Businesses - Sponsors and Providers
Study of Nutrition and Activity in Child Care Settings
Appendix E3 Infant Food Intake Form Final 11.2.15
Businesses - Sponsors and Providers
OMB: 0584-0615
E.3 Infant Food Intake Form
OMB
Control No: 0584-XXXX OMB
Approval Expiration Date: XX/XX/XXXX
LOGO
Study on Nutrition and Activity in
Child Care Settings (SNACS)
Infant Food Intake
Child
Care Center ID
Target
Week
Caregiver Initials: | | |
According to the Paperwork Reduction Act of 1995, an agency may not conduct or sponsor, and a person is not required to respond to, a collection of information unless it displays a valid OMB control number. The valid OMB control number for this information collection is 0584-XXXX .The time required to complete this information collection is estimated to average 10 minutes per infant (for an estimated total of 50 minutes per infant care provider), including the time for reviewing instructions, searching existing data sources, gathering and maintaining the data needed, and completing and reviewing the collection of information. |
About the Study. The Study on Nutrition and Activity in Child Care Settings is intended to study nutrition and activity in child care centers, family day care homes, afterschool programs, and at-risk programs participating in the Child and Adult Care Food Program (CACFP) and some not participating in the CACFP. More than 1,500 child care providers in over 20 states were selected to be part of the study. Abt Associates is conducting this study for the USDA Food and Nutrition Service (FNS).
About this Booklet. This booklet is to be filled out by the infant care provider, and will be used to collect information about the foods and beverages consumed by up to three infants for one day, and the time of each feeding while in the provider’s care. This includes foods brought in from home as well as prepared at the center. The infant care provider will receive $5 for completing the form for each sampled infant.
Protecting Privacy. All information gathered from child care sponsors, child care centers, family day care homes, child care administrators and staff, and families participating in this study is for research purposes only and will be kept private to the full extent allowed by law. Responses will be grouped with those of other study participants, and no individual participants, program administrators, program staff, parents, or children will be identified in any study report.
Questions. If you have any questions about the study please call our toll-free study number at 1-844-808-4777 or email SNACS@abtassoc.com. We will be happy to answer your questions and to help you in any way we can.
Thank you for participating in the Study on Nutrition and Activity in Child Care Settings.
Tab 1
Instructions
This page has been left blank for double-sided printing
INSTRUCTIONS
Please use this form to record all the foods, drinks, formula, and/or breast milk you served to the infants being observed while he/she is in your child care facility on the day noted on the front cover. Please be sure to include anything brought in from home by the parent or guardian that was served to the infant.
USE ONE BOOKLET FOR THREE INFANTS:
One booklet should be used to record the intake of up to three infants on one day. Each infant care provider will receive one booklet to record information for these three infants. Write the name of the infant on each separate form, found on Tabs 4, 5 and 6.
This booklet contains:
TAB 1: Instructions
TAB 2: Measurement Guide
TAB 3: Example of a completed Infant Intake Form
TAB 4: Infant Intake Form – Infant 1
TAB 5: Infant Intake Form – Infant 2
TAB 6: Infant Intake Form – Infant 3
Each infant should be recorded in a separate tab (space for 3 infants is provided)
HOW TO FILL OUT THIS BOOKLET
Fill out the information at the top of the form: Date, Day of the Week, Infant Name, Infant Birthdate, Age Group of Infant, and Gender. When selecting the age group, keep in mind the age groups are as follows:
Birth through 3 months
4 through 5 months
6 through 7 months
8 through 11 months
For example, you would circle 6 - 7 months for an infant who is 7.5 months old.
Then follow the instructions at the top of each column:
Time of Feeding
Write down the time you started each feeding, including a.m. or p.m. This will help you keep track of the feedings you have recorded.
What Did You Serve or Feed (to the Infant)?
For each feeding, write down everything you fed to the infant, including formula, breast milk, solid foods (including purees and blended/mashed foods), snacks, and any other drinks. Use a separate row for each food or beverage.
If you serve juice, please indicate if it is 100% juice in the “What did you serve or feed” column. Please see the last row of the example form.
Check the box to indicate whether the food or drink was brought from home or prepared in the center.
Please also list any time the mother comes to the center and nurses the infant being observed in the center. You can indicate this by selecting the checkbox labeled “mom nursed” in the “What did you serve or feed” column.
Do not worry about recording the amount of breast milk consumed during nursing sessions. Simply write “N/A” for not applicable in the last column. Please see the first row of the example form.
How Much Did the Infant Eat or Drink?
Write down how much of each item the sampled infant ate or drank.
If you use standard measuring tools:
For liquids (formula, breast milk, water, juice, whole milk, and any other liquids or drinks), record amount eaten in fluid ounces. Do NOT record liquids in numbers of cups. For example, write “4 fl. oz.” NOT “1/2 cup”
For foods, use standard measures such as “1 Tablespoon”. Do NOT use non-standard measures such as “two bites”.
For certain foods such as a banana or apple, you may write how much the child ate from the whole fruit, such as “½ apple” then fill in the blank next to the last check box by writing “whole” for the unit of measure. You can write the word “piece” or “whole” in the blank space.
Write down the number or fraction of teaspoons, tablespoons, ounces or cups.
Below is a list of conversions for your convenience.
8 fluid Oz = 1 cup
3 level teaspoons (tsp) = 1 level Tablespoon (TB)
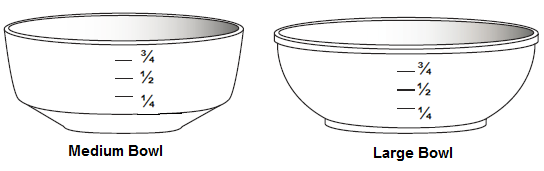
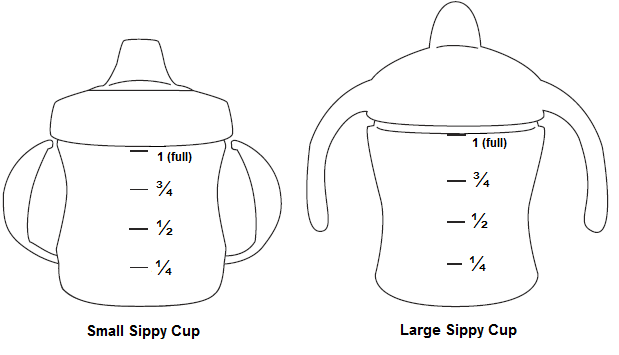
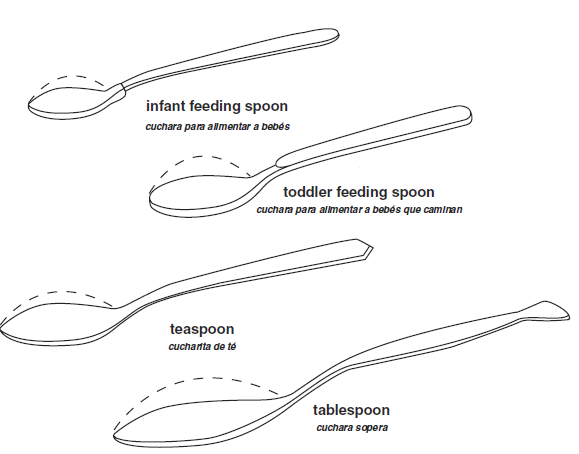
If you do not use standard measuring tools:
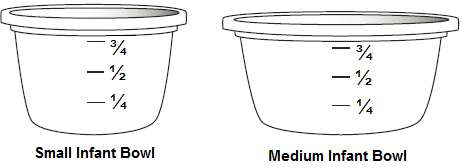
Use the images found on the following pages to estimate how much the infant ate or drank
Indicate which serving dish was used (bowl, cup, spoon) by writing the code found beneath the image (B1, B2, B3, B4, C1, C2, S1, S2, S3, S4)
Estimate how much was eaten (None, ¼ . ½, ¾, All); for spoons, indicate whether the spoonful was mounded or not
Add a checkmark to the final column of the Infant Intake Module Form to indicate that you used the Measurement Guide to approximate the amount consumed.

This page has been left blank for double-sided printing
Tab 2
Measurement Guide
This page has been left blank for double-sided printing
Measurement Guide
B
2
B
1
Infant
Bowls

Child
Bowls
B
4
B
3

Measurement Guide, continued
Sippy
Cups
C
2
C
1

Measurement
Guide, continued
Standard
Spoons
Infant
Spoons
S
4 (tablespoon)
S
1
S2
S
3 (teaspoon)
S
1








If you have any questions, please talk with the study team member that is at your program today. If you are unable to talk with the study team member while they are onsite, please call (toll-free) Abt Associates at 1- 844-808-4777 or email Abt Associates at SNACS@abtassoc.com.
Thank you very much for your help with this important study.
Tab 3
Example of a Completed Infant Intake Form
This page has been left blank for double-sided printing
Child ID #: | | | | | | |
Today’s Date: ______ ______ ______

Day of the Week (Please circle one): MON TUES WED THURS FRI
INFANT FOOD INTAKE FORM

 Name
of infant:__Jackson
Smith_______
Birthdate
of infant:___9/25/15____________
Gender (circle one): M F
Name
of infant:__Jackson
Smith_______
Birthdate
of infant:___9/25/15____________
Gender (circle one): M F
Age of Infant (please circle one): 0 – 3 months 4 – 5 months 6 – 7 months 8 months through 11 months
Office Use Only |
Time of Feeding |
What did you serve or feed? Use one line for each food or drink. (List all formula, breast milk, foods and drinks) |
How much did the infant eat or drink? (Include units: Fluid ounces (FL OZ), cups, teaspoons (tsp), Tablespoons (TB), or other |
If you used the Measurement Guide to estimate amount consumed, check box. |
|||
Food |
Drink/Beverage |
Measurement Guide? |
|||||
1 |
8:00am |
Breast milk From home From provider Mom nursed |
|
Cups tsp TB ______ |
N/A |
FL OZ |
|
2 |
10:00am |
Apple Sauce From home From provider Mom nursed |
2 |
Cups tsp TB ______ |
|
FL OZ |
|
3 |
12:00pm |
Oatmeal From home From provider Mom nursed |
1/4 |
Cups tsp TB ______ |
|
FL OZ |
|
4 |
12:00pm |
Breast milk From home From provider Mom nursed |
|
Cups tsp TB ______ |
5 |
FL OZ |
|
5 |
12:00pm |
Banana, From home mashed From provider Mom nursed |
1/4 |
Cups tsp TB whole |
|
FL OZ |
|
6 |
3:00pm |
Breast milk From home From provider Mom nursed |
|
Cups tsp TB ______ |
6 |
FL OZ |
|
7 |
3:00pm |
100% Juice : Apple From home From provider Mom nursed |
|
Cups tsp TB ______ |
¼ C1 |
FL OZ |
|
The Infant Food Intake Form was adapted from the Infant Food Intake Record used in the Early Childhood and Childcare Study and the Childcare Food Information Form from the Feeding Infants in Childcare Study (FITS).
This page has been left blank for double-sided printing
Tab 4
Infant Intake Form—Infant 1
This page has been left blank for double-sided printing
OMB
Control No: 0584-XXXX OMB
Approval Expiration Date: XX/XX/XXXX
Infant
1
INFANT
FOOD INTAKE FORM

This page has been left blank for double-sided printing
Child ID #: | | | | | | |
Today’s Date: ______ ______ ______
Day of the Week (Please circle one): MON TUES WED THURS FRI
INFANT FOOD INTAKE FORM
Name of infant:________________________ Birthdate of infant:_______________ Gender (circle one): M F
Age of Infant (please circle one): 0 – 3 months 4 – 5 months 6 – 7 months 8 months through 11 months
Office Use Only |
Time of Feeding |
What did you serve or feed? Use one line for each food or drink. (List all formula, breast milk, foods and drinks) |
How much did the infant eat or drink? (Include units: Fluid ounces (FL OZ), cups, teaspoons (tsp), Tablespoons (TB), or other |
If you used the Measurement Guide to estimate amount consumed, check box. |
|||
Food |
Drink/Beverage |
Measurement Guide? |
|||||
1 |
|
From home From provider Mom nursed |
|
Cups tsp TB _____ |
|
FL OZ |
|
2 |
|
From home From provider Mom nursed |
|
Cups tsp TB _____ |
|
FL OZ |
|
3 |
|
From home From provider Mom nursed |
|
Cups tsp TB _____ |
|
FL OZ |
|
4 |
|
From home From provider Mom nursed |
|
Cups tsp TB _____ |
|
FL OZ |
|
5 |
|
From home From provider Mom nursed |
|
Cups tsp TB _____ |
|
FL OZ |
|
6 |
|
From home From provider Mom nursed |
|
Cups tsp TB _____ |
|
FL OZ |
|
7 |
|
From home From provider Mom nursed |
|
Cups tsp TB _____ |
|
FL OZ |
|
INFANT FOOD INTAKE FORM continued
Office Use Only |
Time of Feeding |
What did you serve or feed? Use one line for each food or drink. (List all formula, breast milk, foods and drinks) |
How much did the infant eat or drink? (Include units: Fluid ounces (FL OZ), cups, teaspoons (tsp), Tablespoons (TB), or other |
If you used the Measurement Guide to estimate amount consumed, check box. |
|||
Food |
Drink/Beverage |
Measurement Guide? |
|||||
8 |
|
From home From provider Mom nursed |
|
Cups tsp TB _____ |
|
FL OZ |
|
9 |
|
From home From provider Mom nursed |
|
Cups tsp TB _____ |
|
FL OZ |
|
10 |
|
From home From provider Mom nursed |
|
Cups tsp TB _____ |
|
FL OZ |
|
11 |
|
From home From provider Mom nursed |
|
Cups tsp TB _____ |
|
FL OZ |
|
12 |
|
From home From provider Mom nursed |
|
Cups tsp TB _____ |
|
FL OZ |
|
13 |
|
From home From provider Mom nursed |
|
Cups tsp TB _____ |
|
FL OZ |
|
14 |
|
From home From provider Mom nursed |
|
Cups tsp TB _____ |
|
FL OZ |
|
15 |
|
From home From provider Mom nursed |
|
Cups tsp TB _____ |
|
FL OZ |
|
Office Use Only |
Time of Feeding |
What did you serve or feed? Use one line for each food or drink. (List all formula, breast milk, foods and drinks) |
How much did the infant eat or drink? (Include units: Fluid ounces (FL OZ), cups, teaspoons (tsp), Tablespoons (TB), or other |
If you used the Measurement Guide to estimate amount consumed, check box. |
|||
Food |
Drink/Beverage |
Measurement Guide? |
|||||
16 |
|
From home From provider Mom nursed |
|
Cups tsp TB _____ |
|
FL OZ |
|
17 |
|
From home From provider Mom nursed |
|
Cups tsp TB _____ |
|
FL OZ |
|
18 |
|
From home From provider Mom nursed |
|
Cups tsp TB _____ |
|
FL OZ |
|
19 |
|
From home From provider Mom nursed |
|
Cups tsp TB _____ |
|
FL OZ |
|
20 |
|
From home From provider Mom nursed |
|
Cups tsp TB _____ |
|
FL OZ |
|
21 |
|
From home From provider Mom nursed |
|
Cups tsp TB _____ |
|
FL OZ |
|
22 |
|
From home From provider Mom nursed |
|
Cups tsp TB _____ |
|
FL OZ |
|
23 |
|
From home From provider Mom nursed |
|
Cups tsp TB _____ |
|
FL OZ |
|
24 |
|
From home From provider Mom nursed |
|
Cups tsp TB _____ |
|
FL OZ |
|
The Infant Food Intake Form was adapted from the Infant Food Intake Record used in the Early Childhood and Childcare Study and the Childcare Food Information Form from the Feeding Infants in Childcare Study (FITS).
This page has been left blank for double-sided printing
Tab 5
Infant Intake Form—Infant 2
This page has been left blank for double-sided printing
OMB
Control No: 0584-XXXX OMB
Approval Expiration Date: XX/XX/XXXX
Infant
2
INFANT
FOOD INTAKE FORM
Child ID #: | | | | | | |
Today’s Date: ______ ______ ______
Day of the Week (Please circle one): MON TUES WED THURS FRI
INFANT FOOD INTAKE FORM
Name of infant:________________________ Birthdate of infant:_______________ Gender (circle one): M F
Age of Infant (please circle one): 0 – 3 months 4 – 5 months 6 – 7 months 8 months through 11 months
Office Use Only |
Time of Feeding |
What did you serve or feed? Use one line for each food or drink. (List all formula, breast milk, foods and drinks) |
How much did the infant eat or drink? (Include units: Fluid ounces (FL OZ), cups, teaspoons (tsp), Tablespoons (TB), or other |
If you used the Measurement Guide to estimate amount consumed, check box. |
|||
Food |
Drink/Beverage |
Measurement Guide? |
|||||
1 |
|
From home From provider Mom nursed |
|
Cups tsp TB _____ |
|
FL OZ |
|
2 |
|
From home From provider Mom nursed |
|
Cups tsp TB _____ |
|
FL OZ |
|
3 |
|
From home From provider Mom nursed |
|
Cups tsp TB _____ |
|
FL OZ |
|
4 |
|
From home From provider Mom nursed |
|
Cups tsp TB _____ |
|
FL OZ |
|
5 |
|
From home From provider Mom nursed |
|
Cups tsp TB _____ |
|
FL OZ |
|
6 |
|
From home From provider Mom nursed |
|
Cups tsp TB _____ |
|
FL OZ |
|
7 |
|
From home From provider Mom nursed |
|
Cups tsp TB _____ |
|
FL OZ |
|
INFANT FOOD INTAKE FORM continued
Office Use Only |
Time of Feeding |
What did you serve or feed? Use one line for each food or drink. (List all formula, breast milk, foods and drinks) |
How much did the infant eat or drink? (Include units: Fluid ounces (FL OZ), cups, teaspoons (tsp), Tablespoons (TB), or other |
If you used the Measurement Guide to estimate amount consumed, check box. |
|||
Food |
Drink/Beverage |
Measurement Guide? |
|||||
8 |
|
From home From provider Mom nursed |
|
Cups tsp TB _____ |
|
FL OZ |
|
9 |
|
From home From provider Mom nursed |
|
Cups tsp TB _____ |
|
FL OZ |
|
10 |
|
From home From provider Mom nursed |
|
Cups tsp TB _____ |
|
FL OZ |
|
11 |
|
From home From provider Mom nursed |
|
Cups tsp TB _____ |
|
FL OZ |
|
12 |
|
From home From provider Mom nursed |
|
Cups tsp TB _____ |
|
FL OZ |
|
13 |
|
From home From provider Mom nursed |
|
Cups tsp TB _____ |
|
FL OZ |
|
14 |
|
From home From provider Mom nursed |
|
Cups tsp TB _____ |
|
FL OZ |
|
15 |
|
From home From provider Mom nursed |
|
Cups tsp TB _____ |
|
FL OZ |
|
Office Use Only |
Time of Feeding |
What did you serve or feed? Use one line for each food or drink. (List all formula, breast milk, foods and drinks) |
How much did the infant eat or drink? (Include units: Fluid ounces (FL OZ), cups, teaspoons (tsp), Tablespoons (TB), or other |
If you used the Measurement Guide to estimate amount consumed, check box. |
|||
Food |
Drink/Beverage |
Measurement Guide? |
|||||
16 |
|
From home From provider Mom nursed |
|
Cups tsp TB _____ |
|
FL OZ |
|
17 |
|
From home From provider Mom nursed |
|
Cups tsp TB _____ |
|
FL OZ |
|
18 |
|
From home From provider Mom nursed |
|
Cups tsp TB _____ |
|
FL OZ |
|
19 |
|
From home From provider Mom nursed |
|
Cups tsp TB _____ |
|
FL OZ |
|
20 |
|
From home From provider Mom nursed |
|
Cups tsp TB _____ |
|
FL OZ |
|
21 |
|
From home From provider Mom nursed |
|
Cups tsp TB _____ |
|
FL OZ |
|
22 |
|
From home From provider Mom nursed |
|
Cups tsp TB _____ |
|
FL OZ |
|
23 |
|
From home From provider Mom nursed |
|
Cups tsp TB _____ |
|
FL OZ |
|
24 |
|
From home From provider Mom nursed |
|
Cups tsp TB _____ |
|
FL OZ |
|
The Infant Food Intake Form was adapted from the Infant Food Intake Record used in the Early Childhood and Childcare Study and the Childcare Food Information Form from the Feeding Infants in Childcare Study (FITS).
Tab 6
Infant Intake Form—Infant 3
This page has been left blank for double-sided printing
OMB
Control No: 0584-XXXX OMB
Approval Expiration Date: XX/XX/XXXX
Infant
3
INFANT
FOOD INTAKE FORM
Child ID #: | | | | | | |
Today’s Date: ______ ______ ______
Day of the Week (Please circle one): MON TUES WED THURS FRI
INFANT FOOD INTAKE FORM
Name of infant:________________________ Birthdate of infant:_______________ Gender (circle one): M F
Age of Infant (please circle one): 0 – 3 months 4 – 5 months 6 – 7 months 8 months through 11 months
Office Use Only |
Time of Feeding |
What did you serve or feed? Use one line for each food or drink. (List all formula, breast milk, foods and drinks) |
How much did the infant eat or drink? (Include units: Fluid ounces (FL OZ), cups, teaspoons (tsp), Tablespoons (TB), or other |
If you used the Measurement Guide to estimate amount consumed, check box. |
|||
Food |
Drink/Beverage |
Measurement Guide? |
|||||
1 |
|
From home From provider Mom nursed |
|
Cups tsp TB _____ |
|
FL OZ |
|
2 |
|
From home From provider Mom nursed |
|
Cups tsp TB _____ |
|
FL OZ |
|
3 |
|
From home From provider Mom nursed |
|
Cups tsp TB _____ |
|
FL OZ |
|
4 |
|
From home From provider Mom nursed |
|
Cups tsp TB _____ |
|
FL OZ |
|
5 |
|
From home From provider Mom nursed |
|
Cups tsp TB _____ |
|
FL OZ |
|
6 |
|
From home From provider Mom nursed |
|
Cups tsp TB _____ |
|
FL OZ |
|
7 |
|
From home From provider Mom nursed |
|
Cups tsp TB _____ |
|
FL OZ |
|
INFANT FOOD INTAKE FORM continued
Office Use Only |
Time of Feeding |
What did you serve or feed? Use one line for each food or drink. (List all formula, breast milk, foods and drinks) |
How much did the infant eat or drink? (Include units: Fluid ounces (FL OZ), cups, teaspoons (tsp), Tablespoons (TB), or other |
If you used the Measurement Guide to estimate amount consumed, check box. |
|||
Food |
Drink/Beverage |
Measurement Guide? |
|||||
8 |
|
From home From provider Mom nursed |
|
Cups tsp TB _____ |
|
FL OZ |
|
9 |
|
From home From provider Mom nursed |
|
Cups tsp TB _____ |
|
FL OZ |
|
10 |
|
From home From provider Mom nursed |
|
Cups tsp TB _____ |
|
FL OZ |
|
11 |
|
From home From provider Mom nursed |
|
Cups tsp TB _____ |
|
FL OZ |
|
12 |
|
From home From provider Mom nursed |
|
Cups tsp TB _____ |
|
FL OZ |
|
13 |
|
From home From provider Mom nursed |
|
Cups tsp TB _____ |
|
FL OZ |
|
14 |
|
From home From provider Mom nursed |
|
Cups tsp TB _____ |
|
FL OZ |
|
15 |
|
From home From provider Mom nursed |
|
Cups tsp TB _____ |
|
FL OZ |
|
Office Use Only |
Time of Feeding |
What did you serve or feed? Use one line for each food or drink. (List all formula, breast milk, foods and drinks) |
How much did the infant eat or drink? (Include units: Fluid ounces (FL OZ), cups, teaspoons (tsp), Tablespoons (TB), or other |
If you used the Measurement Guide to estimate amount consumed, check box. |
|||
Food |
Drink/Beverage |
Measurement Guide? |
|||||
16 |
|
From home From provider Mom nursed |
|
Cups tsp TB _____ |
|
FL OZ |
|
17 |
|
From home From provider Mom nursed |
|
Cups tsp TB _____ |
|
FL OZ |
|
18 |
|
From home From provider Mom nursed |
|
Cups tsp TB _____ |
|
FL OZ |
|
19 |
|
From home From provider Mom nursed |
|
Cups tsp TB _____ |
|
FL OZ |
|
20 |
|
From home From provider Mom nursed |
|
Cups tsp TB _____ |
|
FL OZ |
|
21 |
|
From home From provider Mom nursed |
|
Cups tsp TB _____ |
|
FL OZ |
|
22 |
|
From home From provider Mom nursed |
|
Cups tsp TB _____ |
|
FL OZ |
|
23 |
|
From home From provider Mom nursed |
|
Cups tsp TB _____ |
|
FL OZ |
|
24 |
|
From home From provider Mom nursed |
|
Cups tsp TB _____ |
|
FL OZ |
|
The Infant Food Intake Form was adapted from the Infant Food Intake Record used in the Early Childhood and Childcare Study and
the Childcare Food Information Form from the Feeding Infants in Childcare Study (FITS).
| File Type | application/vnd.openxmlformats-officedocument.wordprocessingml.document |
| Author | Tara Wommack |
| File Modified | 0000-00-00 |
| File Created | 2021-01-24 |
© 2026 OMB.report | Privacy Policy