gender Identity in Federal Surveys, Current Measures of Sexual Orientation and Gender Identity in Federal Surveys at 17 (Aug. 2016) (“available at https://s3.amazonaws.com/sitesusa/wp-content/uploads/sites/242/2014/04/current_measures_20160812.pdf..
50 See generally www.cdc.gov/brfss/ (providing information about the BRFSS).
No
Don’t know/not sure
Refused
The approach in the BRFSS survey is far superior to the one originally included in the NHIS because it asks all respondents – not just those who described their sexual orientation as “something else” – about their gender identity, while significantly reducing the number of gender identity choices by focusing on the most significant categories.
The BRFSS questions have been used extensively. The CDC developed the questions in 2013 and, in 2014, gave states the option of adding them to their BRFSS questionnaires. Twenty-five states and territories used the module in 2015.51 An additional thirty States have chosen to use a variant of the CDC-developed question in their BRFSS questionnaires.52 “States that have used this module report that it is well-received by respondents and does not negatively affect the quality of data collected.”53 For example, Missouri State BRFSS Coordinator Janet Wilson noted that the State’s use of this module in its 2015 survey “did not result in any survey break-off and had very low rates of item nonresponse.”54
The CDC can also benefit from the significant efforts that have been made to improve the methods used to collect gender identity information in recent years. Over time, a consensus has developed that the best method to collect this data is the so-called “two-step” method. This method involves a question regarding one’s sex assigned at birth, followed by a question about one’s current gender identity:
51 Center for American Progress, Sexual Orientation and Gender Identity Data Collection in the Behavioral Risk Factor Surveillance System, 1-2 (2016), available at www.americanprogress.org/issues/lgbt/report/2016/03/29/134182/sexual-orientation-and-gender-identity-data- collection-in-the-behavioral-risk-factor-surveillance-system/.
52 For example, the 2013 Massachusetts sexual orientation and gender identity module for the BRFSS includes the following question:
Some people describe themselves as transgender when they experience a different gender identity from their sex at birth. For example, a person born into a male body, but who feels female or lives as a woman. Do you consider yourself to be transgender? Yes, transgender, male to female; Yes, transgender, female to male; Yes, transgender, gender non-conforming; or No.
Williams Institute, Best Practices for Asking Questions to Identify Transgender and Other Gender Minorities on Population-based Surveys. Available at http://williamsinstitute.law.ucla.edu/wp-content/uploads/geniuss-report-sep- 2014.pdf
53 Id. at 6.
54 Id. At least two other federal surveys have successfully collected gender identity information from respondents. The Youth Risk Behavior Surveillance System (“YRBS”), which is the youth corollary of the BRFSS, includes a gender identity measure. See Williams Institute, Best Practices for Asking Questions to Identify Transgender and Other Gender Minorities on Population-based Surveys, at 5 (2014), available at http://williamsinstitute.law.ucla.edu/wp-content/uploads/geniuss-report-sep-2014.pdf. In addition, the National Inmate Survey (“NIS”), which collects provide more detailed information regarding sexual victimization in jails and prisons, includes a question designed to identify transgender respondents. See id. at 6.
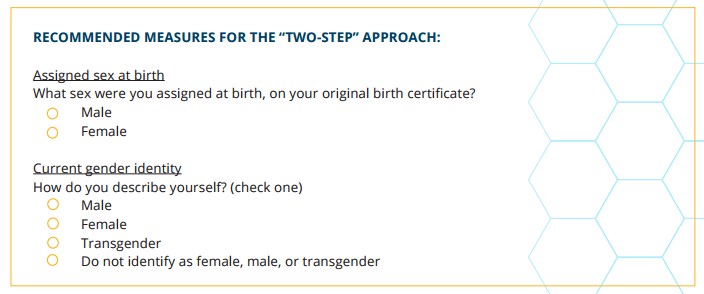
The two-step approach is able to more accurately identify transgender respondents than a single, stand- alone gender identity item with a transgender response option (e.g., male, female, or transgender) because some transgender individuals identify their gender as male or female rather than transgender and, thus, would be missed if a gender identity measure was used alone.55
Whatever approach the CDC selects should, of course, be evaluated and, if necessary, further refined in order to ensure that the data collection is as effective as possible while imposing the least burden necessary to achieve its intended purpose.
Conclusion
Given the health challenges faced by LGBT older adults and especially transgender older adults; the great risk of greatest social and economic need faced by LGBT older adults and transgender older adults in particular; the great risk that LGBT older adults and especially transgender older adults will not access the services and supports they need to live independently; and most importantly, the paucity of data about LGBT older adults and transgender older adults in particular, the need to collect data about both sexual orientation and gender identity in the NHIS is especially great
Including a single (or even two-step) gender identity questions would not increase the agency’s burden in any measurable degree. SAGE and the ACL-funded National Resource Center on LGBT Aging are prepared to work with the CDC to further improve the process for collecting data to help insure that we learn more about and are therefore better able to meet the needs of older adults, including transgender older adults.
55 See Williams Institute, Best Practices for Asking Questions to Identify Transgender and Other Gender Minorities on Population-based Surveys, at 9, 16 (2014), available at http://williamsinstitute.law.ucla.edu/wp- content/uploads/geniuss-report-sep-2014.pdf.
| File Type | application/vnd.openxmlformats-officedocument.wordprocessingml.document |
| File Title | Microsoft Word - Williams Institute NHIS Comment 2017-10-17 |
| Author | Romero |
| File Modified | 0000-00-00 |
| File Created | 2021-01-21 |
© 2026 OMB.report | Privacy Policy