Evaluation Questionnaire: Follow-up month 8
WHAM: Women Health and Mindfulness Program
19144 ID_(WHAM) Women's Health and Mindfulness Program - Mindfulness Study Evaluation Questionnaire Follow-up Month 8
Evaluation Questionnaire: Follow-up month 8
OMB: 0990-0414
Form Approved
OMB No. 0990-
Exp. Date XX/XX/20XX
Mindfulness Study Evaluation Questionnaire Follow-up Month 8 (WHAM) Women’s Health and Mindfulness
Program
To be completed by the interviewer.
1.1 PARTICIPANT ID: _____ _____
1.2 INTERVIEWER ID: _____
1.3 DATE OF INTERVIEW: _____ _____ / _____ _____ / 2 0 _____ _____ (MM/DD/YY)
1.4 INTERVIEW BEGIN TIME: _____ _____ : _____ _____ AM / PM
1.5 INTERVIEW END TIME: _____ _____ : _____ _____ AM / PM
1.6 STUDY VISIT NUMBER (CIRCLE ONE): 2 3
Read introduction:
We are ready to begin the interview. Please remember that your answers will not be shared with anyone outside the study team. Your answers will be put together with all the other participants’ answers to help us learn more about lesbian and bisexual women's health. For this reason, your honest answers are very important.
Remember that you are not being judged based on your answers and there are no right or wrong answers. Some of the questions ask about personal topics about your health and you may feel uncomfortable answering some of them. You can skip questions, end the interview, or ask me to repeat or explain anything at any time. If you have any questions or want to talk about certain things that come up during the interview, let me know and I will make a note of it to talk to you when we finish. Do you have any questions before we begin?
These questions will be familiar to you from your first interview with us. Some things may be the same for you and other things may have changed.
CODING NOTE TO INTERVIEWERS: DON’T KNOW=-8; DECLINED=-9.
II. Sociodemographics
To begin, I would like to ask about whether you are working now.
*What is your current employment status?
_____1 Working part-time (less than 32 hours/week)
_____2 Working full-time (32 or more hours/week)
_____3 Unemployed, laid off, on strike
_____4 Retired
_____5 Disabled or unable to work
_____6 In school full time and not working
_____7 Full-time homemaker
*Quality of Life (VR-12 Survey): The next part of the interview will ask some general questions about how you see your health.
2.13 In general, would you say your health is:
_____1 Excellent
_____2 Very good
_____3 Good
_____4 Fair
_____5 Poor
2.14 The following questions are about activities you might do during a typical day. Does your health now limit you in these activities? If so, how much?
2.14A. Moderate activities, such as moving a table, pushing a vacuum cleaner, bowling or playing golf?
_____1 Yes, limited a lot
_____2 Yes, limited a little
_____3 No, not limited at all
2.14B. Climbing several flights of stairs?
_____1 Yes, limited a lot
_____2 Yes, limited a little
_____3 No, not limited at all
During the past 4 weeks, have you had any of the following problems with your work or other regular daily activities as a result of your physical health?
2.15A. Accomplished less than you would like.
_____1 No, none of the time
_____2 Yes, a little of the time
_____3 Yes, some of the time
_____4 Yes, most of the time
_____5 Yes, all of the time
2.15B. Were limited in the kind of work or other activities.
_____1 No, none of the time
_____2 Yes, a little of the time
_____3 Yes, some of the time
_____4 Yes, most of the time
_____5 Yes, all of the time
2.16 During the past 4 weeks, have you had any of the following problems with your work or other regular daily activities as a result of any emotional problems (such as feeling depressed or anxious)?
2.16A. Accomplished less than you would like.
_____1 No, none of the time
_____2 Yes, a little of the time
_____3 Yes, some of the time
_____4 Yes, most of the time
_____5 Yes, all of the time
2.16B. Didn’t do work or other activities as carefully as usual
.
_____1 No, none of the time
_____2 Yes, a little of the time
_____3 Yes, some of the time
_____4 Yes, most of the time
_____5 Yes, all of the time
During the past 4 weeks, how much did pain interfere with your normal work (including both work outside the home and housework)?
_____1 Not at all
_____2 A little bit
_____3 Moderately
_____4 Quite a bit
_____5 Extremely
These questions are about how you feel and how things have been with you during the past 4 weeks. For each question, please give the one answer that comes closest to the way you have been feeling.
2.18 How much of the time during the past 4 weeks:
Have you felt calm and peaceful?
_____1 All of the time
_____2 Most of the time
_____3 A good bit of the time
_____4 Some of the time
_____5 A little bit of the time
_____6 None of the time
2.19 How much of the time during the past 4 weeks:
Did you have a lot of energy?
_____1 All of the time
_____2 Most of the time
_____3 A good bit of the time
_____4 Some of the time
_____5 A little bit of the time
_____6 None of the time
2.19 How much of the time during the past 4 weeks:
Have you felt downhearted and blue?
_____1 All of the time
_____2 Most of the time
_____3 A good bit of the time
_____4 Some of the time
_____5 A little bit of the time
_____6 None of the time
2.20. During the past 4 weeks, how much of the time has your physical health or emotional problems interfered with your social activities (like visiting with friends, relatives, etc.)?
_____1 All of the time
_____2 Most of the time
_____3 Some of the time
_____4 A little of the time
_____5 None of the time
Now, we’d like to ask you some questions about how your health may have changed.
2.21. Compared to one year ago, how would you rate your physical health in general now?
_____1 Much better
_____2 Slightly better
_____3 About the same
_____4 Slightly worse
_____5 Much worse
2.22. Compared to one year ago, how would you rate your emotional problems (such as feeling anxious, depressed or irritable) now?
_____1 Much better
_____2 Slightly better
_____3 About the same
_____4 Slightly worse
_____5 Much worse
III. Health Behaviors
We are interested in finding out about the kinds of physical activities that people do as part of their everyday lives. The questions will ask you about the time you spent being physically active in the last 7 days. Please answer each question even if you do not consider yourself to be an active person. Please think about the activities you do at work, as part of your house and yard work, to get from place to place, and in your spare time for recreation, exercise or sport.
SHOW PARTICIPANT PHYSICAL ACTIVITY IMAGE CARD.
Think about all the vigorous activities that you did in the last 7 days. Vigorous physical activities take hard physical effort and make you breathe much harder than normal. Think only about those physical activities that you did for at least 10 minutes at a time.
*During the last 7 days, on how many days did you do vigorous physical activities like heavy lifting, digging, aerobics, or fast bicycling?
_____ days in the last week if 0, skip to 3.3
*How much time did you usually spend doing vigorous physical activities on one of those days?
_____1 Hour(s) per day
_____2 Minutes per day
_____3 Don’t know/not sure
Think about all the moderate activities that you did in the last 7 days. Moderate activities take moderate physical effort and make you breathe somewhat harder than normal. Think only about those physical activities that you did for at least 10 minutes at a time.
*During the last 7 days, on how many days did you do moderate physical activities like carrying light loads, bicycling at a regular pace, or doubles tennis? Do not include walking.
_____ days in the last week if 0, skip to 3.5
*How much time did you usually spend doing moderate physical activities on one of those days?
_____1 Hour(s) per day
_____2 Minutes per day
_____3 Don’t know/not sure
Now, think about the time you spent walking in the last 7 days. This includes at work and at home, walking to travel from place to place, and any other walking that you might do solely for recreation, sport, exercise, or leisure.
*During the last 7 days, on how many days did you walk for at least 10 minutes at a time?
_____ days in the last week if 0, skip to 3.7
*How much time did you usually spend walking on one of those days?
_____1 Hour(s) per day
_____2 Minutes per day
_____3 Don’t know/not sure
The last question is about the time you spent sitting on weekdays during the last 7 days. Include time spent at work, at home, while doing course work and during leisure time. This may include time spent sitting at a desk, visiting friends, reading, or sitting or lying down to watch television.
*During the last 7 days, how much time did you spend sitting on a week day?
_____1 Hour(s) per day
_____2 Minutes per day
_____3 Don’t know/not sure
The next section is about the foods you ate or drank during the past 30 days, including meals and snacks. Remember to include any sweetened beverages used as a mixer for cocktails.
*During the past 30 days, how often did you drink regular soda or pop that contains sugar? Do not include diet soda.
_____1 Times per day
_____2 Times per week
_____3 Times per month
_____4 Never
*During the past 30 days, how often did you drink diet soda or pop that contains artificial sweeteners?
_____1 Times per day
_____2 Times per week
_____3 Times per month
_____4 Never
*During the past 30 days, how often did you drink sports or energy drinks such as Gatorade, Red Bull or Vitamin Water. Remember to use include sports or energy drinks used as a mixer? Do not include diet or sugar-free kinds.
_____1 Times per day
_____2 Times per week
_____3 Times per month
_____4 Never
*During the past 30 days, how often did you drink sweetened fruit drinks such as Kool-aid, cranberry drink or lemonade? Include fruit drinks you made at home and added sugar to. Do not include 100% fruit juices and drinks with things like Splenda or Equal.
_____1 Times per day
_____2 Times per week
_____3 Times per month
_____4 Never
*During the past 30 days, how often did you drink coffee or tea with sugar or honey added? Do not include drinks with things like Splenda or Equal. Include pre-sweetened tea and coffee drinks such as Arizona Iced Tea and Frappuccino.
_____1 Times per day
_____2 Times per week
_____3 Times per month
_____4 Never
*During the past 30 days, how often did you drink water (including tap, bottled, and carbonated water)?
_____1 Times per day
_____2 Times per week
_____3 Times per month
_____4 Never
*Each time you drank water, how much did you usually drink?
_____1 Less than 6 fl oz (3/4 oz)
_____2 8 fl oz (1 cup)
_____3 12 fl oz (1-1/2 cups)
_____4 16 fl oz (2 cups)
_____5 More than 20 fl oz (2-1/2 cups)
*During the past 30 days, how many times per day, week or month did you drink 100% PURE fruit juices? Do not include fruit-flavored drinks with added sugar or fruit juice you made at home and added sugar to. Only include 100% juice.
_____1 Times per day
_____2 Times per week
_____3 Times per month
_____4 Never
*During the past 30 days, not counting juice, how many times per day, week or month did you eat fruit? Count fresh, frozen or canned fruit.
_____1 Times per day
_____2 Times per week
_____3 Times per month
_____4 Never
*During the past 30 days, how many times per day, week or month did you eat cooked or canned beans, such as refried, black, garbanzo beans, beans in soup, soybeans, edamame, tofu or lentils. Do NOT include long green beans.
_____1 Times per day
_____2 Times per week
_____3 Times per month
_____4 Never
*During the past 30 days, how many times per day, week or month did you eat dark green vegetables for example broccoli or dark leafy greens including romaine, chard, collard greens or spinach?
_____1 Times per day
_____2 Times per week
_____3 Times per month
_____4 Never
*During the past 30 days, how many times per day, week or month did you eat orange colored vegetables such as sweet potatoes, pumpkin, winter squash or carrots?
_____1 Times per day
_____2 Times per week
_____3 Times per month
_____4 Never
*Not counting these last questions on fruits and vegetables, during the past 30 days, about how many times per day, week or month did you eat OTHER vegetables? Examples of other vegetables include tomatoes, tomato juice or V-8 juice, corn, eggplant, lettuce, cabbage and white potatoes that are not fried such as baked or mashed potatoes.
_____1 Times per day
_____2 Times per week
_____3 Times per month
_____4 Never
*How many servings of fruits and vegetables do you usually have per day? (1 serving = 1 medium piece of fruit; ½ cup fresh, frozen or canned fruits/vegetables; ¾ cup fruit/vegetable juice; 1 cup salad greens; or ¼ cup dried fruit).
____0 servings per day
____1-2 servings per day
____3-4 servings per day
____5 or more servings per day
The next questions are about alcohol use and smoking.
*During the 30 days, how often did you usually have any kind of drink containing alcohol?
By a drink we mean half an ounce of absolute alcohol (e.g. a 12 ounce can or glass of beer or cooler, a 5 ounce glass of wine, or a drink containing 1 shot of liquor).
_____1 Every
day
_____2 5 to 6 times a week
_____3 3 to 4 times a
week
_____4 twice a week
_____5 once a week
_____6 2
to 3 times a month
_____7 once a month
_____8 I did not
drink any alcohol in the past 30 days, but I did drink in the past
SKIP TO 3.25
_____9 I never drank any alcohol in my life SKIP TO 3.25
During the last 30 days, how many alcoholic drinks did you have on a typical day when you drank alcohol?
_____1 25 or
more drinks
_____2 19 to 24 drinks
_____3 16 to 18
drinks
_____4 12 to 15 drinks
_____5 9 to 11
drinks
_____6 7 to 8 drinks
_____7 5 to 6 drinks
_____8 3
to 4 drinks
_____9 2 drinks
_____10 1 drink
*During the last 30 days, how often did you have 4 or more drinks containing any kind of alcohol in within a two-hour period?
_____1 Every
day
_____2 5 to 6 days a week
_____3 3 to 4 days a
week
_____4 two days a week
_____5 one day a week
_____6 2
to 3 days a month
_____7 one day a month
_____8 Never
*Do you NOW smoke cigarettes every day, some days or not at all?
_____1 Every day
_____2 Some days
_____3 Not at all
*Have you smoked at least 100 cigarettes in your lifetime?
_____1 Yes
_____2 No
_____1 Yes
_____2 No
If yes, how often do you use marijuana?
_____1 Every
day
_____2 5 to 6 days a week
_____3 3 to 4 days a
week
_____4 two days a week
_____5 one day a week
_____6 2
to 3 days a month
_____7 one day a month
IV. Psychosocial Assessments
The next questions ask about what things you may or may not think about when it comes to food and eating. I will give you a card so you can show me which number describes your experiences with each question I read out loud to you. [HAND RESPONSE CARD C].
|
Almost Never |
Some- times |
Fairly Often |
Very Often |
Factor 1: Disinhibition |
||||
|
1 |
2 |
3 |
4 |
|
1 |
2 |
3 |
4 |
|
1 |
2 |
3 |
4 |
|
1 |
2 |
3 |
4 |
|
1 |
2 |
3 |
4 |
|
1 |
2 |
3 |
4 |
|
1 |
2 |
3 |
4 |
|
1 |
2 |
3 |
4 |
Factor 4: Emotional Response |
||||
|
1 |
2 |
3 |
4 |
|
1 |
2 |
3 |
4 |
|
1 |
2 |
3 |
4 |
|
1 |
2 |
3 |
4 |
Factor 5: Distraction |
||||
|
1 |
2 |
3 |
4 |
|
1 |
2 |
3 |
4 |
|
1 |
2 |
3 |
4 |
Below is a collection of statements about your everyday experience. Using the 1-6 scale I have given you on the chart, please indicate how frequently or infrequently you currently have each experience. Please answer according to what really reflects your experience rather than what you think your experience should be. Please treat each item separately from every other item. (SHOW RESPONSE CARD D) [reverse score]
|
Never |
Very Infrequently |
Somewhat Infrequently |
Somewhat Frequently |
Very Frequently |
Almost Always |
|
1 |
2 |
3 |
4 |
5 |
6 |
|
1 |
2 |
3 |
4 |
5 |
6 |
|
1 |
2 |
3 |
4 |
5 |
6 |
|
1 |
2 |
3 |
4 |
5 |
6 |
|
1 |
2 |
3 |
4 |
5 |
6 |
|
1 |
2 |
3 |
4 |
5 |
6 |
|
1 |
2 |
3 |
4 |
5 |
6 |
|
1 |
2 |
3 |
4 |
5 |
6 |
|
1 |
2 |
3 |
4 |
5 |
6 |
|
1 |
2 |
3 |
4 |
5 |
6 |
|
1 |
2 |
3 |
4 |
5 |
6 |
|
1 |
2 |
3 |
4 |
5 |
6 |
|
1 |
2 |
3 |
4 |
5 |
6 |
|
1 |
2 |
3 |
4 |
5 |
6 |
|
1 |
2 |
3 |
4 |
5 |
6 |
The next questions ask you about your feelings and thoughts during the last month. Again, that includes all time from MONTH/YEAR until today. In each case, you will be asked to say how often you felt or thought a certain way. You can answer by choosing one of these responses from “Never” to “Very Often” [SHOW RESPONSE CARD E].
|
Never |
Almost Never |
Sometimes |
Fairly Often |
Very Often |
|
0 |
1 |
2 |
3 |
4 |
|
0 |
1 |
2 |
3 |
4 |
|
0 |
1 |
2 |
3 |
4 |
|
0 |
1 |
2 |
3 |
4 |
|
0 |
1 |
2 |
3 |
4 |
|
0 |
1 |
2 |
3 |
4 |
|
0 |
1 |
2 |
3 |
4 |
|
0 |
1 |
2 |
3 |
4 |
|
0 |
1 |
2 |
3 |
4 |
|
0 |
1 |
2 |
3 |
4 |
Section V. Partners and Social Support
* Which of the following best describes your present relationship?
_____1 In a committed relationship with a woman (for example, cohabitating, domestic partnership, or legally married)
_____2 In a committed relationship with a man (for example, cohabitating, domestic partnership or legally married)
_____3 Single, but somewhat involved with a woman, man or both – SKIP TO 5.2
_____4 Single, and not involved with anyone – SKIP to 5.2
5. IA If in a committed relationship, do you currently live with your partner:
_____1 All or most of the time
_____2 Some of the time
_____3 None of the time
In this last section I will ask you about your connections with friends, any partner you might have and the community.
How satisfied are you with your current relationship status?
Very satisfied
Somewhat satisfied
Somewhat dissatisfied
Very dissatisfied
How would you rate the health of your current partner?
Excellent
Very good
Good
Fair
Poor
No partner (or N/A)
*What is the number that best depicts the approximate outline of your primary partner?
RECORD RESPONSE: _____ _____ [NO PARTNER=7]
How satisfied are you with the support you receive from your current social network of friends?
Very satisfied
Somewhat satisfied
Not satisfied nor unsatisfied
Somewhat dissatisfied
Very dissatisfied
Is your current social network
Mostly other lesbian and bisexual women
A mix of LGBT people
A mix of women, LB and straight
A mix of heterosexual men and women and LGBT people
Mostly heterosexual people
Social Isolation: Family |
|
*5.7 How many relatives do you see or hear from at least once a month? |
0 = none |
*5.8 How many relatives do you feel at ease with that you can talk about private matters? |
0 = none |
*5.9 How many relatives do you feel close to such that you could call on them for help? |
0 = none |
Social Isolation: Friendships |
|
*5.10 How many of your friends do you see or hear from at least once a month? |
0 = none |
*5.11 How many friends do you feel at ease with that you can talk about private matters? |
0 = none |
*5.12 How many friends do you feel close to such that you could call on them for help? |
0 = none |
VI. Health Assessment
Read introduction: These questions are basic health questions. It will include me taking down your height, weight and measuring your waist circumference with a measuring tape. Is it okay for me to measure your waist? A clinic staff member will take your blood pressure as well.
6.1. What is your current height? ________ ft _______inches
6.2. Record current weight ________ pounds
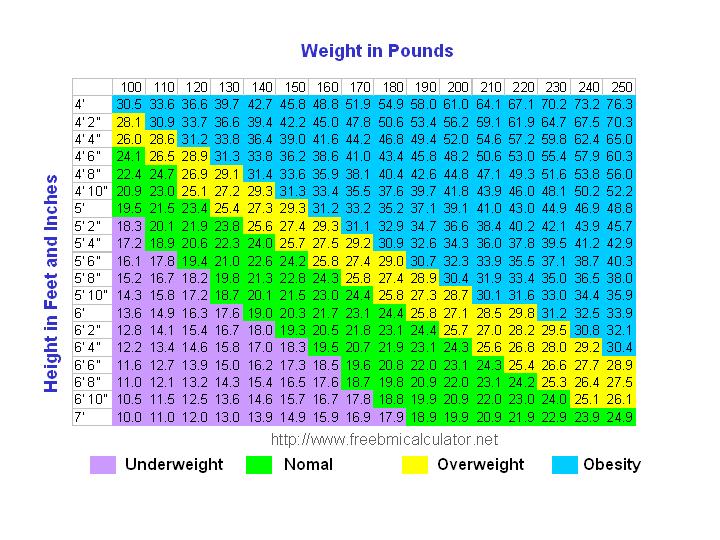
6.3. BMI = __________________ (filled in by staff)
6.4. Waist circumference _____________ inches
6.5. Blood pressure ______________
6.6. Have you had at least one menstrual period in the past 12 months? (Please do not include bleedings caused by medical conditions, hormone therapy, or surgeries).
_____1 Yes
_____2 No SKIP TO 6.6C
6.6A. Is your period:
_____1 Regular (approximately once a month)
_____2 Irregular
6.2B Why do you think your period is irregular? _____________________________
SKIP TO 6.7.
6.6C How long has it been since your last period? ____________ months (calculate years into months)
6.6D. What are you doing to manage your menopause symptoms?
Hormone treatment
Nutritional treatment
Herbal treatment
Other prescription medications
Meditation
Other ________________
6.7. Do you currently have or have you ever had any of the following health concerns or chronic conditions?
Heart attack
Stroke
High blood pressure
High cholesterol (hyperlipidemia, high triglycerides)
Asthma
Emphysema, COPD, chronic bronchitis or other lung disease
Prediabetes
Diabetes
Arthritis
Chronic pain
Lab Testing
Total cholesterol _________
LDL ___________
HDL __________
Triglycerides ___________
Hemoglobin A1C ______________
Note: Core questions across study sites are indicated with an * at their start.
According to the Paperwork Reduction Act of 1995, no persons are required to respond to a collection of information unless it displays a valid OMB control number. The valid OMB control number for this information collection is 0990-xxxx . The time required to complete this information collection is estimated to average 4 minutes per response, including the time to review instructions, search existing data resources, gather the data needed, and complete and review the information collection. If you have comments concerning the accuracy of the time estimate(s) or suggestions for improving this form, please write to: U.S. Department of Health & Human Services, OS/OCIO/PRA, 200 Independence Ave., S.W., Suite 336-E, Washington D.C. 20201, Attention: PRA Reports Clearance Officer
| File Type | application/vnd.openxmlformats-officedocument.wordprocessingml.document |
| Author | Natalie Ingraham |
| File Modified | 0000-00-00 |
| File Created | 2021-01-28 |
© 2026 OMB.report | Privacy Policy