Supporting Statement A
02_Supporting Statement A_ASPE-CDC Study SUDs and Child Welfare_Response to OMB Questions 6-7-2019.docx
ASPE Generic Clearance for the Collection of Qualitative Research and Assessment
Supporting Statement A
OMB: 0990-0421
Addressing Substance Use Disorders Among Families Involved with the Child Welfare System: A Cross-Agency Collaboration
ASPE Generic Information Collection Request
OMB No. 0990-0421
Supporting Statement – Section A
Submitted: April 12, 2019
Program Official/Project Officer
Laura Radel
Senior Social Science Analyst
Division of Children and Youth Policy
Office of the Assistant Secretary for Planning and Evaluation
U.S. Department of Health and Human Services
200 Independence Avenue, SW
Washington, DC 20201
202-730-3927
laura.radel@hhs.gov
Section A – Justification
The Office of the Assistant Secretary for Planning and Evaluation (ASPE) and the Centers for Disease Control and Prevention (CDC) are requesting clearance for a new, cross-agency data collection entitled, “Addressing Substance Use Disorders Among Families Involved with the Child Welfare System: A Cross-Agency Collaboration.” Recognizing that communities across the United States are facing challenges related to substance/opioid misuse and its impact on children and families and their involvement in child welfare, ASPE and CDC are collaborating on a multicomponent study to identify strategies to help break this cycle. Through this collaboration, ASPE and CDC will fund separate study components with a shared goal of identifying promising strategies and potential protective factors that may help to address rising rates of substance/opioid misuse and child welfare entries. There are two components to this study and eight data collection activities, including in-person, telephone/Skype, and/or online key informant interviews (KIIs) and focus groups.
Study Component 1 (ASPE): “Addressing Substance Use Disorders Among Families Involved with the Child Welfare System: Challenges and Promising Strategies in Rural Communities” (short title, Rural Communities Substudy [RCS])
RCS instruments include (1) Wave 1 KIIs–Experts, (2) Wave 2 KIIs/Site Visit Interviews–Program Administrators, (3) Site Visit Interviews–Practitioners, (4) Site Visit Interviews–Partners/Other Related Organizations,
Study Component 2 (CDC): “Formative Research on Opioids and Their Impact on Children, Youth, and Families (short title, Community Burden Substudy [CBS])
CBS instruments include (1) KII–Parents/Caregivers, (2) KII–Providers/Stakeholders, (3) Focus Group Guide–Caregivers, and (4) Focus Group Guide–Providers/Stakeholders.
Circumstances Making the Collection of Information Necessary
Background
Foster care entries have been on the rise since 2012 (Children’s Bureau, 2018). Findings from a recent study by ASPE confirmed that substance misuse—particularly related to the opioid crisis—is contributing to more children entering the child welfare system (Radel et al., 2018; Child Welfare Information Gateway, 2018; Oliveros & Kaufman, 2011). Over the last several years, the sharp rise in opioid misuse and drug overdose deaths has inundated child welfare agencies with increased caseloads, removals, and foster care placements. Similarly, high rates of drug-related hospitalizations and overdose deaths coincide with increases in substantiated reports of child abuse and neglect (CAN). More specifically, the ASPE study found that a 10 percent increase in drug overdose death rates corresponds to a 2.4 percent increase in substantiated child maltreatment reports and a 4.4 percent increase in foster care entry rates (Radel et al., 2018). With adverse childhood experiences (ACEs), such as exposure to abuse, neglect, and parental substance misuse, widely linked to a variety of poor health and behavioral outcomes in both the short- and long-term, disrupting the substance misuse-child welfare cycle is more critical than ever (Felitti et al., 1998; Finkelhor et al., 2013; Fin et al., 2015).
While many communities across the United States struggle with this issue, the relationship between overdose death rates and foster care entry rates varies in different areas of the country. Some regions experience a higher burden than others—as evidenced by stronger, positive relationships between rates of overdose deaths and foster care entries. For example, rural counties in Appalachia, Montana, New England, and Oklahoma have a strong positive association, whereas nearly all counties in other rural states, such as Iowa, Nebraska, and North and South Dakota, do not (Radel et al., 2018). Similar variations exist in urban and suburban counties. Although the reasons for the differential burden is not known, differences in community services, supports, resources, and partnerships may contribute to these variations.
Still, overdose deaths continue to rise across the nation, especially in rural states (Keyes et al., 2014; Vivolo-Kantor et al., 2018). Rural areas likely face greater vulnerability to drug use than urban or suburban areas due to more depressed economic conditions, longer distances to substance use disorder treatment facilities, and poorer transportation infrastructure. Areas with high poverty and unemployment rates have higher rates of retail opioid sales, opioid-related hospitalizations, and fatal drug overdoses (Ghertner & Groves, 2018; Keyes et al., 2014). Nationally representative surveys show that polysubstance use and depression are associated with nonmedical opioid use in rural areas (Keyes et al., 2014). Those seeking treatment and recovery services for substance use in rural areas often face limited options, long waiting lists, and long travel distances to available services (President’s Commission on Combating Drug Addiction and the Opioid Crisis, 2017; Radel et al., 2018; Rosenblatt et al., 2015). Although both rural and urban communities face similar challenges, weaker community infrastructure and support services exacerbate the difficulties of rural families. Child welfare agencies in rural and urban areas face a variety of barriers in assessing substance use, addressing the needs of children with neonatal abstinence syndrome, and connecting families with treatment for substance use (Child Welfare Information Gateway, 2018; Radel et al., 2018).
In addition to issues facing rural communities, untangling and addressing the connections between substance misuse and families requiring support services is a significant challenge. In response to growing demand for child welfare services and the complex contributing role of substance misuse, there is emerging recognition of the need to focus efforts on family strengths and capacity to care for children and prevent entry into the child welfare system. While ACEs, including CAN and trauma, are known to increase the risk of substance abuse later in life (Anda et al., 2008; Dube et al, 2003), separating children from their families and placing them in foster care can be traumatic in and of itself (Bruskas & Tessin, 2013). Parental substance abuse is also a well-established risk factor for children misusing drugs and alcohol later in life (Kumpfer, 1987). It is critically important that we break the cycle whereby parental substance misuse results in ACEs, including foster care entry, which increases the likelihood of substance abuse and child maltreatment by those same children as they grow into adults. As such, there is a growing awareness that support services for families experiencing substance misuse must be multifaceted, including support for both parent or caregiver recovery as well as the child’s immediate safety and well-being (First Focus Campaign for Children, 2018; NIDA, 2016).
The Need for Evaluation
The rise of opioid misuse has led to a large federal response, including passage of the Family First Prevention Services Act, which allows states, beginning in federal fiscal year 2020, to use Title IV-E funding to support evidence-based substance use treatment services, not only for families whose children are already in foster care, but also for parents whose children are at risk of entry into foster care. State and local initiatives also offer opportunities; for example, the Connecticut Family Stability Pay for Success Project leverages public and private partnerships to expand substance use treatment services for families in the child welfare system. There is a need to understand how various communities are leveraging these resources to address and prevent opioid and other substance misuse and out-of-home placements.
Because of the challenges facing rural communities, it is unclear whether they can make full use of these opportunities. Many rural areas find it difficult to attract a sufficient workforce to meet demand or expand, and evidence-based programs or practices might require specific clinicians or professionals that are not available in rural areas. In addition, the evidence to support certain substance use treatment services might not extend to other settings and populations, such as those in rural communities or parents with child welfare involvement. Thus, understanding the challenges facing rural communities and identifying promising strategies to help them overcome their challenges is needed.
To further help communities, we must also explore potential reasons for variations in the substance misuse-child welfare relationship in different areas, with specific emphasis on supports and services and substance misuse trajectories within families. For example, low and mixed burden communities may offer protective factors for substance misuse and/or ACEs that are not present in higher burden communities. Thus, studying the resources, supports, services, and partnerships of low, mixed, and high burden communities may help to identify factors with the potential to lessen the impact of substance misuse on children and families and their involvement with child welfare.
Building on findings from ASPE’s previous study, ASPE and CDC are collaborating on a new, multicomponent effort entitled, “Addressing Substance Use Disorders Among Families Involved with the Child Welfare System: A Cross-Agency Collaboration.” ASPE and CDC are funding separate study components with a shared goal of identifying promising strategies and potential protective factors to help communities overcome challenges and disrupt the substance misuse-child welfare link.
Study Component 1 (ASPE): Addressing Substance Use Disorders Among Families Involved with the Child Welfare System: Challenges and Promising Strategies in Rural Communities (Rural Communities Substudy [RCS])
In 2018, ASPE funded a contractor (Mathematica Policy Research) to conduct study component 1, the Rural Communities Substudy. The RCS aims (1) to provide insights into the key issues and specific challenges rural communities face in serving families that have substance use disorders and are involved in the child welfare system, including taking advantage of state and federal opportunities; (2) to identify promising strategies that rural communities could use or adapt to better serve child-welfare-involved families with parental substance use; and (3) to identify opportunities at the federal, state, and local levels to support implementation of promising strategies. This component will begin with an environmental scan and literature review to identify key issues and promising strategies to be explored further in key informant and site visit interviews.
The contractor will conduct up to 12 KIIs in 2 waves, with 6 interviews in each, and conduct 6 site visits in rural communities implementing promising strategies. Key informants will be familiar with substance use treatment and child welfare issues in rural areas. Wave 1 key informant interviews will be conducted with substantive experts, evaluators, program directors, and developers. Wave 2 interviews will be conducted with program administrators. Site visit participants will include program administrators; practitioners (those who work directly with families) from child welfare agencies and substance use treatment facilities; and partners or agencies they collaborate with, including evaluators. The following four discussion guide instruments will be used: (1) Wave 1 KIIs–Experts (Instrument 1); (2) Wave 2 KIIs/Site Visit Interviews–Program Administrators (Instrument 2); (3) Site Visit Interviews–Practitioners (Instrument 3); and (4) Site Visit Interviews–Partners/Other Related Organizations (Instrument 4). The four are included as Attachments A through D, respectively. The informed-consent document for all RCS key informant and site visit interview participants is included as Attachment E.
Study Component 2 (CDC): Formative Research on Opioids and Their Impact on Children, Youth, and Families (Community Burden Substudy [CBS])
To build upon the previous work of ASPE, in 2018, CDC funded a contractor (ICF) to conduct study component 2, the Community Burden Substudy. The CBS aims to explore resources, supports, and prevention strategies across counties with low, mixed, or high opioid/child welfare burden to identify factors that may protect families and children from opioid misuse and/or ACE exposure. The contractor will visit matched county pairings within three states to conduct in-person data collection with the following groups: parents involved with child welfare who engage in opioid misuse, kinship caregivers, foster parents, service providers (e.g., child welfare, substance use treatment), and key stakeholders identified by the state officials.
Data collection instruments include the following: (1) KII–Parents/Caregivers, (2) KII–Providers/Stakeholders, (3) Focus Group Guide–Caregivers, and (4) Focus Group Guide–Providers/Stakeholders. Participants will complete a brief demographic form prior to their scheduled sessions. See Attachments F–K for CBS instruments and informed consents.
Clearance Request
In the current information collection request, ASPE and CDC seek approval for the new data collection, “Addressing Substance Use Disorders Among Families Involved with the Child Welfare System: A Cross-Agency Collaboration.” The current information collection request represents a multicomponent study collaboration between ASPE and CDC. This data collection will be conducted using the Generic Information Collection mechanism through ASPE – OMB No. 0990-0421.
Across study components, findings from this data collection will:
Provide nuanced information to supplement the key issues and promising strategies identified through an environmental scan and a literature review related to rural communities;
Inform the selection of promising strategies by state and local administrators and future research by ASPE and its federal partners to bolster the evidence of promising strategies for further dissemination in other rural communities;
Explore differences in services, resources, opioid misuse trajectories, and stigma in communities with low, mixed, and high opioid-child welfare burden; and
Identify factors for further research that may help to protect communities, families, and children from opioid misuse and/or ACE exposure.
Purpose and Use of the Information Collection
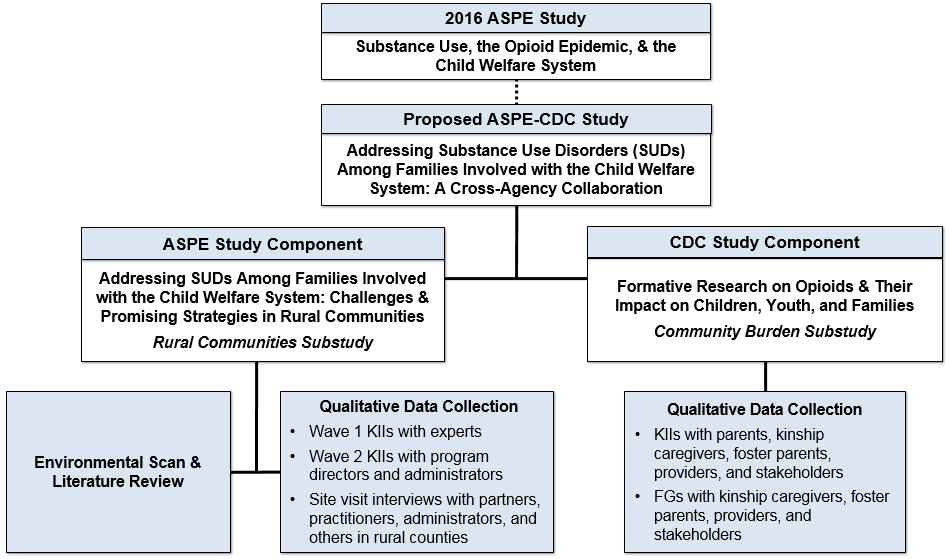
The current ASPE-CDC study collaboration consists of two components—ASPE’s Rural Communities Substudy and CDC’s Community Burden Substudy. Each agency is separately responsible for conducting data collection associated with its component. Both components consist of qualitative data collection, while the RCS also involves an environmental scan and literature review. An overview of the multicomponent study is displayed in Exhibit A2-1.
Exhibit A2-1. ASPE-CDC Cross-Agency Multicomponent Study Collaboration
Study Component 1 (ASPE): Rural Communities Substudy
The purposes of the Rural Communities Substudy is to:
Understand the challenges specific to rural communities when serving child-welfare-involved families with substance use disorder
Identify promising strategies rural communities can use or adapt to better serve these families
Assess and describe the evidence base of promising strategies, key issues and challenges the strategies address, and contextual factors that could affect their effectiveness
Identify federal, state, and local opportunities that rural communities can leverage to improve services and outcomes for child-welfare-involved families with parental substance use
Data collected through the key informant and site visit interviews are needed to supplement information obtained through an environmental scan and literature review. Without collecting these data, we will be limited in our ability to identify and understand the nuances of implementing promising strategies. For example, some strategies hold promise but have limited evidence to demonstrate their effectiveness and thus might not appear in the peer-reviewed or gray literature. Other strategies have been implemented successfully in settings or with populations different from those targeted for this study. Interview and site visit data from people with firsthand knowledge of and experience with the promising strategies will provide insights into the contextual and implementation factors that may not be described in full or in ways that would inform adaptation for rural communities.
The environmental scan and literature review will provide background or preliminary information on the four aims of the data collection described above. However, the literature is unlikely to provide sufficient detail about promising strategies, such as how rural communities adapt them or leverage federal, state, or local opportunities to implement them. Therefore, information from the interviews and site visits will be important to understanding how policies and practices in child welfare and substance use treatment can help rural communities address key challenges and make use of federal, state, and local opportunities to address the rise in substance and opioid misuse. Although ASPE project staff will know the identities of the key informants and the entities hosting the site visits, ASPE will not include names, titles, or other information that will disclose the identities of the participants in any information from this study that becomes publicly available. Exhibit A2-2 outlines the data collection participants, activities, and methods associated with the Rural Communities Substudy.
Exhibit A2-2. RCS Participants, Data Collection Activities, and Methods
Participants |
Data Collection Activities & Methods |
Substantive experts, evaluators, program directors, and developers |
|
Program directors and administrators |
|
Practitioners, program administrators, partners, and other related organization staff |
|
Study Component 2 (CDC): Community Burden Substudy
The purpose of the CDC Community Burden Substudy is to conduct a formative study to identify opportunities for injury and violence prevention among children, youth and families and the health and human service systems that serve them. Substance misuse may limit parents’ capacity to provide sensitive, responsive, and consistent care and may lead to adverse childhood experiences (ACEs). For instance, the misuse of opioids and other substances might lead a parent to forget or neglect parenting responsibilities, limit their ability to provide adequate supervision, expose children to unsafe situations, and potentially engage in neglectful and/or abusive behavior toward children that can bring them to the attention of Child Protective Services (CPS). Given the widespread nature of the opioid epidemic, the CDC is interested in understanding whether there are community factors (e.g., systems and supports) that might prevent ACEs and parental substance misuse. The Community Burden Substudy sampling plan is designed to sample from communities with high and low burdens of opioid misuse and CPS reports.
Since there has been limited research to date on this issue, the information that we learn from this study may help support the development of primary and secondary prevention strategies that have the potential to disrupt the pathways between substance misuse and ACEs to improve safety, stability, and permanency outcomes for children. Since the previous ASPE study did not speak with parents and caregivers, this important perspective will allow CDC to better understand the needs of this important group and develop more targeted and relevant approaches. Specific goals of the study include the following:
Identify services, supports, resources, and partnerships present in low and mixed burden counties that may protect against substance misuse and/or children’s exposure to violence and other ACEs and determine how these compare to the characteristics of higher burden counties;
Identify existing primary prevention strategies for opioid/substance misuse in low and mixed burden counties and determine how these compare to/differ from the strategies present in higher burden counties;
Determine the varying trajectories into opioid misuse that place children at risk for exposure to violence and other ACEs and potential opportunities for prevention; and
Determine how experiences related to stigma around seeking help and the availability and accessibility of services differ for children, youth, and families in counties with varying burdens.
The CBS team will conduct separate, weeklong site visits to six counties across three states to complete in-person KIIs and focus groups. See Exhibit A2-3 for an overview of data collection participants, activities, and methods for each county. In total, the CBS team will conduct 108 KIIs and 30 focus groups across counties. Participants will complete a brief demographic form in person or by telephone prior to their session.
Exhibit A2-3. CBS Participants, Data Collection Activities, and Methods in Each County
Participants |
Data Collection Activities & Methods |
Parents with opioid misuse who are involved with CW |
|
Kinship caregivers |
|
Foster parents |
|
Multi-sectoral providers and stakeholders |
|
The CBS team will aim to conduct all parent, caregiver, and provider/stakeholder KIIs and focus groups in person during site visits to each of the six counties. Team members will prioritize scheduling sessions with parents and caregivers to maximize flexibility for these participants. We will conduct KIIs by telephone if requested by participants or as needed to complete data collection. If needed, team members will schedule provider/stakeholder KIIs and focus groups to occur remotely after the site visit. All interview and focus group participants will complete a brief demographic form prior to their session.
Within each state, the CBS team will visit two counties matched on county level unemployment, median household income, average poverty status, and average percent uninsured across all ages. Counties will be selected on the basis of the burden experienced across opioid misuse (i.e., overdose deaths) and child welfare entries. Matched counties will be paired on the basis of burden as follows: (1) low opioid misuse/low child welfare burden and high opioid misuse/high child welfare burden (low/low and high/high); (2) low opioid misuse/low child welfare burden and high opioid misuse/low child welfare burden (low/low and high/low); and (3) high opioid misuse/high child welfare burden and high opioid misuse/low child welfare burden (high/high and high/low).
Use of Improved Information Technology and Burden Reduction
Across components, every effort will be made to limit burden on individual respondents who participate in data collection activities through the use of technology and flexibility in scheduling.
Study Component 1. Rural Communities Substudy
The RCS team will conduct key informant interviews by telephone to accommodate the scheduling preferences of the participants and to facilitate collection of information from various locations around the country. We will conduct up to six in-person site visits to observe the rural sites and establish rapport with participants.
To avoid asking questions that can be answered through publicly available information, and to minimize the burden on participants, we will leverage information learned through our environmental scan and literature review on potential strategies. All interviewers will prioritize questions in the discussion guides that are most central to this study and to the individual respondent’s expertise and thus that cannot be addressed through other sources.
Study Component 2. Community Burden Substudy
Although the CBS team will aim to conduct all data collection in person, it is possible that participants may not be available during the scheduled site visits and/or that some sessions may need to be completed after the site visit. In these cases, the CBS team will conduct sessions remotely. We recognize that some parents and caregivers may not have access to computers and/or the internet; thus, we will conduct remote interviews and focus groups with these individuals by telephone to maximize the potential for participation and reduce burden. Because providers and stakeholders are likely to have access to computers and the internet, the CBS team will conduct KIIs by telephone or Skype and focus groups by telephone and/or online through meeting software, such as Adobe Connect.
The CBS team will obtain limited personally identifying information (PII) as needed to facilitate contacting respondents. In order to reach out to potential participants to request their participation in the study, the contractor will collect limited PII in terms of name and phone/email contact information. All contact information will be stored separately and will not be linked to the interview or focus group data. Once interviews have been completed, the contact information will be deleted. No PII will be shared with CDC and any identifying information will be scrubbed from files shared with CDC. Additionally, no participants will be identified by name or description in any reports and all information will be provided as an aggregate summary. An HHS Privacy Impact Assessment form has been completed for the PII, including names and contact information that will be stored on ICF’s secure system during the data collection process. The PIA was submitted in November 2018.
Efforts to Identify Duplication and Use of Similar Information
CDC reached out to ASPE to assess how to build on their previous work without duplicating it. In addition, CDC also reviewed the Federal Register and searched proposed data collections using the key words “formative”, “opioid”, and child welfare. Of the 43 records returned, none proposed research into promising strategies and opportunities to address key challenges and issues of rural communities to improve child welfare outcomes for families with parental substance use or research into protective factors present in low or mixed burden communities that may have the potential to disrupt the opioid misuse-child welfare problem in higher burden counties. CDC also searched the Office of the Administration for Children & Families Children’s Bureau funded research and Child Welfare Information Gateway. In addition, CDC searched the published research literature and is an active member in Federal Interagency Workgroups focused on adverse childhood experiences and the opioid epidemic, through which member agencies share information about ongoing activities, including research, in this space. Through these groups we consulted with HRSA’s Office of Rural Health about ASPE’s rural substudy as well as with SAMHSA’s staff working on early childhood issues. We also discussed the effort with CMS staff working on their Maternal Opioid Misuse financing models. It is our understanding from our literature review, outreach through working groups, and individual staff outreach to relevant agencies, that no other prior or current research efforts have substantial overlap with our proposed study. To our knowledge, ASPE and CDC are the only federal agencies funding a multicomponent study of this nature.
Impact on Small Businesses or Other Small Entities
Some data collection participants will include individuals from public and private agencies, such as the child welfare system and healthcare practices; however, these data collections will not have a significant impact on the agencies or entities.
For the Community Burden Substudy, we also will work closely with a representative from each local child welfare agency to serve as a site liaison. There will be 6 site liaisons in total. The site liaison will help support identifying and recruiting parents and caregivers involved with the agency to participate in KIIs and focus groups during the site visit. The CBS contractor will work with an administrator from the child welfare agency to approve this role, identify an appropriate individual, and ensure that study-related responsibilities do not significantly impact the individual or agency.
Consequences if Information Collected Less Frequently
This request represents a one-time data collection across both components of the “Addressing Substance Use Disorders Among Families Involved with the Child Welfare System: A Cross-Agency Collaboration” study. With drug overdose deaths recently surpassing deaths from traffic accidents and child welfare entries on the rise, ASPE and CDC are collaborating to identify feasible strategies with the potential to help struggling communities overcome these issues.
If data are not collected as part of the Rural Communities Substudy, rural communities, policymakers, and other stakeholders might have less information about (1) which strategies are promising to address substance use among child-welfare-involved families in rural communities, (2) how these strategies might address challenges in their communities, and (3) how opportunities might be taken to leverage these strategies.
Further, if data are not collected for the Community Burden Substudy, we will be missing the perspective of parents and caregivers in developing strategies to help communities struggling with substance misuse and address the opioid epidemics impact on children, youth, and families. Due to our inclusion of counties experiencing different degrees of impact from the crisis in terms of mortality burden and foster care entries, we would also have less information without this study about promising strategies, services, supports, resources, and partnerships present in low and mixed burden counties that may protect against substance misuse and/or children’s exposure to violence. Without this information, we may be missing key opportunities within communities to support families and prevent parental substance misuse, child abuse and neglect, and other adverse childhood experiences.
Special Circumstances Relating to the Guidelines of 5 CFR 1320.5
There are no special circumstances with this information collection package. This request complies fully with regulation 5 CFR 1320.5 and will be voluntary.
Comments in Response to the Federal Register Notice and Efforts to Consult Outside the Agency
This data collection is being conducted using the Generic Information Collection mechanism through ASPE – OMB No. 0990-0421 therefore, no additional Federal Register notice is required.
Explanation of Any Payment or Gift to Respondents
The ASPE study will not provide payments or gifts to respondents for their participation. However, for the Community Burden Study, CDC will provide parents and caregivers participating in data collection an incentive of no more than $50 to offset the costs of participating in the study, including costs of transportation and childcare that may otherwise preclude participation. We believe this measure will ensure that lower-income parents and caregivers are not systematically discouraged from participating due to the costs of participation and help to avoid non-response bias. The incentive will only be used for parents and caregivers. No incentive will be provided for service providers or multi-sectoral stakeholders.
Assurance of Confidentiality Provided to Respondents
Study Component 1: Rural Communities Substudy
The Privacy Act does not apply to this data collection. State and local administrators and practitioners who answer questions will be answering in their official roles and will not be asked about, nor will they provide, sensitive individually identifiable information.
Before beginning all interviews, the interviewer will provide each participant a copy of the informed consent (see Attachment E), which will provide an overview of the project and describe the following key points: (1) participation is voluntary; (2) participants can decline to answer or skip any question that they do not wish to answer and can stop or pause the interview at any time, with no negative consequences; (3) although participant names and titles will not be used in summaries or briefs, a goal of the project is to disseminate information about promising strategies, which will likely necessitate naming the site’s organization and location; (4) Mathematica intends to audio-record the interview, but participants have the opportunity to opt out of the recording and still participate. For interviews conducted by telephone, interviewers will email the informed consent to participants and offer to mail a hard copy if preferred. For in-person site visits, interviewers will provide a hard copy to keep. Interviewers will give each participant as much time as needed to review the informed consent. Interviewers will verbally request participation for the interview and for audio-recording and will not request a signature for informed consent because a signed inform consent form would be the only hard copy record linking the participant and the research. The contractor will not record any session where a participant does not agree to recording. Instead, the interviewer will take notes during the interview. If the participants agree to the interview and to the audio-recording, the recordings will be stored on Mathematica’s secure network. Only a limited number of Mathematica staff (those working directly on the project) will have access to the recordings. The interview recordings will be deleted upon approval of the project deliverables (issue briefs). The contractor will securely store participant names and contact information for the purposes of recruitment and scheduling. Participant names will be stored a separate secure file directory from participant responses. All personally identifiable information will be scrubbed from files before they are shared with ASPE or CDC. Any data findings shared with ASPE will go through a disclosure analysis to minimize the identification of interview and site visit participants. Reporting of findings will exclude a description of observable characteristics of participants to minimize disclosure risk. . Additionally, no participants will be identified by name or description in any reports and all information will be provided as an aggregate summary.
Study Component 2: Community Burden Substudy
To ensure the confidentiality of data compiled and the protection of human subjects, the data collection protocol and instruments for the Community Burden Substudy will be reviewed through the ICF institutional review board (IRB) prior to the collection of covered or protected data. The ICF IRB holds a Federal wide Assurance (FWA00002349; Expiration, 07/12/2023) from the HHS Office for Human Research Protections (OHRP). This review ensures compliance with the spirit and letter of HHS regulations governing such projects.
All personally identifying information (PII) will be stored on secure servers at ICF in the manner described in the IT Data Security Plan. We will collect and securely store participant names and contact information only to facilitate contacting respondents. This information will be stored separately and will not be linked to participants’ data. Once interviews have been completed, the contact information will be deleted. As an added step in protecting the privacy of study participants, we will invoke the certificate of confidentiality (CoC), which is automatically granted for CDC-funded research in which identifiable, sensitive information is collected or used. The CoC will support the CBS team in protecting the data against compulsory legal demands (e.g., court orders, subpoenas) for identifying sensitive information or identifying characteristics of a research participant.
Prior to beginning all data collection, the KII or focus group moderator will review the informed consent aloud, including the following: (1) purpose of the substudy; (2) rights regarding participation and the voluntary nature of participation; (3) procedures to protect privacy; (4) additional privacy protections (the CoC); (5) the sensitive nature of questions (for parents and caregivers), risks, and benefits; (6) intent to audio record the session; and (7) contact information for the principal investigator. The moderator will request permission to audio record each session and obtain verbal consent to participate. If a participant declines to be audio recorded, a second team member will take detailed notes during the in-person or telephone/online session. For interviews conducted by telephone, interviewers will email the informed consent to participants if an email is provided or read the informed consent prior to the interview if not. For in-person site visits, interviewers will provide a hard copy to keep. Interviewers will give each participant as much time as needed to review the informed consent and ask questions. Informed consents will not request a signature. The study protocol is currently under review by the ICF IRB and a final determination has not yet been made. However, initial feedback from the ICF IRB has indicated that the IRB will exempt the need for a written signature.
For those interviews/focus groups that are recorded, audio files will be housed on the laptop computers of research staff until transferred to ICF’s secure server. Only a limited number of ICF staff (those working directly on the project) will have access to the recordings. All audio files will be deleted within two weeks of being checked for accuracy and transcribed. The contractor will not record any session where a participant does not agree to recording. Instead, the interviewer will take notes during the interview, and similar to the audio files, notes will be transferred to ICF’s secure server and removed from the research staff’s computers.
Justification for Sensitive Questions
No information of a personal or sensitive nature will be collected as part of ASPE’s Rural Communities Substudy. However, the Community Burden Substudy involves the collection of some sensitive information among parents and caregivers. CBS instruments designed for use with parents and caregivers may include questions about parental opioid/substance misuse, child welfare involvement, children’s exposure to violence and other ACEs, and help seeking for substance misuse. These questions are central to CDC’s goal of learning about trajectories into opioid misuse, children’s exposure to violence and ACEs, and possible protective factors for opioid misuse and ACEs.
Participants will be told that their answers will be kept secure and that their responses will not be linked to them personally. Participants will also be informed about the certificate of confidentiality but told that interviewers will still be required to report participants who pose a danger to themselves or others, or if child abuse or neglect is suspected. The informed consent left with participants will also contain contact information for the both the project director and ICF IRB in case a participant has further questions or concerns.
Data collectors will also be trained and instructed on handling a participant crisis should one arise. Crisis instructions will be provided during the pre-data collection training. Data collectors will be instructed that should interviewers sense that participants are feeling distressed or don’t wish to continue with the interview, that the interview should be concluded without putting the participant under any undue stress. All interviewers will be experienced in conducting field data collection and should be able to detect a situation where the interviewee may be uncomfortable or wish to discontinue. The interviewer will also be instructed to help the person reconnect and regain control over his or her feelings by normalizing the person’s feelings and experience, reminding him or her that it is not unusual for people to have strong feelings arise following this type of interview. Participants can also be connected with the local child welfare agency for additional resources if requested. Participants will also receive key CDC resources that might be helpful in navigating their day-to-day challenges (e.g., Essentials for Parenting Toddlers and Young Children).
Estimates of Annualized Burden Hours and Costs
For the Rural Communities Substudy’s key informant interviews, the estimated burden is 60 minutes per response. We plan to interview up to 24 key informants, for a total of 24 hours. For site visit interviews, the estimated burden is 90 minutes per response. We plan to conduct site visit interviews with up to 120 participants, for an estimated burden of 180 hours. The total annualized burden for all 144 participants across all instruments is 204 hours.
As part of the Community Burden Substudy, we will conduct a total of 108 key informant interviews with parents, caregivers, providers, and stakeholders. In addition, we will conduct a total of 30 focus groups with parents, caregivers, providers, and stakeholders. Each focus group will involve approximately 8 participants. The burden for the KIIs and focus groups includes 3 minutes to complete a brief demographic form prior to participation. As such, the burden for KIIs is 63 minutes and the burden for focus groups is 90 minutes.
Exhibit A-12 shows estimated burden and costs for the ASPE-CDC study.
Exhibit A-12: Estimated Annualized Burden Hours and Costs to Respondents – Addressing SUDs among Families Involved with the Child Welfare System: A Cross-Agency Collaboration
Type of respondent |
No. of Respondents |
No. of responses per respondent |
Average burden per response (in minutes) |
Total burden hours |
Hourly wage1 |
Total respondent costs |
Rural Communities Substudy |
||||||
Key informants – wave 1: Substantive experts, evaluators, program directors, and developers |
12 |
1 |
60 |
12 |
$39.96 |
$480 |
Key informants – wave 2: Program administrators |
12 |
1 |
60 |
12 |
$39.96 |
$480 |
Site visits: Program administrators |
12 |
1 |
90 |
18 |
$33.91 |
$610 |
Site visits: Practitioners |
72 |
1 |
90 |
108 |
$23.28 |
$2,514 |
Site visits: Partners or staff from related organizations |
36 |
1 |
90 |
54 |
$33.91 |
$1,831 |
STUDY 1 TOTALS |
144 |
|
|
204 |
|
$5,915 |
Community Burden Substudy |
||||||
KII informants – Parents/Caregivers |
84 |
1 |
63/60 |
88 |
$7.25 |
$638 |
KII informants – providers/stakeholder |
24 |
1 |
63/60 |
25 |
$28.56 |
$714 |
FG participants – Caregivers |
96 |
1 |
93/60 |
149 |
$7.25 |
$1,080 |
FG participants – Providers/stakeholders |
144 |
1 |
93/60 |
223 |
$28.56 |
$6369 |
CW site liaison |
6 |
1 |
180 |
18 |
$28.56 |
$514 |
STUDY 2 TOTALS |
354 |
|
|
503 |
|
$9,315 |
|
||||||
COMBINED TOTAL |
498 |
|
|
707 |
|
15,230 |
1Estimates for the average hourly wage for respondents are based on the Department of Labor 2017 National Occupational Employment and Wage Estimates, March 30, 2018. Available at https://www.bls.gov/oes/current/oes_nat.htm.
Estimates of Other Total Annual Cost Burden to Respondents or Record Keepers
There will be no direct costs to the respondents other than their time to participate in each data collection.
Annualized Cost to the Government
The total annualized cost to the government across the two components is $498,119. The breakdown of how that estimate was reached for each component is below.
Governmental costs for the Rural Communities Substudy project include personnel costs for federal staff overseeing the project; data collection instrument and OMB materials development; and data collection, analysis, and reporting. This level of effort includes approximately 10 percent of a GS-14 behavioral scientist’s time (assuming a $97,400 annual salary, this totals $19,480). There are no equipment or overhead costs; however, a contractor is being used to support this effort. The contract amount to plan, conduct, and analyze the data is $274,972. Thus, the total cost to the government for the RCS is $294,452.
Governmental costs for the Community Burden Substudy project include personnel costs for federal staff overseeing the project; data collection instrument and OMB materials development; and data collection, analysis, and reporting. This level of effort includes approximately 10 percent of a GS-13 behavioral scientist’s time (assuming a $97,400 annual salary, this totals $19,480). There are no equipment or overhead costs; however, a contractor is being used to support this effort. The contract amount to plan, conduct, and analyze the formative research is $184,187. Thus, the total cost to the government for the CBS is $203,667.
Explanation for Program Changes or Adjustments
This is a new data collection.
Plans for Tabulation and Publication and Project Time Schedule
Data Analysis and Plans for Publication
Study Component 1. Rural Communities Substudy
After the key informant and site visit interviews, the contractor will prepare site-specific summaries using standardized templates to document key findings.
The contractor will prepare two issue briefs for ASPE to summarize study findings, which will be made publicly available.
Study Component 2. Community Burden Substudy
CBS team members will analyze the qualitative data to identify patterns and themes related to the aims of the research and summarize findings. The team will analyze data from the demographic information forms using basic descriptive analyses. All data will be reported in aggregate. Team members will prepare the following reports: (1) summary report of KIIs/focus groups with providers/stakeholders, (2) summary report of focus groups with caregivers, (3) summary report of interviews with parents and caregivers, and (4) a final project report.
Project Time Schedule
Below we present the project time schedule for each study. Note that all dates are dependent upon the receipt of OMB approval, which is estimated for April 2019.
Exhibit A16. Project Time Schedule
Project Time Schedule |
|
Rural Communities Substudy |
|
November 2018–February 2019 |
Develop discussion guides and recruitment plan |
February 2019 |
Outreach and scheduling of Wave 1 key informant interviews |
March–April 2019 |
Conduct Wave 1 key informant interviews; outreach and scheduling of site visits |
May–July 2019 |
Conduct Wave 2 key informant interviews and 6 site visits |
August–November 2019 |
Analyze findings on promising strategies to ASPE |
September–December 2019 |
Analyze findings and submit memo and briefing to ASPE |
Community Burden Substudy |
|
April 2019 |
Estimated OMB approval date |
March-June 2019 |
Work with state and local child welfare agencies to gain study buy-in and identify participants |
July-December 2019 |
Conduct site visits and analyze data |
January – March 2020 |
Prepare and submit report summaries |
September 2020 |
Submit final project report |
Reason(s) Display of OMB Expiration Date is Inappropriate
We are requesting no exemption.
Exceptions to Certification for Paperwork Reduction Act Submissions
There are no exceptions to the certification. These activities comply with the requirements in 5 CFR 1320.9.
REFERENCES
Anda RF, Brown DF, Felitti VJ, et al. (2008). Adverse childhood experiences and prescription drug use in a cohort study of adult HMO patients. BMC Public Health, 8,198.
Bruskas D & Tessin DH. (2013). Adverse childhood experiences and psychosocial well-being of women who were in foster care as children. The Permanente Journal, 17(3), e131–e141.
Children’s Bureau. (2018). Trends in Foster Care and Adoption: FY 2008 – FY 2017. Available at https://www.acf.hhs.gov/cb/resource/trends-in-foster-care-and-adoption.
Child Welfare Information Gateway. “Rural Child Welfare Practice.” Washington, DC: Children’s Bureau, 2018. Available at https://www.childwelfare.gov/pubPDFs/rural.pdf. Accessed July 10, 2018.
Conron KJ, Beardslee W, Koenen KC, et al. (2009). A longitudinal study of maternal depression and child maltreatment in a national sample of families investigated by child protective services. Archives of Pediatrics & Adolescent Medicine, 163(10), 922.
Dube SR, Felitti VJ, Dong M, et al. (2003). Childhood abuse, neglect, and household dysfunction and the risk of illicit drug use: The adverse childhood experiences study. Pediatrics, 111(3), 564–572.
First Focus Campaign for Children. (March 2018). Family First Prevention Services Act: Bill Summary. Retrieved from https://campaignforchildren.org/wp-content/uploads/sites/2/2016/06/FFCC-Short-Summary-FFPSA.pdf
Felitti, V. J., Anda, R. F., Nordenberg, D., Williamson, D. F., Spitz, A. M., Edwards, V., … Marks, J. S. (1998). Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults. The Adverse Childhood Experiences (ACE) Study. American Journal of Preventive Medicine, 14(4),245–258.
Finkelhor, D., Turner, H. A., Shattuck, A., & Hamby, S. L. (2013). Violence, Crime, and Abuse Exposure in a National Sample of Children and Youth. JAMA Pediatrics, 167(7), 614.
Fin, L. K., Breiding, M. J., Merrick, M. T., Thompson, W. W., Ford, D. C., Dhingra, S. S., & Parks, S. E. (2015). Childhood Adversity and Adult Chronic Disease: An Update from Ten States and the District of Columbia, 2010. American Journal of Preventive Medicine, 48(3), 345–349.
Ghertner, R., and L. Groves. “The Opioid Crisis and Economic Opportunity: Geographic and Economic Trends.” ASPE Research Brief. Washington, DC: U.S. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation, June 29, 2018.
Keyes, K.M., M. Cerdá, J.E. Brady, J.R. Havens, and S. Galea. “Understanding the Rural-Urban Differences in Nonmedical Prescription Opioid Use and Abuse in the United States.” American Journal of Public Health, vol. 104, no. 2, 2014, pp. e52-e59.
Kumpfer KL. Special populations: Etiology and prevention of vulnerability to chemical dependency in children of substance abusers. In Brown BS, Mills AR, Eds., Youth at High Risk for Substance Abuse. Rockville, MD: National Institute on Drug Addiction Research Monograph; 1987.
NIDA. (2016, March 9). Principles of substance abuse prevention for early childhood. Retrieved from https://www.drugabuse.gov/publications/principles-substance-abuse-prevention-early-childhood
Oliveros, A., and J. Kaufman. “Addressing Substance Abuse Treatment Needs of Parents Involved with the Child Welfare System.” Child Welfare, vol. 90, no. 1, 2011, pp. 25–41.
Radel, L., M. Baldwin, G. Crouse, R. Ghertner, and A. Waters. “Substance Use, the Opioid Epidemic, and the Child Welfare System: Key Findings from a Mixed Methods Study.” ASPE Research Brief. Washington, DC: U.S. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation, March 7, 2018.
Rosenblatt, R.A., C.H.A. Andrilla, M. Catlin, and E.H. Larson. “Geographic and Specialty Distribution of US Physicians Trained to Treat Opioid Use Disorder.” Annals of Family Medicine, vol. 13, no. 1, 2015, pp. 23–26. Available at https://doi.org/10.1370/afm.1735. Accessed July 9, 2018.
The President’s Commission on Combating Drug Addiction and the Opioid Crisis. 2017. Available at https://www.whitehouse.gov/sites/whitehouse.gov/files/images/Final_Report_Draft_11-1-2017.pdf.
Vivolo-Kantor A.M., P. Seth, R.M. Gladden, C.L. Mattson, G.T. Baldwin, A. Kite-Powell, and M.A. Coletta. “Vital Signs: Trends in Emergency Department Visits for Suspected Opioid Overdoses—United States, July 2016–September 2017.” Morbidity and Mortality Weekly Report, vol. 67, no. 9, 2018, pp. 279–285. Available at http://dx.doi.org/10.15585/mmwr.mm6709e. Accessed July 16, 2018.
LIST OF ATTACHMENTS – Section A
Note: Attachments are included as separate files as instructed.
Attachment A: Instrument 1 – RCS Discussion Guide for Key Informant Interviews for Wave 1
Attachment B: Instrument 2 – RCS Discussion Guide for Key Informant Interviews for Wave 2 and Site Visit Interviews with Program Administrators
Attachment C: Instrument 3 – RCS Discussion Guide for Site Visit Interviews with Practitioners
Attachment D: Instrument 4 – RCS Discussion Guide for Site Visit Interviews with Partners and Other Related Organizations
Attachment E: RCS Informed Consent
Attachment F. CBS KII–Parents/Caregivers
Attachment G. CBS KII–Providers/Stakeholders
Attachment H. CBS Focus Group Guide–Caregivers
Attachment I. CBS Focus Group Guide–Providers/Stakeholders
Attachment J. CBS Demographic Forms
Attachment K. CBS Informed Consents
| File Type | application/vnd.openxmlformats-officedocument.wordprocessingml.document |
| Author | Matjasko, Jennifer (CDC/DDNID/NCIPC/DVP) |
| File Modified | 0000-00-00 |
| File Created | 2021-01-16 |
© 2026 OMB.report | Privacy Policy