SSA CASPER Final
SSA CASPER Final.docx
Community Assessment for Public Health Emergency Response (CASPER)
OMB: 0920-1036
Community Assessment for Public Health Emergency Response (CASPER)
OMB Control No. 0920-1036 (Expiration Date: 12/17/2017)
Revision
Supporting Statement Part A –
Justification
Amy Helene Schnall
Title: Epidemiologist
Phone: 770.488.3422
Email: GHU5@cdc.gov
Fax: 770.488.3450
Date: October 3, 2017
Table of Contents
A.1. Circumstances Making the Collection of Information Necessary 1
A.2. Purpose and Use of the Information Collection 6
A.3. Use of Improved Information Technology and Burden Reduction 9
A.4. Efforts to Identify Duplication and Use of Similar Information 9
A.5. Impact on Small Businesses or Other Small Entities 10
A.6. Consequences of Collecting the Information Less Frequently 10
A.7. Special Circumstances Relating to the Guidelines of 5 CFR 1320.5 11
A.9. Explanation of Any Payment or Gift to Respondents 14
A.10. Protection of the Privacy and Confidentiality of Information Provided by Respondents 14
A.11. Institutional Review Board (IRB) and Justification for Sensitive Questions 19
A.12. Estimates of Annualized Burden Hours and Costs 19
A.13. Estimates of Other Total Annual Cost Burden to Respondents and Record Keepers 21
A.14. Annualized Cost to the Federal Government 21
A.15. Explanation for Program Changes or Adjustments 21
A.16. Plans for Tabulation and Publication and Project Time Schedule 22
A.17. Reason(s) Display of OMB Expiration Date is Inappropriate 23
A.18. Exceptions to Certification for Paperwork Reduction Act Submissions 23
Goal of the study: Under
this generic clearance, NCEH conducts Community Assessments for
Public Health Emergency Response (CASPERs) to assess current or
emerging community needs during a disaster.
Intended use of the
resulting data: The
CASPER enables public health practitioners and emergency management
officials to rapidly determine the health status and basic needs of
communities affected by a disaster or public health emergency. In
the past three years, NCEH has completed two CASPERs under the
current generic clearance, OMB Control No. 0920-1036 (expiration
date 12/17/2017).
Using data collected under
this generic clearance information collection request, emergency
response officials are able to prioritize response activities and
make informed decisions regarding the distribution of resources.
Results of the CASPER are used to recommend actions.
Methods to be used to
collect: A
cluster sampling methodology is used, which involves a 2-stage
sampling procedure. The first stage includes a sample of 30
clusters (census blocks), with probability proportional to the
estimated number of households. In the second stage, seven
households are selected systematically in each of the 30 clusters.
This methodology provides estimates for the population, including
the proportion and number of persons with specific needs.
Subpopulation to be
studied: The
subpopulation includes residents of a household that is within the
community or geographic area of interest that is being assessed.
The respondent universe for a CASPER is comprised of any member of
a household within the chosen geographic area of interest who is
aged 18 years of older.
How data will be
analyzed: CASPER
uses weighted frequencies with 95% confidence intervals to account
for the two-stage cluster sampling method.
The Centers for Disease Control and Prevention (CDC) is requesting revision of a currently approved Generic Information Collection Request (ICR), Community Assessment for Public Health Emergency Response (CASPER) (OMB No. 0920-1036). This request is for three years and includes changes that result in a decrease in requested burden. The changes are as follows:
Decrease in number of proposed annual CASPERs, from 15 CASPERs to 6 CASPERs annually. Each CASPER will consist of 214 respondents (210 households, or respondents, for CASPER questionnaire and 4 respondents for referral forms).
Decrease in number of total annual respondents from 3,200 to 1,284, resulting in burden reduction of 946 hours.
Respondent costs are being updated to reflect current wage data from 2015.
The total reduction in burden requested for this revision is 946 hours. The total burden requested for this Generic ICR is 631 hours from 1,284 respondents.
A.1. Circumstances Making the Collection of Information Necessary
CDC is seeking Office of Management and Budget (OMB) approval for a revision of a currently approved generic clearance titled Community Assessment for Public Health Emergency Response (CASPER). The previously OMB-approved generic information collection request (OMB No. 0920-1036) is set to expire 12/17/2017. The purpose of this generic clearance is to facilitate the use of CASPER to quickly provide low-cost, household-based information about a community’s perceived needs in a simple, easy-to-understand format to requesting state and local agencies during a disaster or emergency. In an emergency situation, it is often more useful for local health officials and emergency responders to have immediate feedback on perceived needs than it is to wait for more precise characterizations of actual health conditions, access limitations, and infrastructure problems.
The law authorizing data collection using CASPER is Section 301 of the Public Health Service Act (42 U.S.C. 241) (Attachment A). The 60-day Federal Register Notice is provided as Attachment B.
Background
HSB Disaster-related Expertise
Important areas of expertise within Health Studies Branch (HSB), National Center for Environmental Health (NCEH), Centers for Disease Control and Prevention (CDC), are disaster epidemiology and disaster response in all four phases of a disaster (preparedness, response, recovery, mitigation). Our role is often to gather knowledge about the community as it progresses through these four disaster phases. Both natural (e.g., tornado, earthquake, hurricane, drought) and man-made (e.g., chemical spill, radiation event) disasters are environmental. Disasters destroy homes and damage local infrastructure such as the water distribution systems, power production and distribution systems, and health facilities. Disasters also interrupt services and social support networks, thus negatively affecting community well-being. A number of public health issues may arise from exposure to the environmental impacts of a disaster. For example, morbidity and mortality results from exposure to chemicals, flood waters, falling debris, and structure collapse.1,2
Following disasters or other public health emergencies, public health and emergency management professionals must be prepared to quickly identify and meet the needs of the affected community. To mitigate negative health consequences and respond appropriately, these professionals need timely and accurate information.
What is a CASPER?
CASPER is a public health tool (i.e., one of the many options that a public health professional can use to gather information) originally developed by the World Health Organization (WHO) and adapted by HSB for use in preparing for, responding to, and recovering from disasters. The purpose is to quickly gather information about the current situation and assess a community’s needs by conducting a survey of a representative sample of the community. CASPER’s method to identify the community’s perceived needs and infrastructure status during all phases of a disaster has been validated via use and review by epidemiologists and statisticians from WHO and CDC over the last few decades.3,4 Reviewers concluded that the CASPER method provides critical information needed to allow emergency response officials to prioritize emergency response activities and make informed decisions regarding the distribution of resources.
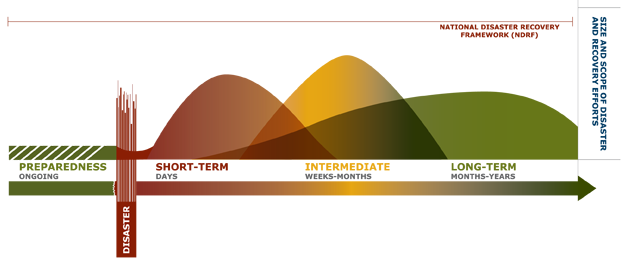
Each time a CASPER is conducted, it is tailored to the current needs of public health and, if appropriate, emergency managers. For example, during disaster preparedness, a CASPER may be used to assess whether people are prepared to remain at home for a prolonged period by having sufficient emergency supplies available. During disaster response, a CASPER may be conducted to assess whether people have electricity or whether people are receiving and understanding critical public health messages. The results of CASPER surveys are shared through the local public health or incident command structure with a wide variety of professionals, including city planners, emergency medical personnel, public health officials, and engineers. HSB developed the CASPER toolkit to explain what a CASPER is and to standardize the process for conducting one. The CASPER toolkit can be found on the web and is freely available for use by state and local jurisdictions (see http://www.cdc.gov/nceh/hsb/disaster/casper/default.htm). In this Generic ICR, we focus only on CASPERS done in the context of an emergency disaster response and recovery; CASPERS designed only for capacity building, preparedness, and post-event evaluations are not covered in this generic ICR. Urgent public health needs can occur both in the response and short- and intermediate-term recovery phases of a disaster (see figure below).5 The recovery phase of a disaster involves moving the community back toward normal functioning. Recovery is immediate and overlaps with response. It includes actions such as providing essential public health and safety services, restoring interrupted utility and other essential services, reestablishing transportation routes, and providing food and shelter for those displaced by the incident.6
Figure A.1.1. The Recovery Continuum
What are the objectives of a CASPER done during an emergency disaster response?
In the disaster setting, the main objectives of CASPER are to
determine the perceived health needs and assess the immediate infrastructure impact of the disaster (e.g., characterizing the availability of public utilities and sanitation services for the population) and
characterize the population residing in the affected area (e.g., assessing basic demographic characteristics such as age, ethnicity, sex, and number of households with pregnant women).
Who can request a CASPER?
At the request of a state, local, tribal, or territorial government agency (SLTT) or an international health authority, HSB will conduct a CASPER to assess current or emerging community needs during a disaster emergency response and recovery. This does not require a federally- or state-declared disaster; this only requires an official request from the public health authority of an SLTT or an international health authority. Domestic CASPERs will follow prescribed Incident Command System (ICS) or Incident Management Structure (IMS) procedures described below. CASPERs conducted internationally, such as the CASPER conducted for the Turkey Earthquake in 1999, will be managed through the CDC emergency operations center and follow prescribed IMS for CDC staff.7, 8 The jurisdiction will determine the level of CDC’s involvement and the particular objectives of the CASPER they would like to conduct.
How does a CASPER fit in to the overall emergency disaster response?
HSB will assist with a CASPER when requested by a state or other Public Health Partner. HSB’s CASPER surveys will only collect information that is not available from other disaster response entities. The notice that HSB has been invited by a state to conduct a CASPER will be shared by our public health contact (e.g., the State Epidemiologist) with other agencies responding to the event through the ICS or IMS – entities activated by the emergency management coordinating agency in the affected state. The ICS and IMS are designed to promote efficient communication and integration across responding entities.9 A liaison officer will act as the point of contact for agency representatives, including the state health official requesting a CASPER, and will track assisting and cooperating agencies, and aid in setting up interagency contacts.9 The individual filling this role will change from event to event. For more information please see the following site: http://training.fema.gov/EMIWeb/IS/ICSResource/assets/reviewMaterials.pdf. HSB will work through the requesting state agency if contact with any other entities active in the disaster is required.
How is HSB involved in CASPER surveys?
HSB developed the CASPER toolkit as a guidance document for use by external partners. The toolkit provides options on the best method available for conducting CASPERs. Sometimes, CDC provides technical assistance with sampling methodologies or questionnaire development and is not involved in data collection. In these cases, CDC does not receive the data nor do we request to keep the data. Thus for these types of technical assistance requests, OMB approval would not be required. In other cases, CDC employees are deployed to the field to assist in some or all of the operations of the CASPER, including interviewing household members. This is considered a sponsored project in the context of the Paperwork Reduction Act (PRA).
A.2. Purpose and Use of the Information Collection
Information collected through CASPER questionnaires and their corresponding reports is designed to be used by public health department personnel, emergency management officials, academia, or other entities with responsibility for disaster response that must rapidly assess household-level public health needs.
The information collected characterizes the population residing in the affected area and is not intended for use outside of that local area nor to inform activities in other areas. CDC may also provide recommendations to state or local decision makers, but ultimately it is the state or local jurisdiction’s decision to act on the recommendations presented. CDC also plans to analyze the data collected during the CASPERs that are federally sponsored to provide insight into how disaster related emergencies affect communities and to assess community preparedness.
It is important for the information collected to be applicable specifically for the affected jurisdiction. Negative impacts of not conducting CASPER include not having information to understand and take action to address immediate community needs during disaster-related emergencies.
The information collected during a CASPER meets the a priori objectives determined by the requesting public health entity. Information is gathered to identify the community’s perceived needs and infrastructure status during the response or recovery phase of a disaster. Depending on the objectives, information can be collected in the following categories: demographic characteristics and functional needs; housing damage and repair; general utilities; carbon monoxide exposure; animal safety; supplies, relief, and emergency preparedness; health status; medical care and prescriptions; and communications. For more detail please see Table A-10.1. Household-level information that may be collected using a CASPER survey in section A.10.1. Privacy Impact Assessment Information.
Since receiving OMB approval for the CASPER Generic ICR (OMB No. 0920-1036, Expiration Date: 12/17/2017), HSB has conducted two CASPERs with OMB PRA approval, which are described below.
Flood-Related CASPER, WV 2016:
In response to extensive flooding in West Virginia on July 23, 2016, which resulted in 23 deaths, the West Virginia Department of Health and Human Resources (DHHR), Bureau for Public Health (BPH) requested assistance from CDC to conduct two CASPERs. BPH selected two of the most severely affected communities in regard to loss of property and human life: Clendenin (Kanawha County) and Rainelle (Greenbrier County). The two assessments collected household level data five weeks after the flood in a sample that was representative of the whole community and results were analyzed separately for comparison to one another. The goal of the CASPERs was to assess household disaster preparedness, access to health care, health impacts due to flood damage, health information sources, and stage of disaster recovery. The CASPERs identified that household disaster preparedness could be improved in both communities by increasing the proportion of households with an evacuation plan and food and water stored in an easily accessible place. Results also showed that hypertension and asthma/chronic obstructive pulmonary disease (COPD) were the most frequently reported chronic diseases that worsened after the flood; those households reporting mold were associated with a three-fold to six-fold increase in the risk of reporting a member with worsening asthma/COPD. CASPER data also demonstrated that, although intended to be received by the entire population of both communities, approximately half (46% in Clendenin, 50% in Rainelle) of households did not receive boil water advisory notices. Recommendations were provided to BPH decision makers to implement flood response and recovery strategies that focus on planning and health risk reduction after a disaster. Lessons learned from the CASPER questionnaire (e.g., which questions worked well) and field activities (e.g., interview team successes) were noted by CDC to be incorporated into future information collections under the CASPER Generic ICR in a flood response or other disaster response or recovery activity. For example, we had modified the water source questions from a previous CASPER and found these modifications to be more effective and clearly understood by respondents. Additionally, we adjusted the timing of interview collection to start later in the afternoon (i.e., at 3pm rather than 1pm) to maximize response rates and decrease field team fatigue. This resulted in less actual field data collection time, while maintaining, and even improving, response rates. West Virginia undertook a series of public health actions following completion of this CASPER, including the following:
Created a roster of disaster epidemiology volunteers identified during the CASPER that will be maintained by the Center for Threat Preparedness
Planned a disaster epidemiology training in Morgantown, WV for April 2017
Developed an updated mass immunization plan
Discussed creating an updated disaster health communications plan
CASPER addressing the California Drought, Mariposa County, 2016:
The second CASPER conducted under the CASPER Generic ICR to date was in Northern California in response to the ongoing emergency of the most severe drought in recorded history. Drought can have a substantial impact on the economy, the environment, and the affected communities, leading to both direct and indirect public health consequences. In November 2015, the Mariposa County Health Department (MCHD) and California Department of Health (CDPH) conducted a CASPER in Mariposa County, CA to address multiple knowledge gaps about the impact of drought on households. To aid in ongoing response efforts, MCHD and CDPH requested assistance from the CDC in October 2016 to conduct a second CASPER to assess the continued effects of drought on Mariposa County households. The CASPER specifically assessed the following: 1) communication practices and preferences for disseminating drought related information to the community; 2) sources, quality, quantity, and ease of access to water before and during drought; 3) prevalence of behaviors that can make households more at-risk for drought-related health effects; 4) household knowledge, attitudes, and beliefs about drought and its mitigation; 5) community’s perception of the impact of drought on physical and mental health; and 6) financial impact of drought, including costs associated with loss of trees resulting in dead tree removal. CASPER data indicated that households reported engaging in water conservation behaviors in response to water shortages, with 86% reducing water usage. However, 36% of households reported washing hands less or for a shorter amount of time, which is of public health concern. Based on the CASPER findings, we suggested the following recommendations for consideration:
Continue outreach efforts to inform residents of Mariposa County’s Dry Well Program. Consider new routes of outreach.
Continue promotion of proper hygienic practices, especially regarding hand-washing behaviors.
Consider expanding mental health services to serve those under acute stress from the drought or drought-related consequences.
Identify households that may be eligible for dead tree removal assistance.
Consider a follow-up CASPER assessment focusing on tree mortality to determine the extent of the burden on the community, including a regional collaboration and involvement from the existing Tree Mortality Task Force.
Consider multiple media outlets for Mariposa County’s planned communications during acute disasters and events that may cause widespread and/or prolonged power outages.
The CASPER was a successful collaboration between CDPH, MCHD, and CDC which helped characterize the impacts of drought in Mariposa County as well as actions households have taken. These results were useful in allocating resources for response to the drought and in strengthening the emergency preparedness capacity of Mariposa County. Lessons learned from the CASPER questionnaire (e.g., which questions worked well) and field activities (e.g., interview team successes) were noted by CDC to be incorporated into future information collections under the CASPER Generic ICR in a drought response or other disaster response or recovery activity. For example, there was confusion in the timeframe of some questions as they were unclear or inconsistent. Therefore, we have noted these questions and have modified them for future use.
A.3. Use of Improved Information Technology and Burden Reduction
CASPER interviews are conducted in person and there are two options for data collection: paper forms and handheld electronic devices. Both the paper and the electronic formats have their advantages and disadvantages; therefore, it is important to carefully consider both options prior to making a decision and developing the questionnaire. Generally, while the paper forms can be labor-intensive in the data entry process, the electronic format can be labor-intensive in the development stage. In addition, electronic forms may be more resource intensive to conduct.
To reduce burden on the participant, CASPER questionnaires are generally limited to two pages. In general, yes/no and multiple choice questions are used to capture the needed information more efficiently. While the CASPER questionnaire is usually completed using pen and paper, there may be instances where the surveys may be completed using CDC-approved electronic devices, such as digital pens. Digital pens are encrypted and the databases that information is entered into are password protected. State and local CASPER partners may own other electronic equipment that can range in type (e.g., various handheld devices). Use of these devices is up to the local jurisdiction conducting the CASPER. The responses potentially collected via electronic equipment are currently approximated at 1% of all CASPERs conducted. Referral forms that contain personally identifiable information (PII) will not be collected using electronic devices.
Regardless of how information is collected, data is analyzed with CDC-approved software, such as Epi Info 7TM. Epi Info 7TM is publically available statistical software that stores data in a Microsoft Access Database file (http://wwwn.cdc.gov/epiinfo/). Data is stored as a flat file and the databases are password protected.
A.4. Efforts to Identify Duplication and Use of Similar Information
The purpose of CASPER is to assess the health status and needs of a community at the household level and to provide information specific to the event being addressed at that time. While there may be health information known about an area before a disaster or public health threat occurs, a community’s perceived needs will be directly affected by a disaster-related emergency event. As a result, CDC and its partners may decide to conduct CASPERs to assess the changing situation by collecting data that are immediately relevant to the emergency. Without this event-specific information on the community, public health officials cannot respond to the most current community needs.
It is important to note that CASPERs are unique data collection events. CASPERs are used to assess current needs of community members. By contrast, the Federal Emergency Management Agency (FEMA) formerly conducted rapid needs assessment (RNAs) as part of their disaster emergency response activities.10, 11 FEMA’s RNAs focus on high level key infrastructure assessments (e.g., hospitals, bridges, emergency operation centers) to assist in determining Federal involvement and funding in a disaster/emergency. These assessments are done by FEMA’s Incident Management Assistance Team (IMAT).12Different from a FEMA RNA or IMAT, CASPER focuses on assessing household-level public health needs (e.g., household access to utilities, generator use/exposure to carbon monoxide, receipt and understanding of public health communications). CDC does not consult with FEMA before conducting a CASPER. CASPERs are done at the request of our SLTT partners, who then coordinate with other agencies that may be responding to the same disaster-related emergencies.
A.5. Impact on Small Businesses or Other Small Entities
No small businesses will be involved in CASPER data collection.
A.6. Consequences of Collecting the Information Less Frequently
The purpose of this request for a revision of a currently approved generic clearance information collection request, Community Assessment for Public Health Emergency Response (CASPER) (OMB No. 0920-1036), is to ensure the collection of data that provides valuable, time-sensitive information on critical health needs and impacts of an event; characterize the affected population; provide primarily household-based information to decision-makers; and potentially to use this information after the event to assess the effectiveness of relief efforts. These data are not otherwise available prior to a disaster or other event occurring. Without this data, public health officials may make decisions based on anecdotal information; such decisions may not accurately reflect the perceived needs of the entire community.
A majority of CASPERs are one-time assessments related to a specific event. Respondents will most likely never have to report information more than once. If follow up studies are conducted in the community (under separate PRA clearances or by local organizations), efforts will be made to minimize the extent to which the same individuals are contacted (See Section B.2 for more information on the sampling methodology).
There are no legal obstacles to reducing the burden.
A.7. Special Circumstances Relating to the Guidelines of 5 CFR 1320.5
There are no special circumstances with this information collection package. This request fully complies with the regulation 5 CFR 1320.5.
This ICR only covers CASPERs requested by SLTTs or an international health authority under emergency situations (e.g., hurricane response, oil spill, drought, flood). A strength of the CASPER tool is its ability to be quickly initiated and conducted once a state has requested CDC assistance in the field.
Figure A.7.1 and A.7.2 below are examples of past response timelines for disaster/emergency CASPERs. In both instances CDC teams were conducting CASPER surveys within 48-96 hours of a formal request for assistance from states. Necessary changes to sampling frames and data collection instruments took place 12-24 hours before data collection began.
Figure A.7.1. CASPER response timeline for Hurricane Ivan, 2004

Figure
A.7.2. CASPER response timeline for Kentucky Ice Storm, 2009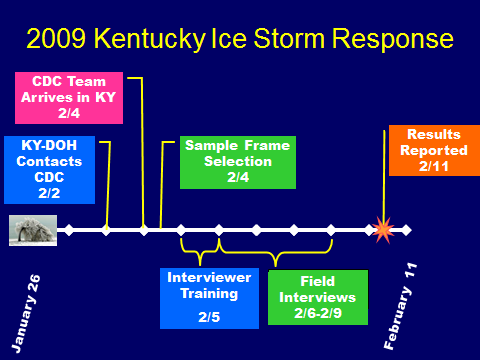
The time critical nature of CDC’s response to these situations can be addressed through the use of this generic OMB submission, under which individual CASPER generic information collections (GenICs) can be submitted for expedited review and approval. To facilitate effective and timely response to public health events, CASPERs often need to be initiated within hours or days of the request. Because of the need to rapidly obtain information to appropriately respond to the urgent public health need, data collection will usually be completed within 180 days.
To ensure that public health data are collected in a timely manner as necessary to protect the health of the public, CASPERs will adhere to the following timeline and processes:
At the request of a SLTT or international health authority, NCEH decides to organize and deploy a team to conduct or assist with a CASPER.
The OMB Desk officer is notified of the CASPER immediately via e-mail from CDC.
Draft data collection instrument(s), a letter of invitation from an SLTT or international health authority (sensitive information in the Letter of Invitation not appropriate for public dissemination should be redacted prior to sending), and the Generic ICR “Request for Approval under Generic Clearance for CASPER” form (Attachment G) describing the problem and the planned response will be submitted to OMB.
CDC staff may deploy to the field and begin planning the CASPER and finalize the collection instrument based on the requesting organization’s CASPER objectives before the request is submitted to OMB. Once the data collection instrument has been finalized, CDC will submit the final version to OMB.
The OMB desk officer responds with approval or comments on the proposed CASPER within 5 days of receipt of the final data collection instrument, unless the request is for a shorter time frame (i.e., 24 or 72 hours). If a 24- or 72-hour approval is requested, an explanation must be provided as to why it is needed. Specifically, CDC must make a case as to why collection must begin within 24 to 72 hours, and it must be related to a public health need. Data collection cannot begin until OMB has approved the information collection request. OMB may provide approval and comments orally (followed by e-mail for written documentation) or e-mail directly to CDC. This may occur before the GenIC request is submitted and received by OMB through the official ICR tracking system.
At the completion of the CASPER, the investigators submit the final data collection instrument(s) and associated burden using the “Burden Memo” form (Attachment H) to the Information Collection Request Liaison (ICRL).
CDC maintains a library of data collection instruments that includes all final data collection instruments conducted under this generic ICR. This library and the updated burden numbers based on data collected via the “Burden Memo” (Attachment H) submitted to OMB quarterly as a non-substantive change to the generic ICR.
A CDC staff person serves in the role of CASPER ICRL. The ICRL oversees the clearance process for individual GenICs. Information about the Generic ICR and how to submit a Generic IC is distributed to CDC program officials (Attachment I). The ICRL maintains a library of data collection forms that may be accessed by CDC programs initiating new CASPERs. Upon the completion of a CASPER, the ICRL places the data collection instruments into the library.
Each CASPER request is closely reviewed by the ICRL. The “Request for Approval under Generic Clearance for CASPER” form (Attachment G) serves as the GenIC package for each individual CASPER investigation.
A.8. Comments in Response to the Federal Register Notice and Efforts to Consult Outside the Agency
The 60-day Federal Register Notice was published in the Federal Register on May 31, 2017, Vol. 82, No. 103, pp. 24973–75 (See Attachment B). CDC did not receive public comments related to this notice.
CDC partners with professional SLTT organizations such as the Council for State and Territorial Epidemiologists (CSTE), and national groups, such as the CDC Disaster Epidemiology Community of Practice (DECoP). The CDC DECoP includes internal and external partners to ensure that the collection requests under Gen ICRs are not in conflict with collections they have or will have in the field within the same timeframe.
Below is a list of individuals outside the NCEH who were consulted to obtain their views on the availability of data, the clarity of instructions and information, and the completeness of the material.
David Zane, MS
Epidemiologist,
Epidemiology and Disease Surveillance Unit
Epidemiology and
Public Health Preparedness Division
Austin Public Health
Jennifer A. Horney, PhD, MPH, CPH
Associate Professor, Department of Epidemiology and Biostatistics
School of Public Health, Texas A&M Health Sciences Center
A.9. Explanation of Any Payment or Gift to Respondents
CDC will not provide payments or gifts to respondents.
A.10. Protection of the Privacy and Confidentiality of Information Provided by Respondents
The NCEH/ATSDR Information Systems Security Officer and the NCEH/ATSDR PRA Contact reviewed this submission on September 27, 2017 and determined that the Privacy Act does not apply. Although CDC is collecting information in identifiable form (IIF) on the referral form, that information is not stored, retained, or entered into any database; it is immediately handed over to the local health jurisdiction to address any immediate needs of the individual during the emergency and will never be collected or store electronically. Identifiable information will not be stored, filed, or retrieved by CDC.
An overview of the data collection system
Supporting Statements A and B outline CDC’s standard procedures for conducting CASPERs. The goal during a standard CASPER is to complete 210 interviews within the assessment area. To provide the basis for sufficiently accurate population estimates, the interviews must be conducted according to an appropriate sampling method. The multistage-stage cluster sampling design used in CASPER provides a representative sample of households within the sampling frame that will allow the generation of sufficiently accurate population estimates during data analysis (further described in Supporting Statement B).
CASPER questionnaires gather information through in-person interviews with one adult (≥18 years of age) from each household identified through the cluster sampling procedure. The particular adult in any given household would be chosen based on whether they are able to communicate fluently with the interviewer, are present at the home when he/she is approached, and are willing to be interviewed. Questionnaire responses are recorded on a paper or electronic form by the interviewer. In general, interviews take approximately 30 minutes and consist of two-page questionnaires. The majority of the time information on the CASPER questionnaire is collected at the household level, meaning that the respondent is answering questions for the household, not just for her- or himself.
Table A-10.1. Household-level information that may be collected using a CASPER survey
Information Collection Categories |
Examples of Needed Information |
Demographic and functional needs (See example CASPER questions provided in the CASPER Toolkit – use of these questions is optional)* |
Age, sex, race, ethnicity |
Housing damage and repair (See example CASPER questions provided in the CASPER Toolkit – use of these questions is optional) |
Home physically safe for habitation, presence of mold, presence of floodwater |
General utilities (See example CASPER questions provided in the CASPER Toolkit – use of these questions is optional) |
Access to running water, gas, electricity, garbage pickup |
Carbon monoxide exposure (See example CASPER questions provided in the CASPER Toolkit – use of these questions is optional) |
Generator use, working carbon monoxide detector |
Animal safety (See example CASPER questions provided in the CASPER Toolkit – use of these questions is optional) |
Exposure to mosquitoes or wild animals, animal bites |
Supplies, relief, and emergency preparedness (See example CASPER questions provided in the CASPER Toolkit – use of these questions is optional) |
Adequate drinking water, adequate food, first aid supplies |
Health status (See example CASPER questions provided in the CASPER Toolkit – use of these questions is optional) |
Physical injuries, mental or behavioral health issues, illness (e.g., fever, diarrhea, vomiting) |
Medical care and prescriptions (See example CASPER questions provided in the CASPER Toolkit – use of these questions is optional) |
Access to medical care, need for urgent care, access to prescription medication |
Communications (See example CASPER questions provided in the CASPER Toolkit – use of these questions is optional) |
Receipt of warnings, reliable sources of information, mode of communication |
* Demographic characteristics, such as sex, age, race and ethnicity, etc., assist public health and emergency responders in understanding the makeup of the population affected. This allows for the determination of specific risk factors and social vulnerabilities and a more tailored response. For example if you found there was a large non-English speaking Hispanic population, translation of your public health communications into Spanish would be appropriate. It is very typical for any epidemiology study or assessment to collect demographics.13
While CASPER questionnaires primarily collect household-level information, there may be instances where the questionnaires are modified to collect information on the individual level. In this circumstance, the adult who is interviewed regarding household-level information is also asked individual-level questions. This adult would be chosen the same way adults are chosen for household-level interviews. Categories of individual level information include the following:
Demographics
Personal needs (e.g., first aid, food, water, ice, and medicine)
Physical and behavioral health status
Perception of and response to public health communications
See Attachment C for sample CASPER questionnaire. These are examples of questionnaires used for CASPERs conducted in the past. There is a list of example questions in the CASPER Toolkit (http://www.cdc.gov/nceh/hsb/disaster/casper/default.htm) which provides guidance on what questions to ask and how they can be asked.
A description of the information to be collected
Tracking forms
Tracking forms are used by interview teams to record households approached (Attachment D). This form is used to document if a chosen household was successfully interviewed, needs to be revisited because there was no one present to complete an interview, or was never interviewed and the reason for non-interview [abandoned, not approachable (aggressive dog, no trespassing sign)]. This information never includes a complete mailing address (e.g., house number, street name, city, state, and zip code) or GPS coordinate information. Information used to identify households for return visits is never retained by CDC or entered into any database. The tracking forms do not contain direct PII. Descriptive information of households is only recorded if a household must be revisited (e.g., no one answered the door after first try). In rare cases, 210 households may be a large portion of some communities thus even without direct PII, the location of a household could be identifiable; however, it is not possible to link the tracking form from a given household to that household’s questionnaire. Only teams working within a cluster will have access to this information, and any descriptive information beyond access, type of dwelling, damage, whether door was answered, and whether interview was conducted is not recorded. All tracking forms are destroyed after data collection and entry is complete. Information regarding number of households approached, number of interviews completed, and reasons for not completing an interview at a household from these forms will be entered into an Excel file on a CDC password-protected computer.
Referral forms
To protect privacy, PII is rarely collected. The few instances where PII may be collected are in situations where households are identified during the CASPER to have urgent, life-threatening needs. In these instances, PII is collected on separate referral forms (Attachment E) which are immediately transferred to a local coordinator (e.g., local public health staff). A local coordinator uses the information on the referral form to rapidly follow-up with the participant and to communicate with health service providers in the area or response agencies to address any immediate needs. The referral form and the information contained in it is never retained by the CDC or entered into any database. The forms will be given immediately to the local jurisdiction. There is no way to link specific questionnaires to any PII that may be collected. Field teams are trained in the handling of referral forms during a training conducted in advance or the morning of the first day of data collection in the field. This training helps to ensure that interviewers properly handle and safeguard any information collected, minimizing the possibility of unauthorized access, use, or dissemination.
A description of how the information will be shared and for what purpose
After the data is analyzed by CDC, the results of the CASPER are shared in two main ways: a preliminary report or presentation provided to key stakeholders within a day or two after data collection and a cleared final report that may be more widely distributed at a later time (Attachment F). Reports of CASPER results are distributed by the requesting state or local public health officials. Politicians occasionally sit in on exit presentation that CDC presents to the state public health officials, and CDC sometimes receives information requests directly from Congress (e.g., progress reports on CASPERs currently being conducted and results from or questions about CASPERs previously conducted). We always consider the media a potential audience. The state often releases the information publicly, and CDC often receives questions directly from the media after the information is released.
Reports only present responses in aggregate form and there is no way to identify households or individuals from reported information or data sets. The report results from CASPER questionnaires are shared to prompt public health action (e.g., prioritization of resources or public health interventions) in response to the current health status or needs of the population affected by the disaster-related emergency.
We intend to share CASPER results by presenting at professional conferences and by publishing manuscripts in peer-reviewed journals. This is a common practice in public health; responses to outbreaks, isolated cases, and emergency responses are often published as they provide lessons learned and examples for others in public health.
A referral form may be used when an interview team identifies households with urgent needs that present an immediate threat to life or health. These forms are given immediately to the local jurisdiction, will not be entered into any CDC database, and will not be in custody of CDC after collection. Further, there is no direct identifier that links either the tracking forms or referral forms back to a specific household’s questionnaire answers.
A statement detailing the impact the proposed collection will have on the respondent’s privacy
When a person is asked if they would like to participate in a CASPER interview, they are informed that the survey is voluntary and anonymous and that they can refuse to answer any of the questions or refuse to participate at any time. We do not gather PII.
Whether individuals are informed that providing the information is voluntary or mandatory
Participation in a CASPER interview is voluntary. In an introductory script, the interviewer will provide the following information:
A description of any anticipated discomfort or inconvenience to the respondent, particularly if some questions may be of a sensitive nature (e.g., race and ethnicity, mental health, pregnancy, or disability).
An explanation that the questionnaire is anonymous and will not be linked to PII.
A statement that taking part in the study is voluntary and that there will be no penalty or loss of benefits if household members do not wish to participate and that they can stop participating at any time with no penalty.
Name and phone number or e-mail of the person(s) a resident can contact if s/he has any questions about the CASPER or would like to verify interview team identification.
A clear participation request or invitation that requires an explicit answer.
Opportunities to consent, if any, to sharing and submission of information
Participants must give explicit verbal consent before a questionnaire is administered. Signed consent is not required for a CASPER because obtaining signatures leads to an increased privacy risk for the participant (i.e., the signed consent would be a link from the participant to the questionnaire). See Attachment J for sample CASPER introduction and consent language.
How the information will be secured
Responses to CASPER questionnaires will be entered into an Epi Info 7TM database (data is stored in a Microsoft Access Database file) and stored on a CDC-approved, encrypted, password-protected computer. The project computers will be kept in locked offices and access to the study data will be password-protected. All electronic data will be maintained by CDC. Data will not include any identifiers. Statistical data analysis and interpretation will be provided by CDC using Epi Info or SAS. Hardcopies of the recorded responses on questionnaires will be given to the local jurisdiction and will not be brought back to CDC Atlanta.
All records are subject to the CDC Comprehensive Record Control Schedule (CRCS), B-371, which contains authorized disposition instructions for CDC’s administrative and program records. CDC is legally required to maintain its program-related records in accordance with disposition instructions contained in this comprehensive records control schedule. These retention periods have a direct impact on completing Freedom of Information Act requests and in applying the requirements of the Privacy Act.
Whether a system of records is being created under the Privacy Act
For the initial 2014 PRA clearance and for the current Generic ICR request, it was determined that the Privacy Act does not apply to this information collection. PII is never stored or retained by the CDC, and a System of Records is not required for this generic clearance.
IRB Approval
Disaster CASPERs are a non-research activity, as they are conducted as part of local public health response or recovery activities for the purposes of informing local public health action. All CASPER Gen ICs will be submitted for a research determination and the determination will be made on a case-by-case basis.
A.11. Institutional Review Board (IRB) and Justification for Sensitive Questions
We will submit appropriate documentation within the individual generic information collection packages for each CASPER to OMB for approval. See Attachment C for an example of CASPER questionnaires. Sometimes, information that can be considered of a sensitive nature (e.g., race and ethnicity, mental health, pregnancy, or disability) may be included in CASPER questionnaires if they can help provide a clearer understanding of what the population being assessed needs and thus help decision makers respond appropriately to the situation at hand.15-19 States may request that we collect information on how a disaster has impacted their communities in regard to specific issues, such as mental and behavioral health issues, so they can provide information and resources if they find there is a need. Questions regarding physical health issues, such as those inquiring if any household members may be blind or deaf, can help to better understand specialized outreach or communication methods that may be needed in that community.
A.12. Estimates of Annualized Burden Hours and Costs
Estimates of Annualized Burden Hours
CDC estimates that it will conduct an average of six emergency CASPERs per year, generally interviewing 210 households (the respondents) per CASPER for a total of 1260 households per year. Additionally, four referral forms (see section A.10.) will be completed for each CASPER for a total of 24 referral forms per year (6 CASPERs x 4 referral forms per CASPER). The referral form is used to collect information from individuals in households with urgent, life-threatening needs during the emergency. The referral form is then given immediately to the local jurisdiction to address the individual’s immediate needs and the information contained within the form is never retained by the CDC or entered into any database. The total number of annual respondents is 1284.
Each household interview is estimated to require 30 minutes, which includes time to give an introduction, obtain consent, and administer the questionnaire. The estimates in Table A-12.1 are based on previous CASPERs conducted in the past three years under the current Generic ICR (OMB No. 0920-1036; expiration 12/17/2017). The respondent universe is described further in Supporting Statement B, section B.1. The total estimated annual burden hours are 631, or 1893 hours over three years. The total estimated number of responses over the three-year period is 3852.
Table A-12.1 Estimated Annualized Burden Hours
Type of Respondents |
Form Name |
No. of Respondents |
No. of Responses per Respondent |
Average Burden per Response (in hours) |
Total Burden (in hours) |
Households in the selected geographic area to be assessed |
CASPER Questionnaire |
1,260 |
1 |
30/60 |
630
|
Referral Form |
24 |
1 |
2/60 |
1 |
|
Total |
631 |
||||
Annualized Cost to Respondents
The average national hourly salary is assumed for all respondents, based on the Department of Labor May 2015 National Occupational Employment and Wage Estimates for the United States (http://www.bls.gov/oes/current/oes_nat.htm#00-0000). With the total estimated burden hours of 631 hours, the overall annual cost of respondents’ time for the proposed collection is estimated to be $14,658.13. There will be no costs to the respondents other than their time.
Table A-12.2 Estimated Annualized Burden Costs
Type of Respondents |
Form Name |
Total Burden Hours |
Hourly Wage Rate |
Total Respondent Costs |
Households in the selected geographic area to be assessed |
CASPER Questionnaire |
630 |
$23.23 |
$14,634.90 |
Referral Form |
1 |
$23.23 |
$23.23 |
|
Total |
$14,658.13 |
|||
A.13. Estimates of Other Total Annual Cost Burden to Respondents and Record Keepers
There are no anticipated costs to respondents other than time.
A.14. Annualized Cost to the Federal Government
There are no equipment or overhead costs. The only cost to the federal government is the salary of CDC staff supporting the data collection activities. Typically up to five FTEs or EIS Officers (GS-13) participate on a CASPER. The estimated cost to the federal government is $41,414.40 based on an average hourly rate of $43.14 for a GS-13 in Atlanta obtained from the Office of Personnel Management’s website (https://www.opm.gov/policy-data-oversight/pay-leave/salaries-wages/salary-tables/17Tables/html/ATL_h.aspx). It is expected that six CASPERs will occur each year. Table A-14 below describes how this estimate was calculated.
Table A-14 Estimated Annualized Cost to the Federal Government
Staff or Contractor |
Average Number of Staff per CASPER |
Average Hours per CASPER |
Average Hourly Rate |
Average Cost |
FTE (GS-13) |
5 |
32 |
$43.14 |
$6,902.40 |
Estimated Total Average Annual Cost of 6 in-person Information Collections |
$41,414.40 |
|||
A.15. Explanation for Program Changes or Adjustments
CDC is requesting a revision of a currently approved generic clearance, Community Assessment for Public Health Emergency Response (CASPER) (0920-1036). This request is for a three year approval and includes changes that result in a decrease in requested burden. Over the past three year approval period, we have used the currently approved Generic ICR to conduct two CASPERs, while we previously estimated that a total of 15 CASPERs would be conducted annually. Going forward, we expect to conduct six CASPERs annually, and have reduced the number of burden hours to reflect this change. Additionally, we have updated respondent costs to reflect current wage data from 2015. A summary of all changes is below:
We estimate conducting six CASPERs annually, generally interviewing 210 households per CASPER. The previously approved Generic ICR estimated that we would conduct 15 CASPERs annually (15 CASPERs annually x 210 households per CASPER = 3150 households annually). This reduces the previously approved burden by 946 hours.
We estimate the completion of 24 Referral Forms annually (original general clearance approved completion of 50 Referral Forms).
We updated respondent costs to reflect current wage data from 2015.
The total reduction in burden requested for this revision is 946 hours. The total burden requested for this generic information collection is 631 hours from 1,284 respondents.
A.16. Plans for Tabulation and Publication and Project Time Schedule
Time schedules for individual CASPERs vary based on situation and site specific conditions. Due to the urgent circumstances under which a CASPER can be requested, it is important for CASPERs to be ready to initiate within 72 hours of a request if necessary, and sometimes within 24 hours of a request. The duration of the data collection varies for each CASPER, but does not exceed 180 days. If it is determined an investigation will extend beyond 180 days, the lead investigator will submit a new Standard ICR. For each CASPER, the lead investigator is responsible for developing an analysis plan and conducting the data analysis. Table A.16 represents a general schedule anticipated for most CASPERs.
Table A-16
Project Time Schedule |
|
Activity |
Time Schedule |
Data collection (field work) |
1-14 days after OMB approval |
Analyses |
1-4 weeks after OMB approval |
Reporting |
1-8 weeks after OMB approval |
Publication |
6-12 months after OMB approval |
A.17. Reason(s) Display of OMB Expiration Date is Inappropriate
The display of the OMB expiration date is not inappropriate.
A.18. Exceptions to Certification for Paperwork Reduction Act Submissions
There are no exceptions to the certification.
References
World Health Organization. Water sanitation health: environmental health in emergencies and disasters. WHO.; c2014 [cited 2014 October 24]. Available from: http://www.who.int/water_sanitation_health/emergencies/en/
Institute of Medicine (US) Roundtable on Environmental Health Sciences, Research, and Medicine. Environmental Public Health Impacts of Disasters: Hurricane Katrina: Workshop Summary. Washington (DC): National Academies Press (US); 2007; 1, Introduction. [cited 2014 October 24].Available from: http://www.ncbi.nlm.nih.gov/books/NBK54245/
Brogan D, Flagg EW, Deming M, Waldman R. Increasing the accuracy of the expanded programme on immunization’s cluster survey design. Annals Epi. 1994; 4(4): 302-311.
Malilay J, Flanders WD, Brogan D. A modified cluster-sampling method for post-disaster rapid assessment of needs. Bull WHO. 1996; 74(4): 399-405. [cited 2014 October 24]. Available from: http://apps.who.int/iris/bitstream/10665/54011/1/bulletin_1996_74%284%29_399-405.pdf?ua=1
Federal Emergency Management Association (FEMA). IS-2900 – National Disaster Recovery Framework (NDRF) Overview: Lesson 1: National Disaster Recovery Framework Introduction website. [cited 2014 December 5]. Available from: http://emilms.fema.gov/IS2900/NDRF01summary.htm
U.S. Department of Homeland Security. National Response Framework. DHS; c2008 [cited 2014 December 5]. Available from: http://www.fema.gov/pdf/emergency/nrf/nrf-core.pdf
Centers for Disease Control and Prevention (CDC). Community needs assessment and morbidity surveillance following an earthquake – Turkey, August 1999. MMWR. 1999 December 24; 48(50): 234-36. [cited 2014 December 5]. Available from: http://www.cdc.gov/mmwr/preview/mmwrhtml/mm4850a2.htm
Daley W, Karpati A, Sheik M. Needs assessment of the displaced population following the August 1999 earthquake in Turkey. Disasters. 2001; 25(1): 67-75. [cited 2014 December 05].
FEMA. IS-701.a – Multiagency coordination systems training website. [updated 2010 October 28; cited 2014 October 24]. Available from: https://training.fema.gov/EMIWeb/IS/is701alst.asp
FEMA. IS-208.A: State Disaster Management, Unit 4 Damage Assessment. [cited 2014 December 5]. Available from: http://training.fema.gov/emiweb/is/IS208A/05_SDM_Unit_04_508.pdf
FEMA. Draft rapid needs assessment in federal disaster operations: Operations manual. 2001 [cited 2014 December 5]. Available: fromhttp://www.parkdatabase.org/files/documents/2001_Rapid-Needs-Assessment_FEMA.pdf
FEMA. Incident management assistance teams fact sheet. [updated 2010 October 5, cited 2014 December 5]. Available from: http://www.fema.gov/pdf/media/factsheets/2010/imat_fact_sheet_10_05_10.pdf
CDC. Community assessment for public health emergency response (CASPER) website. [updated 2014 March 3; cited 2014 December 5]. Available from: http://www.cdc.gov/nceh/hsb/disaster/casper.htm
Buttke D, Vagi S, Schnall A, Bayleyegn T, Morrison, M, Allen M, et al. Community assessment for public health emergency response (CASPER) one year following the Gulf Coast Oil Spill: Alabama and Mississippi, 2011. Prehosp Dis Med. 2012; 27(6): 496-502. [cited 2014 October 24]. Available from: http://journals.cambridge.org/download.php?file=%2FPDM%2FPDM27_06%2FS1049023X12001380a.pdf&code=38a785005a70a3df74f024857fd4885c
Centers for Disease Control and Prevention. Emergency preparedness and response: Disaster mental health primer: key principles, issues and questions website. [updated 2012 July 31; cited 2014 October 24]. Available from: http://www.bt.cdc.gov/mentalhealth/primer.asp
Centers for Disease Control and Prevention. Mental health: Disaster and environmental mental health website. [updated 2013 October 1; cited 2014 October 24]. Available from: http://www.cdc.gov/mentalhealth/information/dis-en-health.htm
Centers for Disease Control and Prevention. Mental health website. [updated 2013 October 4; cited 2014 October 24]. Available from: http://www.cdc.gov/mentalhealth/
Centers for Disease Control and Prevention. CDC mental health work group website. [updated 2013 November 13; cited 2014 October 24]. Available from: http://www.cdc.gov/mentalhealth/workgroup.htm
Safran MA, Chorba T, Schreiber M, Archer WR, Cookson ST. Evaluating mental health after the 2010 Haitian earthquake. Disaster Med Public Health Prep. 2011;5:154-157. [cited 2014 October 24]. Available from: http://journals.cambridge.org/download.php?file=%2FDMP%2FDMP5_02%2FS1935789300003396a.pdf&code=9a33c0f3dea5d47128e851f47f408cbf
Brogan D, Flagg EW, Deming M, Waldman R. Increasing the accuracy of the expanded programme on immunization’s cluster survey design. AEP. 1994 July; 4(4): 302-311.
Serfling, R.E., and Sherman, I.L.: Attribute Sampling Methods for Local Health Departments With Special Reference to Immunization Surveys, PHS publication 1230, (March) 1965.
Cochran WC. Sampling Techniques. 3rd ed. New York: Wiley; 1978: 12-15
Henderson RH, Sundaresan T. Cluster sampling to assess immunization coverage: a review of experience with a simplified sampling method. Bulletin of the World Health Organization, 1982, 60: 253-260.
List of Attachments
Attachment A. Authorizing Legislation
Attachment B. 60-day Federal Register Notice
Attachment C. Sample Questionnaire
Attachment D. Sample Tracking Form
Attachment E. Sample Referral Form
Attachment F. Sample Final Report
Attachment G. Request for Approval under Generic Clearance for CASPER Data Collections
Attachment H. Burden Memo
Attachment I. Step-by-Step How to Use the Generic Clearance for CASPER
Attachment J. Sample Introduction and Consent Script
Attachment K. Sample Sampling Frame
Attachment L. Sample Press Release
Attachment M. Sample Paper
Attachment N. Weighted Analysis
| File Type | application/vnd.openxmlformats-officedocument.wordprocessingml.document |
| Author | Richardson, Tony (CDC/OD/OADS) |
| File Modified | 0000-00-00 |
| File Created | 2021-01-21 |
© 2026 OMB.report | Privacy Policy