Contact update form
Job Search Assistance Strategies (JSA) Evaluation - Contact updates, Interim Surveys and Six-Month Follow-up Survey
JSA OMB - Attachment A - Welcome Packet and Contact Update Form - 11.17.15
Contact update form
OMB: 0970-0440
Supporting Statement A
For the Paperwork
Reduction Act of 1995:
Approval for the Participant
Tracking, Interim Surveys
and Six-Month Follow-up
Survey for the Job Search
Assistance Strategies
Evaluation
Attachment A: Welcome Packet and Contact Update Form
OMB No. 0970-0440
November 9. 2015
Submitted by:
Office of Planning, Research & Evaluation
Administration for Children & Families
U.S. Department of Health and Human
Services
Federal Project Officer
Erica Zielewski
<First Name> <Last Name>
<Address>
<City>, <State> <ZIPCODE>
<Date>
Dear <First Name> <Last Name>,
Thank you for agreeing to participate in the Job Search Assistance Strategies Evaluation. In the last few weeks, when you applied to participate in the <PROGRAM NAME> in <NAME OF ORGANIZATION> you agreed to participate in research to understand how well training and employment programs work to help people find and keep jobs.
The study is sponsored by the U.S. Department of Health and Human Services (DHHS) Administration for Children and Families (ACF). Abt SRBI is part of a team of research contractors conducting the evaluation. You are one of about 8,000 people across the country who will participate. Your participation in this research helps ACF improve job search assistance programs nationwide.
When you enrolled in the study on <RA DATE>, program staff explained that the research team may follow up with you periodically over the next six months to learn about your experiences since applying for the program. This follow up may include periodic short surveys (about 5 minutes in length) and a longer telephone survey (approximately 20 minutes long) about your job search experiences at the end of the six months. We will provide a token of appreciation for your participation in these surveys. While we hope that you will fully participate in this research, your participation is voluntary and you are not required to participate. Additionally, any information you provide to us will be kept private.
[POST OMB APPROVAL, ADD PARAGRAPH BELOW, SPECIFY TOKEN AMOUNT ABOVE, ADD OMB CONTROL NUMBER AND EXPIRATION DATE:]
To make sure we can reach you for these research activities, we would appreciate it if you could review the contact information on the attached form. Please fill in or update any missing or incorrect contact information. It would also be very helpful if you could provide contact information for three people outside your household with whom you are in touch on a regular basis. We would only contact these individuals if we could not reach you. In consideration of your time, we are including $2 to thank you for responding to this request. Please take just a few minutes to review the enclosed form. If there are any changes please return it to Abt SRBI in the enclosed postage paid envelope. If the information is correct, please retain the form in case you need to update your information in the future. We will periodically get in touch with you to make sure we have the most up-to-date contact information for you. The enclosed brochure provides detailed information about research activities taking place over the next six months and how you can participate.
High quality research depends upon the participation of people like you. We greatly appreciate your willingness to be a part of this important study. Please do not hesitate to contact us at our toll-free number, XXX-XXX-XXXX during regular business hours, with any questions. If you contact us, please refer to your PIN. Your Personal Identification Number (PIN) is: <KEY> Thank you!
Sincerely yours,
Kelly Daley
Project Director
Abt SRBI
According to the Paperwork Reduction Act (PRA), an agency may not conduct or sponsor, and a person is not required to respond to, a collection of information unless it displays a currently valid OMB control number. The OMB control number for this collection is ****-**** and it expires xx/xx/xxxx. If you have comments regarding this burden estimate or any other aspect of this collection of information, including suggestions for reducing this burden, please send them to [Contact Name]; [Contact Address]; Attn: OMB-PRA (xxxxxxx).
JSA STUDY CONTACT UPDATE FORM
(PLEASE PRINT / FAVOR DE ESCRIBIR EN LETRA DE MOLDE)
Is this the correct spelling of your name? / Es éste su nombre correcto?
«firstname» «lastname»
Please check appropriate box. Yes / Sí No, the correct spelling is: / El nombre correcto es
First Name/Nombre |
Last Name/Apellido |
Is this your correct address? / Es esta su dirección correcta?
«street1», «apt», «city», «state» «zip»
Please check appropriate box. Yes / Sí No, my correct address is: / Mi dirección correcta es
Street /Calle |
Apartment # / Número de Apt. |
|
City / Ciudad |
State / Estado |
Zip Code / Código Postal |
Is this your correct phone number? / Es éste su número de teléfono correcto? «phone»
Please check appropriate box. Yes / Sí No, my correct phone number is: / Mi número de teléfono correcto es:
Home Phone / Número de teléfono del hogar |
Cell Phone / Número de teléfono del cellular |
||||||
|
Area Code CODIGO DE AREA |
|
Telephone Number NUMERO DE TELEFONO |
|
Area Code CODIGO DE AREA |
|
Telephone Number NUMERO DE TELEFONO |
Is this your correct email address/ Es éste su email correcto? <<email>>
Please check appropriate box. Yes / Sí No, my correct email address is: / Mi email es:
Email address/Email |
Please list the name, address, and relationship to you of three people who will always know how to reach you.
Por favor escriba los nombres y las direcciones de dos personas quienes sepan cómo ponerse en contacto con usted y explique cómo se relacionan con usted. (PLEASE PRINT / FAVOR DE ESCRIBIR EN LETRA DE MOLDE)
1. Name / Nombre: |
Relation to you / Parentesco con usted: |
|
Address / Dirección |
Apartment # / Número de Apt. |
City / Ciudad |
State / Estado |
Zip Code / Codigo Postal |
Phone / NUMERO DE TELEFONO ( ) — |
2. Name / Nombre: |
Relation to you / Parentesco con usted: |
|
Address / Dirección |
Apartment # / Número de Apt. |
City / Ciudad |
State / Estado |
Zip Code / Codigo Postal |
Phone / NUMERO DE TELEFONO ( ) — |
3. Name / Nombre: |
Relation to you / Parentesco con usted: |
|
Address / Dirección |
Apartment # / Número de Apt. |
City / Ciudad |
According
to the Paperwork Reduction Act (PRA), an agency may not conduct
or sponsor, and a person is not required to respond to, a
collection of information unless it displays a currently valid
OMB control number. The OMB control number for this collection is
0970-0440 and it expires xx/xx/xxxx. If you have comments
regarding this burden estimate or any other aspect of this
collection of information, including suggestions for reducing
this burden, please contact Karin Martinson, Study Project
Director, at (301)-652-7322. |
Zip Code / Codigo Postal |
Phone / NUMERO DE TELEFONO ( ) — |

«PIN»
jOB sEARCH ASSISTANCE STRATEGies EVALUATION
STUDY INFORMATION
The Job Search Assistance Strategies Evaluation is sponsored by the Administration for Children and Families (ACF) in the U.S. Department of Health and Human Services (HHS). Researchers at Abt Associates, Inc are conducting interviews with people who agreed to be in a study about a program offered at [NAME OF ORGANIZATION] called [PROGRAM NAME.] You agreed to be part of the study around [RAD]. You may recall signing a consent form and completing a short survey at that time.
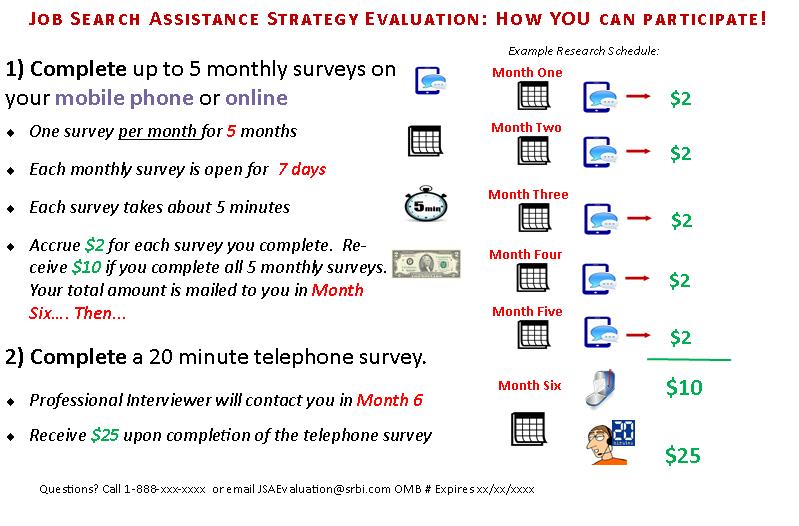
This research has two parts: five (5) brief monthly surveys between [RA date] and [six-month post RA date] and a telephone survey 6 months from now. We have enclosed a summary of this research on the attached card.
Monthly Surveys
If you agreed to receive texts from the study team, we will send you a text message each month, inviting you to take a short survey. The surveys contain brief questions related to the job search process and offer the chance to confirm or update your contact information. If you do not have a cell phone we will send you an email with a link to complete the monthly survey online. It takes about 5 minutes to complete each monthly survey.
The text surveys remain open for 7 days from the initial invitation, and you may answer the questions at any time during that 7-day period. Each time you complete one of these monthly surveys, you will “accrue” $2 as a token of our appreciation for your time. By “accrue”, we mean that the money you earn for completing each survey will be saved and sent to you in one check around [INSERT DATE OF 6 MO INTERVIEW]. You can earn $2, $4, $6, $8 or $10 depending upon how many of these monthly surveys you complete. For example, if you complete two surveys, you will receive $4, if you complete five surveys, you will receive $10. You can complete any one or all of the surveys. We will include the total amount of money you banked with a letter thanking you for participating in these short surveys and provide more information about the next part of the study.
If you choose to participate in the monthly text surveys, please
respond at a time and place when it is safe for you to respond.
Standard text message fees may apply and depend upon your individual plan. Your responses to these surveys will not affect your participation in any programs or your receipt of any kinds of public benefits or services. All of your responses on this survey will be kept private.
Six-Month Telephone Survey
You are eligible to participate in a 20-minute telephone survey to help researchers learn more detail about your job search experiences since applying for the [PROGRAM NAME]. You will be invited to participate in this survey whether or not you participated in the monthly text surveys. The telephone survey includes more detailed questions about you and your employment and job search experiences over the last six months. Like the text surveys, your participation is voluntary. This means you do not have to answer any of the questions and you can stop the survey at any time. Information that could identify you is kept separate from your survey responses. Any information you provide to us will be kept private. Any published reports on this research will summarize results from all 8,000 participants.
A professional interviewer will contact you to conduct the interview at a time that is most convenient for you. In appreciation of your time, we will mail you $25 for completing the telephone survey.
For more information on this study you may contact:
Email: JSAEVALUATION@srbi.com Phone: 888-xxx-xxxx
To update your contact information online, please go to www.JSAUPDATE.com and enter the pin provided in your invitation letter.
If you have questions about your rights as a study participant, you can contact the Abt Associates IRB at:
Email: irb@abtassoc.com Phone: ABT IRB TOLL FREE NUMBER
According to the Paperwork Reduction Act (PRA), an agency may not conduct or sponsor, and a person is not required to respond to, a collection of information unless it displays a currently valid OMB control number. The OMB control number for this collection is ****-**** and it expires xx/xx/xxxx. If you have comments regarding this burden estimate or any other aspect of this collection of information, including suggestions for reducing this burden, please send them to [Contact Name]; [Contact Address]; Attn: OMB-PRA (xxxxxxx).
| File Type | application/vnd.openxmlformats-officedocument.wordprocessingml.document |
| Author | Martina Smith |
| File Modified | 0000-00-00 |
| File Created | 2021-01-22 |
© 2026 OMB.report | Privacy Policy