Tracking Survey
Tracking of Participants in the Early Head Start Research and Evaluation Project
ATTACHMENT D Tracking Survey Internet Version REV
Tracking Survey
OMB: 0970-0388
T
OMB# 0970-0388
Expires: 10/1/2015
Numbering will be made consecutive and font as well as formatting will be made consistent during programming
This collection of information
is voluntary and will be used to maintain up-to-date contact
information on the participants of the Early Head Start Research and
Evaluation Project. Public reporting burden for this collection of
information is estimated to average 15 minutes per response,
including the time for reviewing instructions, gathering and
maintaining the data needed, and reviewing the collection of
information. An agency may not conduct or sponsor, and a person is
not required to respond to, a collection of information unless it
displays a currently valid OMB control number. The OMB number for
this information collection is 0970-0388 (Exp. 10/1/15). Send
comments regarding this burden estimate or any other aspect of this
collection of information, including suggestions for reducing this
burden to: Amy Madigan; ACF / OPRE, 370 L’Enfant Promenade SW,
7th floor West, Washington, DC 20447; Attn: OMB-PRA (0970-0388).
Please
remember that all the information you provide will be shared ONLY
with researchers working on the Early Head Start Follow-up Study
and kept private to the extent permitted by law.
1. We
have your name as (FILL PRIMARYCAREGIVER NAME). Is this correct?
*Q asked if Q1=NO
What
is your correct name?
2. We
have your child’s name as (FILL CHILD NAME). Is this correct?
*Q asked if Q2=NO
What
is your child’s correct name?
3. Are
you still (CHILD NAME)’s primary caregiver?
* If NO, Respondent will be skipped to the “New Primary Caregiver” section of the survey
*Q asked if Q5=NO
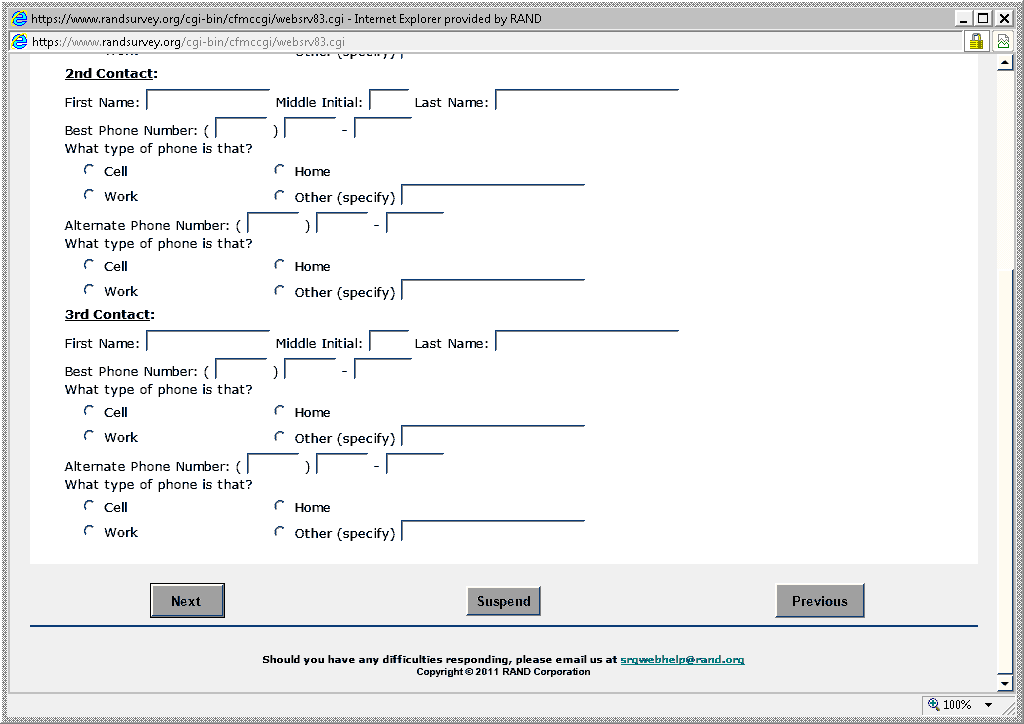
6. What
is the best phone number to reach you on?
10. Do
you have any plans to move in the next year?
*Q asked if Q10=YES


Bottom half of above screen:
After
your child turns 18, we would like to follow up with him or her
directly. If your child is contacted in the future for the study,
they can decide at that time whether or not to take part.
What
is your child’s email address?
Click
this box if they do not have email.
What
is your child’s cell phone number?
Click
this box if they do not have a Cell Phone
Please
list any other ways to reach your child directly?
15.
Thinking ahead to when your child is 18, where do you think your
child will be living? 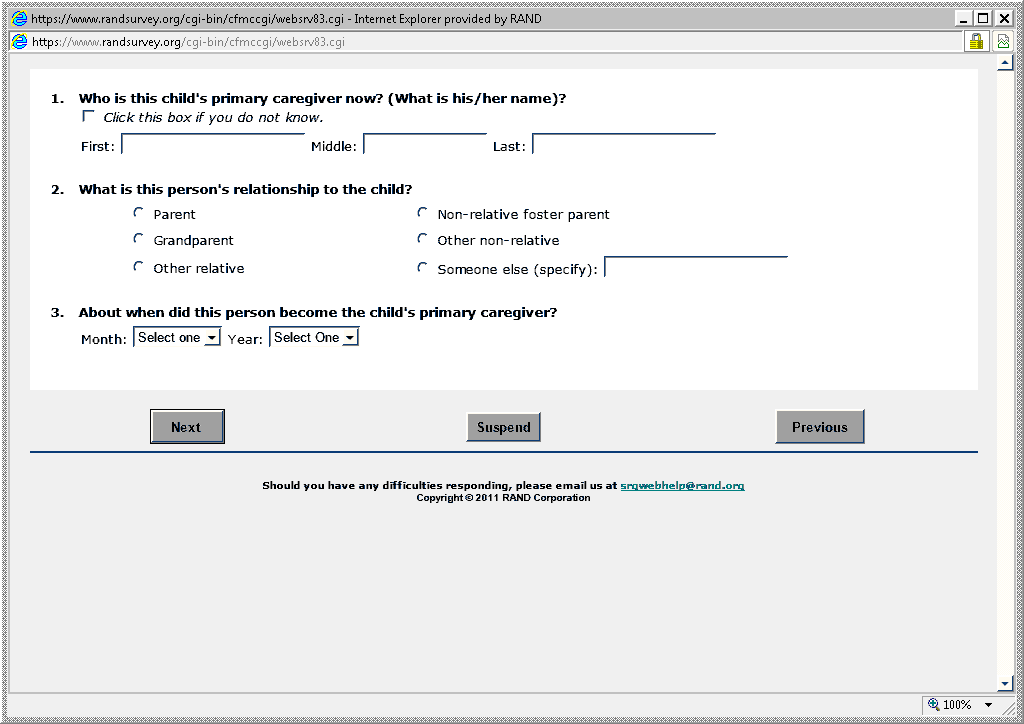
![]() With
you
With
you![]() With
another family member
With
another family member![]() On
his/her own or with roommates
On
his/her own or with roommates![]() In
a college dorm
In
a college dorm![]() In
the military
In
the military![]() Somewhere
else (specify)
Somewhere
else (specify)
![]()
Now
we’d like to ask you a few questions about how your child is
doing.
16.
Will (or did) your child graduate high school or get a GED before
Fall 2013?
Yes,
Graduated high school Yes,
GED No
*Q asked if Q16=YES
17.
If Yes, will (or does) your child go to college?
![]() Yes
Yes![]() No
No
18.
What school will your child attend in Fall 2013?
Click
this box if the child will not be in school.
School:
City:
19.
What grade will your child be in Fall 2013?
Grade:
![]()
![]()
![]()
20.
What do you think are the chances your child will graduate from
college?
![]() No
chance
No
chance![]() Some
chance
Some
chance![]() About
50/50
About
50/50![]() Pretty
likely
Pretty
likely![]() It
will happen
It
will happen
21.
What do you think are the chances your child will have a good job by
age 30?
![]() No
chance
No
chance![]() Some
chance
Some
chance![]() About
50/50
About
50/50![]() Pretty
likely
Pretty
likely![]() It
will happen
It
will happen
22.
Has your child ever had any contact with the juvenile justice
system? This would include:
being
picked up by the police for breaking the law,
being
found guilty for a crime or a delinquent offense,
being
on probation or court supervision,
being
held at juvenile hall or in jail
![]() Yes
Yes![]() No
No![]() Don’t
Know
Don’t
Know
23.
Overall, would you describe your child’s health as…
![]() Excellent
Excellent![]() Very
good
Very
good![]() Good
Good![]() Fair
Fair![]() Poor?
Poor?
Now
a few questions about you.
24.
What is the highest grade or year of school that you have completed?
![]() Less
than high school
Less
than high school![]() High
school or GED
High
school or GED![]() Vocational
school or 2 year Associate’s Degree
Vocational
school or 2 year Associate’s Degree![]() College
or graduate school
College
or graduate school
25.
Which of the following best describes your present work or school
situation?
![]() Working
full-time (35 hours a week or more)
Working
full-time (35 hours a week or more)![]() Working
part-time (less than 35 hours per week)
Working
part-time (less than 35 hours per week)![]() Unemployed
and looking for work
Unemployed
and looking for work![]() Unemployed
and not looking for work
Unemployed
and not looking for work![]() Full-time
homemaker
Full-time
homemaker![]() In
school
In
school![]() Too
disabled to work
Too
disabled to work![]() Some
other situation (specify)
Some
other situation (specify)![]()
26.
These questions are about how you feel and how things have been with
you during the past 4 weeks. For each question, please give the one
answer that comes closest to the way you have been feeling. How
much of the time during the past 4 weeks...
Have
you felt calm and peaceful?
Did
you have a lot of energy?
Have
you felt downhearted
and blue?
![]() All
of the time
All
of the time
![]() Most
of the time
Most
of the time
![]() A
good bit of the time
A
good bit of the time
![]() Some
of the time
Some
of the time
![]() A
little of the time
A
little of the time
![]() None
of the time
None
of the time
![]() All
of the time
All
of the time
![]() Most
of the time
Most
of the time
![]() A
good bit of the time
A
good bit of the time
![]() Some
of the time
Some
of the time
![]() A
little of the time
A
little of the time
![]() None
of the time
None
of the time
![]() All
of the time
All
of the time
![]() Most
of the time
Most
of the time
![]() A
good bit of the time
A
good bit of the time
![]() Some
of the time
Some
of the time
![]() A
little of the time
A
little of the time
![]() None
of the time
None
of the time
* IF R is not current primary caregiver (Q3=NO)
| File Type | application/msword |
| Author | RAND Authorized User |
| Last Modified By | DHHS |
| File Modified | 2013-06-04 |
| File Created | 2013-05-29 |
© 2026 OMB.report | Privacy Policy