Download:
docx |
pdf
Form
Approved
OMB
No. 0990-
Exp.
Date XX/XX/20XX
Office
on Women’s Health (OWH)
Living Healthier, Living Longer
DEMOGRAPHICS/BACKGROUND
|
Are
you of Hispanic or Latino origin?
|
|
|
Which
category most closely describes your race? (check all that
apply)
|
Black
or African American
Asian
White
American
Indian or Alaska Native
Native
Hawaiian or Other Pacific Islander
|
What
is your current employment status? (check all that apply)
|
Working
part-time
Working
full-time
Unemployed,
laid off, on strike
Retired
Disabled
or unable to work
Student
Full-time
homemaker
|
What
is the highest level of education you have completed?
|
Less
than high school
High
school or GED
Technical
school -- no degree
Some
college -- no degree
2-year
college degree/technical school degree
4-year
college degree
Post-graduate work
or degree
|
What
gender were you assigned at birth?
|
|
|
Which
of the following best represents how you think of yourself?
|
Lesbian
or gay (skip
to question 8)
Straight,
that is, not lesbian or gay (skip
to question 8)
Bisexual
(skip
to question 8)
Something
else
I don't know the
answer (skip
to question 8)
|
What
do you mean by something else?
|
You
are not straight, but identify with another label such as queer,
trisexual, omnisexual or pansexual
You
are transgender, transsexual or gender variant
You
have not figured out or are in the process of figuring out your
sexuality
You
do not think of yourself as having sexuality
You
do not use labels to identify yourself
You mean something
else
|
How
“out” are you about your sexuality with your health
care providers (doctors, nurses, nutritionists, mental health
professionals, personal trainers, etc.)
|
Out
to all
Out
to some
Out
to a few
Out
to None
N/A
|
Which
of the following best describes your present relationship?
|
In
a committed relationship with a women (for example, cohabiting,
domestic partnership, legally married)
In
a committed relationship with a man (for example, cohabiting,
domestic partnership, legally married)
Single,
but somewhat involved with a woman, man, or both (skip
to question 12)
Single, and not
involved with anyone (skip
to question 12)
|
Do
you currently live with your partner:
|
|
|
All
or most of the time
Some
of the time
None
of the time
|
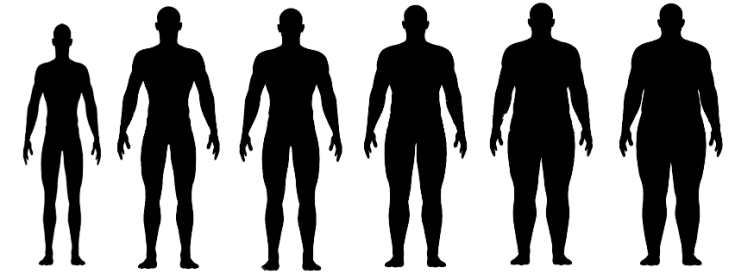
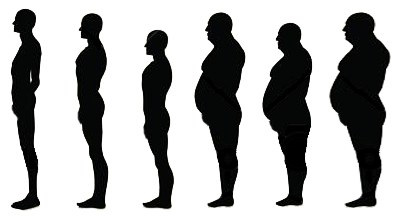
Select
the picture group that best depicts the approximate outline of
your partner:
|
In a relationship
with a women
|
In a relationship
with a man
|
|
|

|

|
|
|
|
|
|

|

|
|
|
|
|
|

|

|
|
|
|
|
|

|

|
|
|
|
|
|

|

|
|
|
|
|
|

|

|
|
|
|
SOCIAL NETWORK
|
For
questions 12-14, include the people to whom you are related by
birth, marriage, adoption, etc.
|
How
many relatives
do you see or hear from at least once a month?
|
None
One
Two
Three
or four
Five
thru eight
Nine or more
|
How
many relatives
do you feel at ease with that you can talk about private
matters?
|
None
One
Two
Three
or four
Five
thru eight
Nine or more
|
How
many relatives
do you feel close to such that you could call on them for help?
|
None
One
Two
Three
or four
Five
thru eight
Nine or more
|
For
questions 15-17, include all of your friends, including those who
live in your neighborhood
|
How
many of your friends
do you see or hear from at least once a month?
|
None
One
Two
Three
or four
Five
thru eight
Nine or more
|
How
many friends
do you feel at ease with that you can talk about private
matters?
|
None
One
Two
Three
or four
Five
thru eight
Nine or more
|
How
many friends
do you feel close to such that you could call on them for help?
|
None
One
Two
Three
or four
Five
thru eight
Nine or more
|
GENERAL HEALTH
|
In
general, would you say your health is:
|
Excellent
Very
good
Good
Fair
Poor
|
The
following questions are about activities you might do during a
typical day. Does your health now limit you in these activities?
If so, how much?
|
Moderate
activities, such as moving a table, pushing a vacuum cleaner,
bowling or playing golf?
|
Yes,
limited a lot
Yes,
limited a little
No, not limited at
all
|
Climbing
several flights of stairs?
|
Yes,
limited a lot
Yes,
limited a little
No, not limited at
all
|
During
the past 4 weeks, have you had any of the following problems
with your work or other regular daily activities as a result of
your physical
health?
|
Accomplished
less than you would like.
|
|
Were
limited in the kind of work or other activities.
|
|
During
the past 4 weeks, have you had any of the following problems
with your work or other regular daily activities as a result of
any emotional
problems
(such as feeling depressed or anxious)?
|
Accomplished
less than you would like.
|
|
Didn’t
do work or other activities as carefully as usual.
|
|
During
the past 4 weeks, how much did pain interfere with your normal
work (including both work outside the home and housework)?
|
Not
at all
A
little bit
Moderately
Quite
a bit
Extremely
|
These
questions are about how you feel and how things have been with
you during the past 4 weeks. For each question, please give the
one answer that comes closest to the way you have been feeling.
|
Have
you felt calm and peaceful?
|
All
of the time
Most
of the time
A
good bit of the time
Some
of the time
A
little of the time
None of the time
|
Did
you have a lot of energy?
|
All
of the time
Most
of the time
A
good bit of the time
Some
of the time
A
little of the time
None of the time
|
Have
you felt downhearted and blue?
|
All
of the time
Most
of the time
A
good bit of the time
Some
of the time
A
little of the time
None of the time
|
During
the past 4 weeks, how much of the time has your physical health
or emotional problems interfered with your social activities
(like visiting with friends, relatives, etc.)?
|
All
of the time
Most
of the time
A
good bit of the time
Some
of the time
A
little of the time
None of the time
|
Now,
we’d like to ask you some questions about how your health
may have changed.
|
Compared
to one year ago, how would you rate your physical
health in
general now?
|
Much
better
Slightly
better
About
the same
Slightly
worse
Much worse
|
Compared
to one year ago, how would you rate your emotional
problems (such
as feeling anxious, depressed or irritable) now?
|
Much
better
Slightly
better
About
the same
Slightly
worse
Much worse
|
NUTRITION AND
CONSUMPTION
|
FRUITS AND VEGETABLES
|
The
next section is about the foods you consumed during the past
month
(i.e., the past 30 days), including meals and snacks.
|
During
the past
month,
how many times per day, week or month did you drink 100% PURE
fruit juices? Do
not include fruit-flavored drinks with added sugar or fruit
juice you made at home and added sugar to. Only include 100%
juice.
|
_____ times per:
|
Day
Week
Month
Never
Don’t know
|
During
the past
month,
not counting juice, how many times per day, week or month did
you eat FRUIT?
Count
fresh, frozen or canned fruit. Include apples, bananas,
applesauce, oranges, grape fruit, fruit salad, watermelon,
cantaloupe or musk melon, papaya, lychees, star fruit,
pomegranates, mangos, grapes, and berries such as blueberries
and strawberries.
|
_____ times per:
|
Day
Week
Month
Never
Don’t know
|
During
the past
month,
how many times per day, week, or month did you eat COOKED
or CANNED BEANS,
such as refried, baked, black, garbanzo beans, beans in soup,
soybeans, edamame, tofu or lentils. Do
NOT include long green beans.
|
_____ times per:
|
Day
Week
Month
Never
Don’t know
|
During
the past
month,
how many times per day, week or month did you eat DARK
GREEN VEGETABLES
for example broccoli or dark leafy greens including romaine,
chard, collard greens or spinach?
|
_____ times per:
|
Day
Week
Month
Never
Don’t know
|
During
the past
month,
how many times per day, week or month did you eat ORANGE
COLORED VEGETABLES
such as sweet potatoes, pumpkin, winter squash or carrots?
Winter
squash have hard, thick skins and deep yellow to orange flesh.
They include acorn, buttercup, and spaghetti squash.
|
_____ times per:
|
Day
Week
Month
Never
Don’t know
|
Not
counting questions 29-33, during the past
month,
about how many times per day, week or month did you eat OTHER
vegetables? Examples
of other vegetables include tomatoes, tomato juice or V-8 juice,
corn, eggplant, peas, lettuce, cabbage and white potatoes that
are not fried such as baked or mashed potatoes.
|
_____ times per:
|
Day
Week
Month
Never
Don’t know
|
How many servings of
fruits and vegetables do you usually have per day?
(1
serving = 1 medium piece of fruit; ½ cup fresh, frozen or
canned fruits/vegetables; ¾ cup fruit/vegetable juice; 1
cup salad greens; or ¼ cup dried fruit)
|
|
|
BEVERAGES
|
The
next section is about the beverages you drank during the past
month (i.e., the past 30 days). Remember
to include any sweetened beverages used as a mixer.
|
During
the past month, how often did you drink regular soda or pop that
contains sugar? Do not include diet soda.
|
_____ times per:
|
|
Each
time you drank soda or pop, how much did you usually drink?
|
|
|
During
the past month, how often did you drink sports or energy drinks
such as Gatorade, Red Bull and Vitamin Water? Do not include
diet or sugar-free kinds.
|
_____ times per:
|
|
Each
time you drank sports or energy drinks, how much did you usually
drink?
|
|
|
During
the past month, how often did you drink sweetened fruit drinks
such as Kool-aid, cranberry drink and lemonade? Include fruit
drinks you made at home and added sugar to. Do not include 100%
fruit juices and drinks with things like Splenda or Equal.
|
_____ times per:
|
|
Each
time you drank sweetened fruit drinks, how much did you usually
drink?
|
|
|
During
the past month, how often did you drink coffee or tea with sugar
or honey added? Do not include drinks with things like Splenda
or Equal. Include pre-sweetened tea and coffee drinks such as
Arizona Iced Tea and Frappuccino.
|
_____ times per:
|
|
Each
time you drank sweetened tea or coffee, how much did you usually
drink?
|
|
|
In
the past month, how often did you drink water (including tap,
bottled, and carbonated water)?
|
_____ times per:
|
|
Each
time you drank water, how much did you usually drink?
|
|
|
For
alcohol, a drink is equal to half an ounce of absolute alcohol
(e.g. a 12 ounce can or glass of beer or cooler, a 5 ounce glass
of wine, or a drink containing 1 shot of liquor).
|
During
the last 30 days, how often did you usually have any kind of
drink containing alcohol? Choose only one.
|
Every
day
5
to 6 times a week
3
to 4 times a week
twice
a week
once
a week
2
to 3 times a month
once
a month
I
did not drink any alcohol in the past month, but I did drink in
the past (done
with survey)
I never drank any
alcohol in my life (done
with survey)
|
During
the last 30 days, how many alcoholic drinks did you have on a
typical day when you drank alcohol?
|
25
or more drinks
19
to 24 drinks
16
to 18 drinks
12
to 15 drinks
9
to 11 drinks
7
to 8 drinks
5
to 6 drinks
3
to 4 drinks
2
drinks
1 drink
|
During
the last 30 days, how often did you have 4 or more drinks
containing any kind of alcohol in within a two-hour period?
Choose only one.
|
Every
day
5
to 6 days a week
3
to 4 days a week
two
days a week
one
day a week
2
to 3 days a month
one day a month
|
End
of Questionnaire
According
to the Paperwork Reduction Act of 1995, no persons are required to
respond to a collection of information unless it displays a valid
OMB control number. The valid OMB control number for this
information collection is 0990-xxxx . The time required to complete
this information collection is estimated to average 4 minutes per
response, including the time to review instructions, search existing
data resources, gather the data needed, and complete and review the
information collection. If you have comments concerning the accuracy
of the time estimate(s) or suggestions for improving this form,
please write to: U.S. Department of Health & Human Services,
OS/OCIO/PRA, 200 Independence Ave., S.W., Suite 336-E, Washington
D.C. 20201, Attention: PRA Reports Clearance Officer
| File Type | application/vnd.openxmlformats-officedocument.wordprocessingml.document |
| Author | Rizer, Allison |
| File Modified | 0000-00-00 |
| File Created | 2021-01-28 |