3-GreatLakes_SSB_20120712
3-GreatLakes_SSB_20120712.doc
Biomonitoring of Great Lakes Populations Program
OMB: 0923-0044
Supporting Statement
For OMB Review and Approval of
Agency for Toxic Substances and Disease Registry (ATSDR)
Biomonitoring of Great Lakes Populations Program
PART B. Collections of Information Employing Statistical Methods
Date: July 12, 2012
Steve Dearwent, Ph.D.
ATSDR Division of Toxicology and Human Health Sciences
Program Official
Phone: 770-488-3665
Email: SDearwent@cdc.gov
Fax Number: 770-488-7187
TABLE OF CONTENTS
B. COLLECTIONS OF INFORMATION EMPLOYING STATISTICAL METHODS
Overview …………………………………………….…………………………………2
B.1. Respondent Universe and Sampling Methods …………………………………………...3
B.2. Procedures for the Collection of Information………………………………………….…11
B.3. Methods to Maximize Response Rates and Deal with No Response…………………….24
B.4. Tests of Procedures or Methods to be Undertaken…………………………………….…27
B.5. Individuals Consulted on Statistical Aspects and Individuals Collecting and/or
Analyzing Data ………………………………………………………………………………. 27
References
….…………………………………………………………………………………38
B. COLLECTIONS OF INFORMATION EMPLOYING STATISTICAL METHODS
Overview
In 2009, the federal Great Lakes Restoration Initiative (GLRI) was established under the stewardship of the U.S. Environmental Protection Agency (US EPA) to protect, restore, and maintain the Great Lakes ecosystem in partnership with 15 other federal agencies. The task force of federal agencies developed the GLRI Action Plan which covers fiscal years 2010 to 2014. In the first three years the U.S. EPA has received over a billion dollars through U.S. President Barack Obama’s administration to make substantial progress towards restoring the Great Lakes to ecological health. Under an interagency agreement with the US EPA, the Agency for Toxic Substances and Disease Registry (ATSDR) established the Great Lakes Biomonitoring Program under its 1980 Comprehensive Environmental Response Compensation and Liability Act (CERCLA) authority. The ATSDR Great Lakes Biomonitoring Program aims to provide a human exposure assessment to Great Lakes contaminants among targeted subpopulations concurrent with the onset of restoration activities.
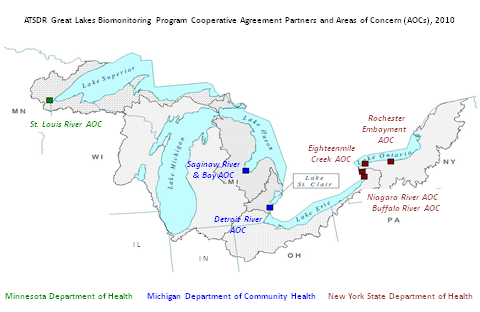
The Agency for Toxic Substances and Disease Registry (ATSDR) announced a funding opportunity called the “Biomonitoring of Great Lakes Populations Program” (CDC-RFA-TS10-1001). From the applicants for this cooperative agreement, ATSDR awarded funds to the Michigan Department of Community Health (MDCH), the Minnesota Department of Health (MDH), and the New York State Department of Health (NYS DOH) to conduct non-research studies of human exposures and to advance jurisdiction-specific public health actions. This public health effort focuses on vulnerable or susceptible subpopulations with the potential for increased risk of exposure to persistent contaminants common to the Great Lakes watersheds and ecosystems (Figure 1).
An overview/diagram of the information collection process for each state program can be found in Attachment 4 (MDCH), Attachment 5 (MDH), and Attachment 6 (NYS DOH).
Figure 1.
An overview/diagram of the information collection process for each state program can be found in Attachment 4 (MDCH), Attachment 5 (MDH), and Attachment 6 (NYS DOH).
B.1. Respondent Universe and Sampling Methods
Table 1. Respondent universe and number of respondents by study area
Michigan shoreline anglers |
Respondent Universe/Respondents |
Response Rate |
Venue-based Secondary Enumeration |
4000 |
|
Number of Eligible Respondents |
1440 |
36% |
Sampling Frame: Eligible Respondents Willing to Participate |
936 |
65% |
Number Randomly Selected to Participate |
500 |
|
Study Participants |
400 |
80%* |
Minnesota American Indians |
|
|
Sampling frame |
4000 |
|
Number Randomly Selected from Frame |
793 |
|
Number of Eligible |
714 |
|
Study Participants |
500 |
70% |
New York state licensed anglers |
|
|
Mail Screening Survey |
14,400 |
|
Screening response |
4,320 |
|
Number of Eligible Respondents |
864 |
|
Study Participants |
400 |
46%** |
NYS Refugees and Immigrants from Burma |
|
|
Screening response |
184 |
|
Number of Eligible Respondents |
124 |
|
Study Participants |
100 |
81% |
*Participation percentage of randomly selected persons eligible per venue-based screening interview who also indicated their willingness to participate
**Participation percentage of randomly selected persons eligible per response to mail screening survey
The response rates for each target population presented in the above table reflect multiple stage sampling processes. Several response stages occur along the path to the clinic screening of study participants and collection of biological specimens. Although final response rates may seem dubiously high, the denominators only include eligible participants based on previous responses; and, for Michigan also a known willingness to participate. A more detailed description of response rates for each program is presented below.
Michigan:
Response rates
The 80% participation rate for the Michigan Department of Community Health (MDCH) program is based on a sampling frame of shoreline anglers who met the study eligibility criteria per a screening interview at shoreline venues and said that were willing to participate in the study.
The response, sampling process begins with a venue-based enumeration phase. People fishing at selected venues will be asked to answer screening questions about eating local-caught fish, their age, gender, and race/ethnicity; and at the end of the screening questions, their interest in participating in the study. The MDCH program estimates that 36% of persons screened at shoreline venues will be eligible to participate. This estimate is based on responses to a fish consumption survey conducted by MDCH in June 2007 (MDCH, 2007). According to the 2007 report, out of a total of 585 responses, 208 reported that they consume 2 or more meals per month. The MDCH program estimates screening about 2,000 people in each the Saginaw Bay area and the Detroit River area to establish a sufficient sampling frame. Of the eligible responders, MDCH estimates that 65% will indicate a willingness to participate in the program if selected. Nonresponse bias will be assessed by comparing eligible people who indicate a willingness to participate in the full study (n~936) to those who decline further participation (n~504) using the information gathered during venue-based screening.
A sampling frame will be constructed of people who meet the eligibility criteria and have indicated an interest to participate in the study. Study participants will be randomly selected from the sampling frame with a target sample size of 200 people from the Detroit River area and 200 people from the Saginaw River/Bay area. The program estimates that 100 people (50 per area) who are randomly selected and contacted to schedule a clinic appointment will not be successfully recruited (either ineligible based on the phone interview, no contact or decline). A second stage of nonresponse bias will be assessed using the information gathered during the venue-based screening.
Sampling method
Shoreline anglers are defined as urban Michigan residents who fish along shoreline venues on the Detroit River and Saginaw Bay Areas of Concern (AOCs). Because no sampling frame exists for this population, MDCH will use Venue Based Sampling (VBS), also known as time-location sampling. VBS is a probability-based strategy for recruiting members of a target population assembling at discrete locations during specific units of time. (Mackellar, et al. 1996) VBS proceeds through three phases: the formative phase; the preparatory or primary enumeration phase, and the sampling or secondary enumeration phase.
Primary enumeration was conducted during the spring of 2011 to provide visual estimates of the density of these shoreline anglers on certain days of the week and at specific times of the day at identified fishing venues. During this phase a clicker was used to make headcounts of persons congregating in venue-day-time units who appear to fit the inclusion criteria of the target group. Data were collected along the Detroit River for 35 days, and along the Lower Tittabawassee and Saginaw Rivers for 21 days. The venue-day-time units were randomized using a random number generator and were clustered geographically to make traveling from one venue to the next feasible. Findings will be used to establish a calendar of the times and places where data collection for the next phase of the study will occur. The benefit of a venue based sampling approach is that it provides an analytically rigorous alternative to traditional probability sampling while avoiding the limitations of non-probability (convenience) sampling (Levy & Lemeshow, 1991). The primary enumeration phase will need to be repeated or verified based on the timeline for program start-up; in mid/late summer 2012 or spring/early summer 2013 pending OMB approval.
During the secondary enumeration phase, people fishing at selected venues will be asked to answer questions about eating local-caught fish, their age, gender, race/ethnicity, and interest in participating in the study (Attachment 4a). Participation in this project will be limited to adults 18 years of age and older who eat at least two meals per month of local-caught fish from the Detroit River or Saginaw River/Bay AOCs. Children will not be included in the study because of the large volume of blood needed for the proposed analyses.
For each AOC, the sampling frame will consist of people who meet the eligibility criteria and have indicated an interest to participate in the study. Study participants will be randomly selected from the sampling frame with a target sample size of 200 people from the Detroit River AOC and 200 people from the Saginaw River/Bay AOC. People who are randomly selected will be telephoned to schedule an appointment for study participation. During the telephone call people will be asked questions to determine if they are pregnant, lactating or have a medical conditions (e.g., hemophilia, recent chemotherapy, anemia) that precludes them from safely donating an 83 ml blood sample; and if yes, will also be excluded (Attachment 4b).
Response rate
A 70% response rate is projected for the Minnesota Department of Health (MDH) program based on the response rates for similar programs that targeted tribal communities in the Great Lakes region. A 1994 ATSDR study to assess methylmercury exposure among members of the Fond Du Lac Band of Chippewa Indians in Northern Minnesota reported an 82% response rate (ATSDR 1994). However, response rates have declined over the past few decades for many epidemiologic studys (Galea and Tracy, 2007). The 2010-2011 First Nations Biomonitoring Initiative pilot study had a response rate of 70% (La Corte and Wutte, 2011). Furthermore, the national participation rate for the 2010 Census mailing was 74%; Minnesota was 81%, and Fond du Lac was 76%. Recent response rates and MDH recruitment efforts described in section B.3 support a relatively high response rate for the Fond du Lac community.
Sampling method
The MDH sampling frame will consist of American Indians who are enrolled and receive a variety of health services and social services from the Fond du Lac (FDL) Human Services Division in Carlton County and the southern half of St. Louis County Minnesota. American Indians enrolled with U.S. federally recognized tribes and children or grandchildren of FDL enrollees are eligible to receive a variety of health and social services from the FDL Human Services Division (HSD). Because these services are widely used by the FDL Community, the FDL-HSD “Client List” will be used as the sampling frame. The Client List is the most complete and accurate enumeration of FDL Community members. Eligible participants must be: 18 years or older; living in the study area for at least 12 consecutive months prior to study enrollment; not pregnant; and, willing and medically able to donate blood and urine specimens.
Alternative methods to obtain a representative sample of eligible participants are flawed or unfeasible. The existing FDL “tribal roster” is outdated, does not include descendants of enrolled members and is not location-specific. Selecting a random sample of households in the study area would be both costly and inefficient because only a small proportion of households would include eligible individuals from the target population.
The Client List will be reviewed and “cleaned” prior to selecting potential participants. The “cleaning” will entail the following: 1) ensure a residential address in the study area; 2) ensure that there is only one record per individual; 3) include only persons aged at least 18 years old; 4) remove non-Indians; and 5) remove any persons known by FDL study staff to have died or moved outside the study area. The reasons for removal will be documented. A random number generator will be used to assign a unique number to each person. These random numbers will be ordered numerically to represent the order in which potential participants will be contacted for recruitment and enrollment efforts. Eligible participants must have lived within the defined study area continuously during the past year (except for vacations or absences that total less than 1 month). Based on recommendations from the Tribal Advice Council women who are pregnant will be excluded; it is culturally inappropriate to take blood from an expectant woman when it is not necessary. The overall target number of participants is 500.
FDL-HSD personnel and the FDL Biomonitoring Advice Council have stipulated that at least 60% of the people who participate in the study be affiliated with the FDL Band. Although this proportion of FDL affiliates is slightly higher than anticipated in the sampling frame, it serves a dual purpose. It ensures a sufficient number of affiliates to allow FDL to use study results to conduct its own evaluation of FDL-specific practices and programs; and at the same time, mitigates concerns related to community stigma associated with biomonitoring results from any one particular tribe. Post-sampling weighting will be applied during the data analysis phase to restore the correct proportion of non-FDL tribal members in the sampling frame. Biomonitoring results will not be broken out by tribal affiliation in summary reports.
An FDL Advice Council has been closely engaged in all aspects of program planning and implementation. MDH has contracted with the FDL-HSD to implement the program. Recruitment will be done by members of the FDL community. The Recruiter will attempt to contact each person by phone. If the person is not interested in participating, the Recruiter will document the reason for refusal, and administer the Refusal Questions Form (Attachment 5b) for nonresponse analysis. If the person is undecided, the Recruiter will attempt to answer questions or address concerns about the study. After 10 unsuccessful attempts (different times of day and different days of week) to contact a potential participant, the Recruiter will ask FDL Public Health Nursing staff if they have further information or advice to help locate the individual. If necessary or advised, the Recruiter may attempt to locate the individual in person by visiting the most current address listed or as otherwise suggested by FDL Public Health Nursing Community Health Representatives. If he/she is located, study staff will try to speak with the person face-to-face to identify a phone number or other mechanism to recontact the person to assess willingness to participate. Information regarding age, gender and tribal affiliation will be used to compare characteristics of non-participants and participants, as this may be a source of refusal/nonresponse bias. A data system to track each potential participant through the recruitment process will be maintained by the FDL-HSD.
New York State:
The New York State Department of Health (NYS DOH) has two respondent populations: (1) licensed anglers who live in proximity to the AOCs in western New York who fish in the AOCs and eat their catch (“licensed anglers”); (2) Burmese refugees and immigrants and their descendants who live in the City of Buffalo and eat fish caught in the AOCs. The Buffalo River, Niagara River, and Eighteenmile Creek AOCs are in Erie and Niagara Counties, and the Rochester Embayment AOC is in Monroe County. The catchment area for the licensed anglers will be the ZIP Codes within a 10-mile buffer of the AOCs). The catchment area for the fish eaters from Burma is the City of Buffalo. The target populations will be sampled, recruited, and enrolled independently.
NYS Licensed Anglers:
Response rate
A 46% response rate is projected for the New York State Department of Health (NYS DOH) program which will utilize a NYS database of issued fishing licenses. The sampling frame will be created using the 2010-2011 fishing license database by extracting records (i.e., licenses) as follows: license type (resident season or resident lifetime), 18-69 years of age at the end of the fishing season (9/30/2011), and a residential address with a ZIP Code in the study area as defined above. The sampling frame will be comprised of about 82,000 licenses as indicated by 2009-2010 data. Based on response rates to the New York Angler Surveys of 1991 and 2008, NY DOH anticipants that about 30% of anglers who are mailed the screening survey will respond. (Bloom, et al. 2005) Two members of the NY DOH program’s advisory committee, Matthew Bonner and Michael Bloom, were investigators for the 1991 and 2008 surveys and advised that the current program should expect a similar response to the mailing. For this reason, the NY DOH will mail the screening packet to a randomly selected sample of 14,400 anglers in the sampling frame in order to provide a sufficient number of licensed anglers to recruit 400 participants. The program estimates that 864 people who respond to the screening survey will meet the eligibility criteria. Eligible respondents will be called by interviewers to be invited to participate and to schedule an appointment to meet the recruitment goal of 400. These response estimates assume a 30% response to the screening survey, a conservative eligibility rate of 20%, and a participation rate (i.e., completes the clinic assessment and provides specimens) of 46%. Nonresponse bias for response to the screening survey will be assessed between people who respond to the screening questionnaire and those who do not using data extracted from the fishing license database. Nonresponse bias among eligible respondents will be evaluated by using data collected as part of the screening survey.
Sampling method
The respondent population is persons aged 18-69 years old who purchased a state resident seasonal or lifetime fishing license with a residential address in the study areas and who fished in the AOCs and ate their catch in the past year. The sampling frame will be drawn from a database of sport fishing and hunting licenses maintained by the New York State Department of Environmental Conservation (DEC). NYS law requires that any person 16 years of age or older must purchase a license and carry it on his/her person when he/she fishes or hunts in the state. The database contains all licenses sold and includes the following data fields: the type of license, the season during which it was purchased (a season is October 1 to September 30), the license holder’s name, residential address, telephone number, email address (optional), sex, and date of birth. Because the purchase of a license is required by law and functions much the same as a driver’s license, the license database is considered a complete and accurate list of sport (i.e., non-commercial) anglers. This database does not, by definition, capture persons who fish illegally. Illegal anglers comprise a separate population that might have different fishing and fish consumption habits.
The NYS DEC provided the fishing license database for the 2009-2010 fishing season to be used for planning purposes (e.g., to estimate the number of persons that will be in the sampling frame and who will be mailed recruitment information). At the close of the 2010-2011 season (the season closest to the initiation of biomonitoring), we will be provided with that database to create the sampling frame. The number of licenses sold in the study area ZIP Codes was estimated based on the proportion of each county’s population in the study area (see table below). We estimate that about 54,000 fishing licenses (with or without hunting privileges) were sold in one season within a 10-mile buffer of the AOCs in Erie and Niagara Counties, and about 28,000 were sold in a 10-mile buffer of the AOC in Monroe County.
Table 2. Populations 15-69 years old and estimated number of season and lifetime fishing licenses sold in 2009-2010 within a 10-mile buffer of the AOCs
County |
Total population |
Population in 10-mi. buffer |
Total fishing licenses sold 2009-2010 |
Estimated fishing licenses sold to residents in 10-mi. buffer |
Erie and Niagara |
807,567 |
728,096 90% |
59,250 |
53,419 |
Monroe |
534,301 |
459,511 86% |
32,181 |
27,676 |
The sampling frame will be created using the 2010-2011 fishing license database. We will extract records (i.e., licenses) as follows: license type (resident season or resident lifetime), 18-69 years of age at the end of the fishing season (9/30/2011), and a residential address with a ZIP Code in the study area as defined above. We will exclude records with a missing ZIP Code or an incomplete mailing address. We will also sort and match records on various fields, such as name and address, to remove duplicate individuals. Because the response rate to the screening is expected to be relatively low, at this stage we will not exclude different individuals with the same address. We expect that the sampling frame will be comprised of about 54,000 licenses in the Erie-Niagara study area and about 28,000 in the Monroe study area.
The overall participation goal is 400 licensed sport anglers who ate their catch in the previous year. Based on 2009-2010 fishing license sales, 62% of the licenses were sold in Erie and Niagara Counties and 38% in Monroe County. Therefore, of the total participation of 400 licensed anglers who eat fish, there will be 250 participants in the Erie-Niagara study area and 150 in the Monroe study area. The participants from the two study areas will be pooled into a single cohort of sport anglers who eat their catch.
License holders in the sampling frame will be randomly selected and mailed a recruitment package to determine eligibility. The recruitment packet includes a cover letter, a fact sheet about the project, the screening survey which includes maps of the AOC areas, and a return stamped envelope (Attachment 6a). The recipient can complete the survey and return it by mail or can complete the survey online (Attachment 6b, 6c). Before initiating recruitment, NY DOH will conduct outreach activities to media and community organizations to increase participation. A project fact sheet will be distributed at appropriate locations, such as bait and tackle shops. Additional outreach may be conducted in neighborhoods where barriers to participation are identified and in areas known to have a high proportion of anglers who eat their catch. To be eligible, the license holder must: (1) have lived at the address on the fishing license for at least one year before the screening date; (2) have eaten at least one fish caught in the AOCs in 2011 if being screened in 2012 (or 2012 if being screening in 2013); (3) have been 18-69 years old on 9/30/2011; and, (4) responded to the screening survey.
Table 3. Recruitment steps and number of anglers to reach participation goals, assuming 50% and 70% response rates, by study area
Recruitment step |
Study areas |
Study areas |
||
Erie-Niagara |
Monroe |
Erie-Niagara |
Monroe |
|
Fishing licenses (# anglers) |
54,000 |
28,000 |
54,000 |
28,000 |
Randomly select |
5.8% |
6.7% |
4.1% |
4.8% |
Mail screening survey (# anglers) |
3,125 |
1,875 |
2,232 |
1,339 |
Screening response rate |
50% |
50% |
70% |
70% |
Screened for eligibility (# anglers) |
1,562 |
938 |
1,562 |
938 |
Eligibility rate |
20% |
20% |
20% |
20% |
Eligible (# anglers) |
312 |
188 |
312 |
188 |
Participation rate |
80% |
80% |
80% |
80% |
|
|
|
|
|
Participants (#anglers) |
250 |
150 |
250 |
150 |
NYS Refugees and Immigrants from Burma:
Response rate
Using a networking driven sampling strategy appropriate for ‘hidden populations’ such as NYS refugees and immigrants from Burma, a response rate of 81% is projected. A high participation rate can be achieved because the respondent driven sampling (RDS) strategy uses peer-recruitment. The initial recruits, referred to as seeds, will be individuals who are well-connected and respected in the community and interested in participating in the project. The respondent driven sampling strategy affords a dual incentive system that helps maximize response. In addition to the typical material incentive that programs provide as a token of appreciation, RDS uses peer-recruitment and thus has a social incentive for people to participate. The enrollment goal for the Burmese target population is a minimum of 100 persons who eat fish caught in the AOCs.
Sampling method
Because there is no known sampling frame for the Burmese who eat fish, respondent-driven sampling (RDS) will be used. RDS is suitable for reaching “hidden” populations for which there is no known sampling frame (Lee 2011; Lansky 2007). RDS has been shown to increase efficiency and decrease cost compared to other sampling designs and has been shown to be suitable for refugee populations (Sabin 2011). For several reasons, RDS will be an effective approach for recruiting the Burmese. By virtue of being refugees, the Burmese are socially connected culturally, geographically, and, to some extent, politically. Second, information about the Burmese living in Buffalo indicates that individuals will have knowledge of each other’s fishing and fish consumption habits. Third, high participation rates can be achieved because RDS uses peer-recruitment. The initial recruits, referred to as seeds, will be individuals who are well-connected and respected in the community and interested in participating in the project. These assumptions will be verified during formative research. RDS has been shown to increase efficiency and decrease cost compared to other sampling designs.
This respondent population includes refugees and immigrants from Burma and their descendants who live in the City of Buffalo and eat fish caught in the AOCs. This population is known to consume fish from the upper Niagara River such as carp that have relatively high levels of PCBs. The Burmese in the City of Buffalo are concentrated in three contiguous neighborhoods that abut the Niagara River AOC and 3 to 5 miles of the Buffalo River AOC. According to the 2010 census tract data, approximately 2,289 ethnic Burmese live in these neighborhoods. To be eligible to participate in this part of the project an individual must be a refugee/immigrant from Burma or a descendant of someone from Burma, be 18 to 69 years old, have lived in the City of Buffalo or its surrounding communities for at least one year, have eaten 12 meals in the past year (an average of one per month) of fish caught in the AOCs, and, finally, must not have participated in the project as a licensed angler. Because we are assuming this population is subsisting on fish caught in the AOCs, at least to some degree, we have set the fish consumption eligibility criterion higher than for the licensed anglers. Our enrollment goal for the Burmese target population is a minimum of 100 persons who eat fish caught in the AOCs.
B.2. Procedures for the Collection of Information
Michigan:
MDCH will work with the Advisory Committee to select appropriate locations at which to hold collection clinics where participants will be administered the study questionnaire and provide biological samples. Locations to be considered include local community centers, local health department facilities, and community medical clinics.
Selected participants will be contacted by telephone to determine their continued willingness to participate and to schedule an appointment at a collection clinic. The phone script for these contacts (Attachment 4b) will be administered to determine if potential participants have a medical condition that will exclude them from participation. Woman who are pregnant or breastfeeding, and people who have lost more than 15 pounds in the last year will not be allowed to participate because these conditions can affect steady state body burden levels of target analytes. People who have hemophilia or any other blood clotting or bleeding health problem, have had chemotherapy in the previous six months, or weigh less than 95 pounds will not be allowed to participate because they may not be able to safely provide the volume of blood needed for this study. Potential participants will be called six times on different days and times, including weekends and weekday nights, and messages will be left on answering machines. Six more telephone calls will be attempted before classifying the individual as not reachable after which a replacement will be randomly selected from the list of eligible participants generated in the secondary enumeration phase of sampling.
Participants’ will be mailed an appointment reminder, a map, and a copy of the consent form. Transportation, likely by cab, to collection clinics will be arranged for participants who indicate this need.
Upon participant’s arrival at a collection clinic, project staff will match the participant’s name to a list of scheduled appointments and project identification numbers (ID) numbers. Labels containing only the project ID number will be used to identify biological sample containers. Biological samples will be collected by a Certified Phlebotomy Technician or other qualified person (e.g., nurse). No special instructions such as fasting or special diets are required. Project staff will explain and obtain signed Informed Consent (Attachment 4c) and verify contact information (Attachment 4d) prior to administration of the questionnaire and collection of biological samples.
MDCH project staff will administer the structured interview questionnaire. The interviewer will ask the participant each question and will record responses in a computer assisted personal interviewing (CAPI) data collection method using portable personal computers. CAPI developers will program skip logic and editing functionality such as field restrictions and automatic validity checks to help ensure data quality and minimize missing data. The interview questionnaire will be used to identify personal behaviors (e.g., consumption of sport caught fish, occupation) or characteristics (e.g., gender, age, diet, weight) that could affect levels of target analytes in participants’ blood and/or urine. (Attachment 4e).
To measure weight, the participant will stand on a floor scale that is equipped with a digital read-out. Height will be measured using a wall-mounted stadiometer. Weight and height will be recorded and the body/mass index (BMI) will be calculated using the following formula: BMI = Weight in Pounds / (Height in inches )2 x 703. Blood Pressure will be taken by clinic staff before collecting blood as a health service to the participant. Participants will be given an American Heart Association blood pressure information (Attachment 10a6) sheet to take with them. Blood pressure readings will be verbally shared with participants and recorded, but will not be retained for any analytical purpose. Blood pressure readings will not be retained as part of the study information.
The Certified Phlebotomy Technician or other qualified person will collect approximately 83 milliliters (mL) of blood by venipuncture from all consenting participants. Blood samples will be collected in eight red top 10-mL glass Vacutainer® tubes (organics) and one purple-top 3 mL EDTA tube (metals). After collection, the red-top tubes will be placed upright in a rack and allowed to clot at room temperature for 20 to 30 minutes, not to exceed one hour after sample collection. Red top tubes are then centrifuged for 15 minutes, and serum transferred to an appropriate storage vessel. Serum samples will be placed into a freezer within 90 minutes of the whole blood draw, then transported on ice to the MDCH laboratory for analyses or shipment as described below. The purple-top tube for metals analysis will be frozen, stored on ice, and delivered to the MDCH laboratory for analyses. Urine samples will be collected in a standard prescreened polypropylene urine cup. The samples will then be stored on ice and delivered to the MDCH laboratory for analyses. The ideal urine specimen amount is 4 to7 mL, with a minimum of 2 mL. If specimen amount is less than 2 mL or contamination is suspected, a second sample should be requested.
At the completion of the clinic visit, participants will receive a $25 gift card for completing the questionnaire, a $25 gift card for the blood and urine collection, and an additional $25 gift card if they complete both parts.
A Manual of Operating Procedures will document standardized procedures to be used in all collection clinics. Blood samples will be collected by Certified Phlebotomy Technicians or other qualified staff. Clinic staff will also be trained to collect urine samples. Interviewers will complete a comprehensive training program in the use of survey instruments, including survey techniques such as methods for converting non-responders. Training materials will be developed to provide interview trainees with interactive role plays for practice on the questionnaire and key skills needed to successfully engage study participants.
Sample size was assessed to assure the ability to detect mean analyte levels above NHANES population means with 80% power with a one-sided test of significance at level alpha=0.05. In NHANES, all contaminant levels were log-transformed; therefore, the geometric means (GM) and 95% confidence intervals (CI) are reported. The standard deviation of the log-transformed analyte was back-calculated from the CI and assumed to be the same for the Great Lakes population. The standard deviation (SD) is related to the coefficient of variation (CV) by the equation SD = [log(1+CV2) ]1/2. Calculations are provided in the table below for target analytes available in NHANES, with the exception of those with a high proportion of levels above the method detection limit (i.e., DDT and Mirex).
The NHANES levels represent the general United States population for all ages and sexes. The NHANES design does not select or exclude participants on the basis of their potential for low or high exposure to a chemical. The Great Lakes population of urban shoreline anglers will be adults with a higher likelihood of exposure to Great Lakes contaminants because they eat at least two local-caught fish meals per month; therefore, we anticipate increased body burden levels of target analytes in this sub-population. As illustrated in the table below, a sample of 400 should be sufficient to detect a minimum increase in geometric means of target analytes among the shoreline anglers of at least 50-100% above reported NHANES levels.
Table 4. Minimum GM and percent above NHANES GM detectable among the Great Lakes shoreline anglers for N=400 (80% power, one-sided alpha=0.05) in nanograms per gram (ng/g), micrograms per liter (ug/L), or micrograms per deciliter (ug/dL)
Contaminant |
2003-2005 NHANES |
Urban Shoreline Anglers (N=400) |
||
Geometric mean (GM) |
Predicted GM |
Percent Above NHANES GM |
||
PCBs (ng/g lipid-adjusted) |
||||
PCB 28 |
4.90 |
6.7 |
36% |
|
PCB 52 |
2.66 |
4.1 |
53% |
|
PCB 101 |
1.65 |
2.5 |
54% |
|
PCB 138 + 153 |
15.1 |
20.6 |
37% |
|
PCB 153 |
19.8 |
25.9 |
31% |
|
DDE (ng/g) |
238 |
-- |
>100% |
|
Hexachlorobenzene (ng/g) |
15.2 |
19.2 |
26% |
|
Mercury (μg/L) |
0.80 |
-- |
>100% |
|
Lead (μg/dL) |
1.43 |
2.25 |
57% |
|
Potential participants will be drawn from the FDL-HSD Client List (described above). The sampling frame is comprised of all eligible persons whose names are in the FDL-HSD Client List covering the three year period up to the date on which the list is pulled. Tribal representatives have indicated that this list is the most current and complete record available to develop a population-based survey of the FDL Community. All clients are either enrolled in an American Indian tribe or affiliated with a tribe (i.e., descendant of enrolled member).
In batches of eligible people drawn from the Client List (e.g., 60 at a time), the Recruiter will attempt to contact each person by phone. For those contacted, the Recruiter will follow a script to provide basic introduction about the study and verify eligibility based on age, residence, and by asking women whether they are pregnant (Attachment 5a). If a person contacted is not eligible, study staff will document the reason.
If the person is eligible and willing to consider taking part in the study, the Recruiter will schedule the clinic visit for sample collection and interview with the potential participant. The Recruiter will also give potential participants instructions regarding their activities on that day or make necessary arrangements (e.g., schedule transportation to and from the appointment). The Recruiter will confirm the mailing address and send the study Individual Consent Form (Attachment 5c). The consent form serves to introduce the study in detail and describe the selection process, explain the purpose of the study, and describe participant activities in addition to all usual elements of informed consent. If a potential participant decides they are no longer interested in participating after receiving the consent form, they can call the Recruiter to cancel their clinic visit. The Recruiter will then attempt to document the reason for refusal.
If the person is not interested taking part in the study, the Recruiter will document the reason for refusal, and administer the Refusal Questions Form (Attachment 5b) for nonresponse analysis. If the person is undecided, the Recruiter will attempt to answer questions or address concerns about the study.
For persons who cannot be contacted, the Recruiter will log the date and time or the attempt and note the outcome and any actions taken or information received (e.g., left a message, spoke with other person, given new number, best time to call is, etc.). After 10 unsuccessful attempts (different times of day and different days of week) to contact a potential participant, the Recruiter will ask FDL Public Health Nursing staff if they have further information or advice to help locate the individual. If necessary or advised, the Recruiter may attempt to locate the individual in person by visiting the most current address listed or as otherwise suggested by FDL Public Health Nursing Community Health Representatives. If he/she is located, study staff will try to speak with the person face-to-face to identify a phone number or other mechanism to recontact the person to assess willingness to participate. A description of contacting and enrolling participants is outlined in the Recruitment Calling Script (Attachment 5a). Contact and data collection materials are provided in Attachments 5a – 5g.
Some eligible persons may not have phones, phone numbers may not be available in the Client List, or the number may not be current. Because there may be systematic differences between those who do and those who do not have phones or current numbers listed, study staff will try to employ alternative contact methods to attempt to recruit them into the study. If an individual indicates (at any point) they are not able or willing to participate, the Recruiter will attempt to collect information about the reason for refusal. Information regarding age, gender and tribal affiliation will be used to compare characteristics of non-participants and participants, as this may be a source of refusal/nonresponse bias. A data system to track each potential participant through the recruitment process will be maintained by the FDL-HSD.
As described in the section above, study staff will send an Individual Consent Form (Attachment 5c) to each potential participant who expresses interest in taking part in the study. At the beginning of the clinic visit, study staff will meet with the participant to go over the consent materials and obtain a signature, indicating understanding and informed consent, prior to collection of specimens and the interview. After a participant gives consent trained staff will obtain updated contact information (Attachment 5d), perform routine clinical measurements (height, weight, waist circumference, history of weight loss or gain, and blood pressure) and collect blood and urine specimens (Attachment 5f). The survey questionnaire will be administered following collection of biological specimens (Attachment 5e). There will be only one appointment per participant.
At the end of the clinic screening, a maximum of $75 dollars in gift cards may be distributed to each participant for successful completion of the IC. As thanks for taking part, each participant will receive a $25 gift card for blood and urine collection, and a $25 in gift card for the interview and clinical assessment. An additional $25 gift card will be given to each participant for completing both parts of the study. A record of receipt will be kept for gift cards given out to participants (Attachment 5g).
All study records will be kept secure, including information about persons who chose not to participate or are ineligible. Individual participants will not be identified in any reports, documents, or other released information related to this study. Study staff will not disclose any information that might identify individual participants. ATSDR will receive individual de-identified data for the purpose of aggregating data from the three states undertaking Great Lakes Biomonitoring Program studies.
Written informed consent will be obtained from each participant. All consent documents will meet requirements under federal rules and policies for informed consent developed by the U.S. Department of Health and Human Services. In addition, FDL Reservation Business Committee, based on recommendations from the Institutional Review Board of the FDL-HSD, reviewed the procedures for obtaining and documenting informed consent. Study staff will follow the Study Protocol in all interactions with participants or potential participants. Originals of all signed consent/assent forms will be filed with study records, and copies will be given to the participants.
Minnesota Statutes Chapter 13 (Minnesota Government Data Practices Act) classifies individual biomonitoring data as private health data. As such, biomonitoring results with personal identifiers may be released only to the participant. Section 144.658 of the act specifies that “health data on an individual collected by public health officials conducting an epidemiologic investigation to reduce morbidity or mortality is not subject to discovery in a legal action.”
Secure management of the data will be a joint MDH-FDL tribal endeavor. The Min No Aya Win Clinic and the MDH Data Center in St. Paul are restricted-access secure facilities. After-hour physical security is provided in the form of a motion-sensor alarm system at the clinic and around the clock security guards and patrols at MDH. Employees at both facilities are required display ID badges at all times. Recruiters contacting potential participants after clinic hours will use FDL HSD computers at the FDL Assisted Living Facility, which has 24-hour staff access.
Paper documents at both facilities will be kept in secure (locked) rooms in locked file cabinets. Study staff will physically transport paper and electronic records and biospecimens from the Min No Aya Win Clinic to the MDH Data Center and MDH Public Health Laboratory. Electronic study files will be maintained behind MDH and FDL firewalls with antivirus and password protection. Data on FDL and MDH servers are backed up every 24 hours. At MDH, offsite backups occur weekly. Both MDH and FDL computers meet Federal Government data encryption standards. All MDH computers are currently migrating from PointSec to Microsoft’s Bitlocker Full Disk encryption, using the highest level of security.
All information in identifiable form (IIF) will be kept only at the Min No Aya Win Clinic in a separate, secure database, which will provide the link to participant responses, measurements, and lab results, by study ID numbers. All biospecimens sent to the four laboratories for analysis will be labeled only with these ID numbers. All study results will be kept separate from the participant’s medical record; participants may independently choose to provide them to a health care provider. Neither MDH nor ATSDR will receive IIF from the FDL-HSD.
At the end of the study, flat files of de-identified data will be provided to ATSDR. No personally identifying information will be transmitted or made available. Procedures for secure data transfer of de-identified data to ATSDR will be developed in collaboration with ATSDR. All public releases of data or publications based on study data must be approved by both the MDH Principal Investigator and the FDL Human Services Department.
Sample size assessments were made to assure the ability to detect mean analyte levels above or below NHANES population means with 80% power with a one-sided test of significance at level alpha=0.05. In NHANES, all contaminant levels were log-transformed; therefore, the geometric means (GM) and 95% confidence intervals (CI) are reported. The standard deviation of the log-transformed analyte was back-calculated from the CI and assumed to be the same for the Great Lakes population. The standard deviation (SD) is related to the coefficient of variation (CV) by SD={log(1+CV2) }1/2. Calculations are provided in Table 4 for core contaminants available in NHANES, with the exception of those with a high proportion of levels above the method detection limit (namely, DDT, mirex, dieldrin).
The NHANES levels represent the general U.S. population, regardless of the potential for exposure to the measured contaminants. The study population will be adults with a higher likelihood of exposure to the Great Lakes legacy pollutants; therefore, we expect higher levels in this target population. With a sample of 500, we should be able to detect a minimum increase of GM among the Tribal Community at least 30-138% above NHANES.
Table 5. Minimum GM and percent above NHANES GM detectable among the Great Lakes FDL community for N=500 (80% power, one-sided alpha=0.05) |
|||
Contaminant |
2003-2005 NHANES |
GL Biomonitoring Project (N=500) |
|
Geometric mean (GM) |
Corresponding GM |
Above NHANES GM |
|
PCBs (lipid-adjusted) |
|
|
|
PCB 28 |
4.90 |
6.5 |
32% |
PCB 52 |
2.66 |
3.9 |
47% |
PCB 101 |
1.65 |
2.4 |
48% |
PCB 138 + 153 |
15.1 |
20.1 |
33% |
PCB 153 |
19.8 |
25.2 |
28% |
Perfluorinated compounds |
|
|
|
PFOS |
20.7 |
29.0 |
40% |
PFOA |
3.95 |
5.6 |
42% |
DDE |
238 |
509 |
114% |
Hexachlorobenzene |
15.2 |
18.7 |
23% |
Mercury (µg/L) |
0.80 |
1.9 |
138% |
Lead (µg/L) |
1.43 |
2.16 |
51% |
New York Licensed Anglers:
Eligibility screening (described above) responses will be entered into a database and merged with the original license database record and the name and address of the respondent will be confirmed against the license database. Eligibility will be determined from information in the license database and responses to the screening survey (Attachment 6a-6c). If the respondent is eligible (i.e., checked all three items), he/she is asked for an email address, telephone numbers, and best times to be reached. Non-respondents will be telephoned to verify their mailing address and will be asked if they would like to complete the survey over the phone.
An interviewer will call each potential participant to determine interest in the study and enroll him/her. Potential participants will be called six times on different days and times, including weekends and weekday nights, and messages will be left on answering machines. Six more telephone calls will be attempted before classifying the individual as not reachable. To be enrolled in the study an angler must (1) be interested in participating, (2) verify the information on the screening survey, (3) be physically able to participate (i.e., travel and donate blood and urine), and (4) schedule an appointment to complete the interview and specimen collection. The participant will be offered a list of dates, times, and locations for conducting the interview and sampling. A reminder call will be made a few days before the appointment confirming the date and location of the appointment and other pertinent information (such as directions to the sampling location, persons to contact for questions). Individuals who complete the screening interview but are ineligible or refuse to participate will be given a small gift for their effort (i.e., a T-shirt and fishing license case with the fish advisory website link).
The study will be conducted at a clinic or similar facility that will allow privacy for the interview and specimen collection. The identity of the participant will be verified and the participant’s informed consent will be obtained. The participant will be interviewed, will have a sample of blood drawn, and provide a urine specimen. We will not verify eligibility at the appointment because we have verified eligibility in the screening and enrollment phases. We expect that some participants will be found ineligible based on the data collected during the interview, but we will let the participant complete the visit rather than turn him/her away after making the effort to come to the clinic. In addition, some participants will be unable to donate a specimen or the specimen may become unusable (e.g., clotted or contaminated). The former will be considered post-participation ineligible and the latter post-participation incomplete. For the ineligible participants and those without a usable specimen, any data that are collected will be omitted from the final datasets.
For the licensed anglers the participant will be given a quiet place to read the consent document, which will be available in English and Spanish. If a participant expresses difficulty with reading, the consent document will be read to them by an interviewer. Before beginning any procedures, a trained interviewer will ask the participant if he/she has any questions. When the participant’s questions have been answered to his/her satisfaction, the participant and the interviewer will sign the consent form. At the end of the appointment, the participant will be given a copy of the consent document and a gift cards for up to $75 as a token of appreciation for participating in the project. Participants will receive a $25 gift card for completing the questionnaire, a $25 gift card for the blood and urine collection, and an additional $25 gift card if they complete both. No gift cards for any incidental expenses (such as travel) will be provided.
With our sample size fixed at 400 sport anglers, sample size assessments were made to assure the ability to detect mean analyte levels above the NHANES population means with 80% power and a one-sided test of significance at level alpha= 0.05 (Appendix 13). In NHANES, all contaminant levels were log-transformed; therefore, the GM and 95% confidence intervals (CI) are reported (CDC 2009). The standard deviation (SD) of the log-transformed analyte was back calculated from the CI and assumed the same for the Great Lakes population of sport anglers. The standard deviation (SD) is related to the coefficient of variation (CV) by SD=[log(1+CV2)]1/2. Calculations are provided for core contaminants available in NHANES, with the exception of those with a high proportion of levels above the method detection limit (namely, BDE-66, 85, 99, 154, DDT, Mirex, dieldrin, trans-nonachlor).
The NHANES levels represent the general U.S. population of all ages and sexes, regardless of the potential for exposure to the measured contaminants. The Great Lakes population of anglers will be adults, primarily men, and with a higher likelihood of exposure to the Great Lakes legacy pollutants; therefore, we expect higher levels in the targeted population. We expect to be able to detect a GM among the Great Lakes licensed sport anglers for PCB 138 + 153 (coeluted congeners) of at least 22% above the NHANES GM, 31% for PCB 153, and 36% for PCB 28, 26% for hexachlorobenzene, 44% for oxychlordane, and 45% and 46% for PFOS and PFOA, respectively. For the remaining contaminants, we would only be able to detect an elevation above 50%, and for DDE and mercury above 100% (Table 6).
Table 6. Minimum geometric mean (GM) and percent above NHANES GM detectable among the Great Lakes licensed sport anglers for N=400 (80% power, one-sided alpha=0.05)
Contaminant |
2003-2005 NHANES |
GL biomonitoring project (N=400) |
|
GM |
GM |
Above NHANES GM |
|
PCBs (lipid-adjusted) |
|
|
|
PCB 28 |
4.90 |
6.7 |
36% |
PCB 52 |
2.66 |
4.1 |
53% |
PCB 101 |
1.65 |
2.5 |
54% |
PCB 138 + 153 |
15.1 |
20.6 |
37% |
PCB 153 |
19.8 |
25.9 |
31% |
PBDEs (lipid-adjusted) |
|
|
|
BDE 28 |
1.19 |
2.2 |
85% |
BDE 47 |
20.5 |
40.0 |
95% |
BDE 100 |
3.93 |
7.3 |
85% |
BDE 153 |
5.69 |
9.4 |
66% |
Perfluorinated compounds |
|
|
|
PFOS |
20.7 |
30.1 |
45% |
PFOA |
3.95 |
5.8 |
46% |
DDE |
238 |
-- |
>100% |
Hexachlorobenzene |
15.2 |
19.2 |
26% |
Oxychlordane |
9.37 |
13.5 |
44% |
Trans-nonachlor |
14.7 |
24.8 |
69% |
Mercury (µg/L) |
0.80 |
-- |
>100% |
Lead (µg/L) |
1.43 |
2.25 |
57% |
New York Refugees and Immigrants from Burma
The RDS process will starts with a formative research phase during which NYS DOH staff works with local community groups and individuals in the community to identify the “seeds.” A seed is an initial recruiter who meets the eligibility criteria and is a member in good standing of the community. NYS DOH staff will select 6 to 10 seeds that have large social networks. If we learn that women and men have limited social interactions (are less likely to recruit peers of the opposite sex), we will select both male and female seeds, or if social interactions are closer among certain ethnic or political subgroups, we will identify seeds based on these characteristics.
Eligibility will be determined using a screening survey. The survey, as well as the interview questionnaire, will be translated into Burmese and administered by a Burmese interpreter. By definition, seeds are eligible to participate. In addition to the eligibility criteria listed above, to be eligible, recruited individuals must know the recruiter, not be a family member, and not have already participated in the project (as a licensed angler or Burmese who eats their catch).
After completing the interview and providing blood and urine samples, each seed is trained on how to recruit Burmese in the target population. Each seed is given three referral coupons to distribute to individuals in his/her network. The coupons are uniquely numbered, so that the recruiter can be linked to his/her recruits, and include instructions on how the recruited peer can participate in the project. A recruit brings the coupon to a site, is screened for eligibility, and is invited to complete the procedures. The participant is then offered the chance to be a recruiter and, if he/she accepts, is trained and given three coupons. Seeds and recruiters are given a gift card as a token of appreciation for each person who is eligible and completes the procedures. To successfully use RDS, we will set remuneration appropriately, ration the coupons (3 per recruiter), track the coupons associated with each recruiter (including the seeds), record the network size of each recruiter, and document the relationship of the recruit to the recruiter. As we reach our target enrollment, we will add an expiration date to the coupons and reduce the number of coupons per participant (for example, two coupons when we reach 80% of the enrollment goal, one coupon when we reach 95%).
Each set of recruits from a single recruiter is a recruitment “wave.” The recruitment process continues until either enrollment goals have been met or equilibrium is reached. Equilibrium is the expected sample composition had the initial participants been selected at random. As part of RDS we will track the traits of the participants, including sex, age, the neighborhood where they reside (current address), and how many years they have lived in the U.S. We expect that we can reach our goal of 100 Burmese anglers quickly using RDS, provided that each participant can make three referrals and that participation is high. For example, one seed (wave 0) recruits three people, all three show up at the project site, and two are eligible and participate (screening and participation occur at the same place and time). This wave (wave 1) produces two new participants. If this scenario continues through four waves, one seed will generate 31 participants, six seeds generate 186 participants, and 10 seeds generate 310 participants. Some seeds may “dry out”; therefore, if possible, it is preferable to balance the number of seeds against the number of recruitment waves expected to reach the enrollment goal.
All contact, consent and data collection documents for the Burmese sample can be found in Attachments 6h – 6k. After confirming the prospective participant’s eligibility, he/she will be given a quiet place to read the consent document, which will be available in English and the primary Burmese language. If a participant expresses difficulty with reading, the consent document will be read to them by an interviewer or trained interpreter. Before beginning any procedures, a trained interviewer will ask the participant if he/she has any questions. When the participant’s questions have been answered to his/her satisfaction, the participant and the interviewer will sign the consent form. At the end of the appointment, the participant will be given a copy of the consent document along with their gift card as a thank you for participating.
At the end of the appointment, the participant will be given a copy of the consent document and a gift cards for up to $75 as a token of appreciation for participating in the project. Participants will receive a $25 gift card for completing the questionnaire, a $25 gift card for the blood and urine collection, and an additional $25 gift card if they complete both. If the participant chooses to be trained to recruit new participants, he/she will be given a $15 gift card for each referral who is screened, eligible, and agrees to participate. In addition to the clinic incentives, participants will be given at most $45 for recruiting three peers. Referred individuals who complete the screening interview but are ineligible or refuse to participate will be given a small gift for their effort (i.e., a T-shirt and fishing license case with the fish advisory website link). No gift cards for any incidental expenses (such as travel) will be provided.
Assuming sample sizes of Burmese who eat fish from the AOCs of 100, we calculated the percent above the NHANES population geometric mean that we would be able to observe with 80% power and a one-sided alpha of 0.05 (CDC, 2009). In NHANES, all contaminant levels were log-transformed; therefore, the geometric means (GM) and 95% confidence intervals (CI) are reported. We estimated the standard deviation from the CI and assumed the same SD for the Great Lakes population of sport anglers. We did this for all contaminants available in NHANES, with the exception of those with a high proportion of levels above the method detection limit (namely, BDE-66, 85, 99, 154, DDT, mirex, dieldrin, trans-nonachlor).
The NHANES levels represent the general U.S. population of all ages and sexes, regardless of the potential for exposure to the measured contaminants. The population of Burmese in Buffalo who eat fish from the AOCs will be adults with a higher likelihood of exposure to the Great Lakes legacy pollutants; therefore, we expect higher levels in this target population. With a sample of 100, we will only be able to detect a GM among the Burmese at least 50-100% above the NHANES GM for PCB 28 (73%), PCB 138+153 (74%), PCB 153 (62%), PFOS (91%), PFOA (95%), hexachlorobenzene (53%), and oxychlordane (89%). A doubling or more is required to detect an elevation in 100 Burmese for PCB 52, PCB 101, all PBDEs, trans-nonachlor, and lead, and a level of over 200% is needed to detect an elevation in DDE. These percentages drop by one-third if the sample size is 200 Burmese. For mercury, even a sample size of 200 requires a level at least 200% above the NHANES GM to detect a difference. Although these percentage differences may appear high, the Burmese who will be eligible to participate are required to have eaten relatively more fish from the AOCs and may also consume relatively more fish from other sources as well. The New York City Health and Nutrition Examination Survey found the highest concentrations of lead, cadmium, and mercury in the New York City Asian population, and the foreign-born Chinese in particular. In addition, mercury concentrations were 3.7 times higher in adults who ate fish or shellfish at least 20 times in the past month compared to adults who did not eat fish. (Table 7)
Table 7. Minimum geometric mean (GM) and percent above NHANES GM detectable among persons from Burmese who eat fish from the AOCs, N=100 and 200 (80% power, one-sided alpha=0.05)
Contaminant |
2003-2005 NHANES |
GM and percent above NHANES GM |
||
N=100 |
|
|||
GM |
GM |
Above NHANES |
|
|
PCBs (lipid-adjusted) |
|
|
|
|
PCB 28 |
4.9 |
8.5 |
73% |
|
PCB 52 |
2.66 |
-- |
>100% |
|
PCB 101 |
1.65 |
3.4 |
108% |
|
PCB 138 + 153 |
15.1 |
26.3 |
74% |
|
PCB 153 |
19.8 |
32.1 |
62% |
|
PBDEs (lipid-adjusted) |
|
|
|
|
BDE 28 |
1.19 |
3.3 |
173% |
|
BDE 47 |
20.5 |
6.0 |
191% |
|
BDE 100 |
3.93 |
10.7 |
170% |
|
BDE 153 |
5.69 |
13.2 |
132% |
|
Perfluorinated compounds |
|
|
|
|
PFOS |
20.7 |
39.5 |
91% |
|
PFOA |
3.95 |
7.7 |
95% |
|
DDE |
238 |
-- |
>200% |
|
Hexachlorobenzene |
15.2 |
23.2 |
53% |
|
Oxychlordane |
9.37 |
17.7 |
89% |
|
Trans-nonachlor |
14.7 |
35.1 |
139% |
|
Mercury (µg/L) |
|
-- |
-- |
|
Lead (µg/L) |
|
3.1 |
115% |
|
B.3. Methods to Maximize Response Rates and Deal with No Response
Michigan:
MDCH has convened two Advisory Committees: one for the Detroit area and one for the Saginaw area. Separate Advisory Committees were needed because of differing population concerns between the two areas and the need for committee members familiar with each community. The role of the Advisory Committee(s) is to:
1. Assist MDCH in identifying local interest groups and participant recruitment opportunities.
2. Advise MDCH on how to approach and engage members of the targeted population.
3. Review and provide comment on outreach materials.
4. Identify local resources necessary for implementation of the project such as medical clinics, communication networks, and community leaders.
5. Provide perspective on community concerns and issues.
6. Provide consultation on providing results to study participants.
7. Collaborate with community groups as needed.
Potential participants will be called six times on different days and times, including weekends and weekday nights, and messages will be left on answering machines. Six more telephone calls will be attempted before classifying the individual as not reachable after which a replacement will be randomly selected from the list of eligible participants generated in the secondary enumeration phase of sampling. During the secondary enumeration phase, people fishing will be asked to answer questions about eating local-caught fish, their age, gender, race/ethnicity. Expected response rates during study phases are presented above in section B.1. Information gathered during the secondary enumeration phase will be used to assess non-response bias by comparing people who indicate willingness to participate in the full study to those who decline participation.
Efforts to maximize participation also include providing information about the program and tokens of appreciation for participation. Anglers at shoreline venues will receive a small LED flashlight imprinted with the Michigan Fish Advisory internet address as a thank you for answering the screening questions; and, an informational brochure including MDCH contact information (Attachment 4a). Shoreline anglers who are selected to participate in the clinic screening will be offered transportation, likely by cab, to collection clinics if they indicate this is needed. Clinic participants will receive a $25 gift card for completing the biomonitoring questionnaire, a $25 gift card for the blood and urine collection, and an additional $25 gift card if they complete both parts.
Minnesota:
MDH will conduct the program in close collaboration with the FDL Community to encourage interest and active participation and to ensure that study findings are interpreted and disseminated in culturally relevant and useful ways. Staff will take steps to learn about the community (e.g., their beliefs, attitudes, values, behaviors, concerns, questions and intentions that are relevant to the project and the questions they will address), share information about the project, and take advice from stakeholders and other community representatives on virtually all aspects of the project. Many opportunities will be provided for community members and other stakeholders (e.g., staff in the Tribe’s Environmental Management program) to provide input on the study.
An FDL Advice Council comprised mainly of FDL community tribal members and other leaders is meeting regularly throughout the study to review proposed plans or draft materials and procedures and to offer guidance on topics related to cultural appropriateness, community collaboration and involvement, and protections for participants.
The study’s goal is to enroll 500 participants. Outreach and information dissemination will be conducted before and during the enrollment phase to familiarize the Community with the purposes and nature of the study. A participation rate of 80 percent is desired. The following list includes methods that will be employed to help attain recruitment goals:
Staff from MDH and FDL Public Health Nursing are working together to design the study.
Study staff and the Community’s leaders and members meet regularly via FDL Advice Council meetings to ensure that the study is conducted in ways that are respectful and relevant to the community. The Advice Council has already been meeting to learn about the study and review proposed plans or draft materials. They have provided guidance on topics related to cultural appropriateness, community collaboration and involvement, and other practical aspects of the study. In addition, the FDL Reservation Business Committee, based on recommendations of the FDL-HSD Institutional Review Board, will examine the proposed study and give approval or request modifications before the study is implemented.
Community outreach and information dissemination: Efforts to promote awareness of the study will be conducted to familiarize the community with the purpose and nature of the study at community health fairs and other public venues. Information will be shared through local news media (FDL website, newspaper, radio, and various newsletters), meetings with community representatives, and/or public meetings and forums.
Recruitment methods: Recruiters will be trained to maximize conversion of undecideds, unable-to-contacts, and soft refusals.
After 10 unsuccessful attempts (different times of day and different days of the week) or for those who do not have phones or current numbers listed, study staff will employ alternative contact recruitment methods:
The Recruiter may attempt to locate the individual in person by visiting the most current address on record. In such cases, study staff may hand deliver study information.
The Recruiter may also consult the FDL Community Health Representatives, as they are very familiar with the whereabouts of community members.
If these methods fail to result in contact, a “Call Us” mailing will be sent to “unable-to-contacts” 1-2 months prior to the end of study enrollment.
The response rate for the FDL Community is expected to be at least 70%. Information provided on the Client List used as the sampling frame and the Refusal Question Form (Attachment 5b) will be used to assess non-response bias by comparing people who indicate willingness to participate in the full study to those who decline participation. This analysis will include age, gender, tribal affiliation, and monthly fish consumption.
Efforts to maximize participation also include providing tokens of appreciation. In total, a maximum of $75 dollars in gift cards may be distributed to each participant for successful completion of the information collection. As thanks for taking part, each participant will receive a $25 gift card for blood and urine collection, and a $25 in gift card for the interview and clinical assessment. An additional $25 gift card will be given to each participant for completing both parts of the study. A record of receipt will be kept for gift cards given out to participants (Attachment 5g).
New York Licensed Anglers
An initial sampling frame of licensed anglers is estimated to include approximately 82,000 residences in the study area. Before initiating recruitment, we will conduct outreach to media and community organizations to increase participation. A project fact sheet will be distributed at appropriate locations, such as bait and tackle shops. Additional outreach may be conducted in neighborhoods where barriers to participation are identified and in areas known to have a high proportion of anglers who eat their catch. We will mail the screening packet to a randomly selected sample of 50% of the anglers in the Erie-Niagara study area and 60% of anglers in the Monroe study area. This should provide a sufficient number of licensed anglers to reach our participation goals. With intensive outreach to non-responders, we are aiming for a 70% screening response rate. As recruitment progresses, if the response rate is closer to 50%, we will mail the screening survey to an additional random sample.
The eligibility screening packet will include maps of the AOC areas, and a return stamped envelope. The recipient can complete the survey and return it by mail (Attachment 6b) or can complete the survey online (Attachment 6c). The online survey will be developed using Zoomerang and will have the same format as the paper survey. The fishing license database includes telephone number and email address, but reporting these on the application is optional. In 2009-2010, 85% of licensed anglers provided a telephone number. Publicly available records can also be used to find the telephone number for non-responders who did not provide it on the license application. Trained study staff will call non-responders who have telephone numbers to verify if they received the packet and, if not, verify their mailing address (Attachment 6d). They will be called up to three times on different days and times and messages will be left on answering machines. They will be offered the opportunity to complete the screening survey over the telephone, by mail, or online. Non-responders with an email address only will be sent up to three emails with the link to the online survey.
An interviewer will call each potential participant to determine interest in the study and enroll him/her (Attachment 6e). Potential participants will be called six times on different days and times, including weekends and weekday nights, and messages will be left on answering machines. Six more telephone calls will be attempted before classifying the individual as not reachable.
For the licensed anglers, to assess non-response bias we will compare the demographic characteristics to the demographics of the sampling frame, non-responders, and refusals. We will also geocode the addresses of the participants to determine the spatial distribution of the participants.
Consistent with the other state programs, efforts to maximize participation also include providing tokens of appreciation. As a thank you for taking part, each participant will receive a $25 gift card for blood and urine collection, a $25 gift card for the interview, and an additional $25 gift card for completing all parts of the study.
New York Refugees and Immigrants from Burma
RDS will be an effective approach for recruiting the Burmese. First, RDS is suitable for reaching “hidden” populations for which there is no known sampling frame. In addition, by virtue of being refugees, the Burmese are socially connected culturally, geographically, and, to some extent, politically. Second, information about the Burmese living in Buffalo indicates that individuals will have knowledge of each other’s fishing and fish consumption habits. Third, high participation rates can be achieved because RDS uses peer-recruitment. For the RDS component, we will generate sampling statistics, descriptive statistics of the partitions (for example, age, sex, employment, education, and income), and compare the estimated proportion of the population in each partition to the sampled population. Finally, we will compute homophily (the measure of preference for connections to an individual’s own group) for selected recruitment characteristics and compute network sizes.
Consistent with the state program clinic screenings, Burmese participants will be given gift cards for up to $75 as a token of appreciation for participating in the project. Participants will receive a $25 gift card for completing the questionnaire, a $25 gift card for the blood and urine collection, and an additional $25 gift card if they complete both. As part of the RDS, if the participant chooses to be trained to recruit new participants, he/she will be given a $15 gift card for each referral who is screened, eligible, and agrees to participate. In addition to the clinic incentives, participants will be given at most $45 for recruiting three peers. Referred individuals who complete the screening interview but are ineligible or refuse to participate will be given a small gift for their effort (i.e., a T-shirt and fishing license case with the fish advisory website link).
B.4. Tests of Procedures or Methods to be Undertaken
Each state program piloted the questionnaire interview and screening surveys on three people representative of their target audience. Since ATSDR is submitting the OMB package as a single program, we did not want the collective number of people to nine. Pilot testing served to identify questionnaire items that were not clear and to evaluate the burden that each item as well as total items posed. Questionnaire items were refined and items that posed a significant time burden for the information gained were eliminated.
The MDCH program pilot tested data questionnaires on community members who have been used as “river walkers” to interact with shoreline anglers in past MDCH surveys of shoreline anglers regarding fish advisories. MDC piloted tested their instruments on tribal members who are on staff. NY DOH also used staff members who meet their eligibility criteria as licensed NY anglers. Pilot testing of data collection instruments for the Burmese population will be performed pending approved translation.
B.5. Individuals Consulted on Statistical Aspects and Individuals Collecting and/or Analyzing Data
B.5.1 Study design and sampling plan:
The study design and sampling plan(s) for each state program were developed as a collaborative process between ATSDR subject matter experts, the National Center for Health Statistics and program-specific consultants and contractors.
ATSDR:
Wendy Wattigney, M.Stat. Robin Lee, Ph.D.
Mathematical Statistician Team Lead, Epidemiologist
770-488-3802 770-488-3811
WWattigney@cdc.gov RLee3@cdc.gov
Stephanie Davis, MSPH
Epidemiologist
770-488-3676
National Center for Health Statistics:
Lester Randy Curtin, Ph.D.
Mathematical Statistician
National Center for Health Statistics (NHANES)
301-458-4172
Michigan:
MDCH has a master contract with Michigan State University (MSU) to provide technical support for project activities such as study design, data analysis, and reporting. MSU personnel:
Joe Gardiner, Ph.D. Julie Wirth, Ph.D.
Professor
of Epidemiology and Statistics Assistant Professor of
Epidemiology
Director, Division of Biostatistics Michigan
State University
Michigan
State University Department of Epidemiology
(517) 353.8623
x110 517-432-8383x199
E-mail: gardine3@msu.edu Email: wirthj@msu.edu
MDCH has a master contract with Wayne State University (WSU) to conduct venue-based screening and recruitment activities in the summer of 2012 in the Detroit and Saginaw areas.
Dr. Andrea Sankar, Professor and Chair Wayne State University (WSU), Department of Anthropology, will oversee venue-based sampling activities to be conducted in the summer of 2012 in the Detroit and Saginaw. Dr. Todd Meyers is an assistant professor in the Department of Anthropology, Wayne State University. He is an experienced ethnographer and has conducted research in Baltimore Maryland that employed venue-based sampling to access hard to reach populations. Dr. Meyers will oversee formative research field activities in the Detroit and Saginaw areas. Dr. Sherylyn Hope Briller is an associate professor in the Department of Anthropology, Wayne State University. She specializes in sampling and research methods and will bring this expertise to the formative research activities.
Todd Meyers, Ph.D. Sherylyn Briller, Ph.D.
Assistant Professor Associate Professor
Wayne State University Wayne State University
Department of Anthropology Department of Anthropology
313-577-6795 313-993-4069
Eg1421@wayne.edu s.briller@wayne.edu
Andrea Sankar, Ph.D.
Professor & Chair
Wayne State University
Department of Anthropolpogy
313-577-6961
Minnesota:
Rita Messing, Ph.D. Deanna Scher, Ph.D.
Co-Principal Investigator Principal Investigator
Environmental Health Division Environmental Health Division
Minnesota Department of Health Minnesota Department of Health
651-201-4916 651-201-4922
Rita.Messing@state.mn.us deanna.scher@state.mn.us
David Jones, M.S.
Project Coordinator
Environmental Health Division
Minnesota Department of Health
651-201-4565
New York:
Syni-An Hwang, Ph.D.
Principal Investigator
Director, Bureau of Environmental & Occupational Research
New York State Department of Health
518-402-7950
Elizabeth Lewis-Michl, Ph.D.
Chief, Community Exposure Research
Bureau of Environmental & Occupational Research
New York State Department of Health
518-402-7950
Marta Gomez, M.S.
Research Scientist
Bureau of Environmental & Occupational Research
New York State Department of Health
518-402-7950
Julie Reuther, M.P.H.
Project Coordinator
Community Exposure Research
Bureau of Environmental & Occupational Epidemiology
New York State Department of Health
518-402-7950
Edward Fitzgerald, Ph.D.
Chair, Department of Epidemiology and Biostatistics
School of Public Health
University at Albany, SUNY
518-402-1062
Ralph R. Van Houten
Assistant Regional Director
NYSDOH
335 Main Street East
Rochester, NY 14604
585-423-8072
B.5.2 Questionnaire design
The questionnaire surveys were designed as a collaborative process between ATSDR Project Officers, staff from all three states programs and state-specific consultants. Weekly conference calls were held for a six month period to determine core elements common among all three programs and to discuss state-specific elements allowing for global input.
ATSDR:
Stephanie Davis, MSPH
Questionnaire lead
Project Officer, MN
Epidemiologist
770-488-3676
Wendy Wattigney, M.Stat. Elizabeth Irvin-Barnwell, Ph.D.
Project Officer, MI Project Officer, NY
Mathematical Statistician Epidemiologist
770-488-3802 770-488-3811
WWattigney@cdc.gov EIrvinBarnwell@cdc.gov
Michigan:
Technical Advisors:
Linda Dykema, Ph.D.
Toxicologist
Chief, Toxicology and Response Section
Division of Environmental Health
Michigan Department of Community Health
(517) 335-8350
DykemaL@michigan.gov
Kory Groetsch, M.S.
Toxicologist
Toxicology and Response Section
Division of Environmental Health
Michigan Department of Community Health
(517) 335-8350
GroetschK@michigan.gov
Susan Manente, M.A.
Health Educator
Toxicology and Response Section
Division of Environmental Health
Michigan Department of Community Health
(517) 335-8350
ManenteS@michigan.gov
Julie Wirth, Ph.D.
Assistant Professor
Michigan State University
Department
of Epidemiology
517-432-8383x199
Email: wirthj@msu.edu
David Karpovich, Ph.D.
Professor of Chemistry and Department Chair
Saginaw Valley University
989-964-4349
Maggie Tufts
Epidemiologist
City of Detroit Department of Health and Wellness Promotion
Community Advisors:
Mike Schram
Local angler
Chef, Gleaners Community Food Bank
Gary Williams
Local angler
Coordinator, 4-H Natural Resources Programs
Michigan State University Extension
Charles Stokes
Community Organizer
Detroiters Working for Environmental Justice
Minnesota:
Rita Messing, Ph.D. Deanna Scher, Ph.D.
Co-Principal Investigator Principal Investigator
Environmental Health Division Environmental Health Division
Minnesota Department of Health Minnesota Department of Health
651-201-4916 651-201-4922
Rita.Messing@state.mn.us deanna.scher@state.mn.us
David Jones, M.S.
Project Coordinator
Environmental Health Division
Minnesota Department of Health
651-201-4565
Patricia McCann, M.S.
Investigator
Environmental Health Division
Minnesota Department of Health
651-201-4915
Eileen Grundstrom, B.A.
Outreach Coordinator
Environmental Health Division
Minnesota Department of Health
651-201-4873
Jill Korinek, B.S.
Project Coordinator
Environmental Health Division
Minnesota Department of Health
651-201-4913
Jessica Nelson, Ph.D.
Epidemiologist
Health Promotion and Chronic Disease Division
Minnesota Department of Health
651-2-1-3610
Minnesota Fond du Lac Biomonitoring Advice Council:
Wayne Dupuis
Fond du Lac Natural Resources
Fond du Lac Environmental Program Manager
218-878-7106
Thomas Howes
Fond du Lac Natural Resources
Program Manager
218-878-7163
Bonnie LaFramboise, RN, PHN
Lead Public Health Nurse Consultant
Fond du Lac Human Services Division
218-878-2132
Nancy Schuldt
Fond du Lac Natural Resources
Water Projects Coordinator
218-878-7110
Deb Smith, PHN, RN, MSN
Fond du Lac Human Services
Public Health Nurse Director
218-878-2104
Carol Jaakola
Advice Council Member
Debra Johnson-Fuller
Advice Council Member
Dominic Johnson-Fuller
Advice Council Member
Marlene Shofner
Advice Council Member
Dave Wise
Advice Council Member
Joseph S. Wise
Advice Council Member
Louis Wise
Advice Council Member
New York:
Syni-An Hwang, Ph.D.
Principal Investigator
Director, Bureau of Environmental & Occupational Research
New York State Department of Health
518-402-7950
Elizabeth Lewis-Michl, Ph.D.
Chief, Community Exposure Research
Bureau of Environmental & Occupational Research
New York State Department of Health
518-402-7950
Marta Gomez, M.S.
Research Scientist
Bureau of Environmental & Occupational Research
New York State Department of Health
518-402-7950
Julie
Reuther, MPH
Research Scientist 2
Bureau of Environmental
and Occupational Epidemiology
Center for Environmental
Health
New York State Department of Health
518-402-7950
Edward Fitzgerald, Ph.D.
Chair, Department of Epidemiology and Biostatistics
School of Public Health
University at Albany, SUNY
518-402-0372
Karen Nolan, M.P.H.
Research Scientist
Community Exposure Research
Bureau of Environmental & Occupational Epidemiology
New York State Department of Health
518-402-7950
James Bowers, M.P.H.
Communication Specialist
Community Exposure Research
Bureau of Environmental & Occupational Epidemiology
New York State Department of Health
518-402-7950
June Moore, M.P.H.
Research Scientist
Community Exposure Research
Community Exposure Research
Bureau of Environmental & Occupational Epidemiology
New York State Department of Health
518-402-7950
Kamal-Nain Siag, M.P.H.
Community Exposure Research
Bureau of Environmental & Occupational Epidemiology
New York State Department of Health
518-402-7950
B.5.3 Data collection
Michigan:
Secondary enumeration at fishing venues: Wayne State University will employ four graduate students to conduct field work in the Detroit and Saginaw areas. Their activities will be overseen by:
Andrea P. Sanker, Ph.D.
Assistant Professor
Wayne State University
Department of Anthropology
313-577-6795; aa7651@wayne.edu
Recruitment and Questionnaire Interviews:
Susan Manente, M.A.
Health Educator
Toxicology and Response Section
Division of Environmental Health
Michigan Department of Community Health
(517) 335-8350
Kory Groetsch, M.S.
Toxicologist
Toxicology and Response Section
Division of Environmental Health
Michigan Department of Community Health
(517) 335-8350
Data Collection Clinic Consultants:
Shielda Braddock
Executive Director
First Ward Community Center
Saginaw, MI
989-753-0369
Christina Chingman
Registered Nurse
U.S. Department of Veteran’s Affairs
Saginaw, MI
Kathy McElroy
Chief, environmental Management Unit
Wayne County Health Department
Detroit, MI
Minnesota:
To be hired, under contracted supervision of:
Bonnie LaFramboise, RN, PHN
Lead Public Health Nurse
Consultant
Fond du Lac Human Services Division
218-878-2132
On behalf of:
David Jones, M.S.
Project Coordinator
Environmental Health Division
Minnesota Department of Health
651-201-4565
New York:
To be hired, under supervisions of:
Elizabeth Lewis-Michl, Ph.D.
Chief, Community Exposure Research
Bureau of Environmental & Occupational Research
New York State Department of Health
518-402-7950
The data collection/coordinator assistant will be recruited for and hired in Year 2 and continue at 100% effort for 12 months in Year 3 within the BEOE to assist the project coordinator in the field, arrange and organize the data collection venues, hire and train part-time interviewers as needed, schedule participants, conduct participant recruitment and interviews, collect and ship biological specimens, and assist with outreach and education.
B.5.4 Data Management
Michigan:
To be hired
MDCH will employ an entry level epidemiologist through the Michigan Public Health Institute (Lansing, Michigan) under a master agreement with the State of Michigan. The person is this position will perform data handling, cleaning, and management.
Minnesota:
Larry Souther, B.S.
Environmental Health Division
Minnesota Department of Health
651-201-4926
New York:
To be hired
The data management/coordinator assistant will be recruited for and hired in Year 1 and continue at 100% effort for 12 months in Year 2 and Year 3 within the BEOE to design databases and data entry programs, manage data, track data collection of interviews and laboratory data, assist with recruitment and data collection as needed, and conduct analyses as required.
B.5.5 Data Analysis
Michigan:
MDCH has a master contract with Michigan State University (MSU) to provide technical support for data analysis and reporting. MSU staff includes 1 graduate student to be hired and:
Joe Gardiner, Ph.D. Julie Wirth, Ph.D.
Professor of Epidemiology and Statistics Assistant Professor
Director, Division of Biostatistics Michigan State University
Michigan
State University Department of Epidemiology
(517) 353.8623
x110 517-432-8383x199
E-mail: gardine3@msu.edu Email: wirthj@msu.edu
Minnesota:
Deanna Scher, Ph.D.
Principal Investigator
Epidemiologist
Environmental Health Division
Minnesota Department of Health
651-201-4922
New York:
To be hired; Data analysis will be conducted by existing staff already listed including the data manager (to be hired) and Co-Investigator, Marta Gomez.
References:
Agency for Toxic Substances and Disease Registry (ATSDR). 1994. Health Study to Assess Methylmercury Exposure Among Members of the Fond du Lac Band of the Chippewa Indians in Northern Minnesota. Indian Health Service Bemidji Service Area, Bemidji, MN. NTIS Publication Number PB94-134798. US Department of Health and Human Services.
Bloom MS, Vena JE, Swanson MK, Moysich KB and Olson JR. Profiles of ortho-polychlorinated biphenyl congeners, dichlorodiphenyldichloroethylene, hexachlorobenzene, and Mirex among male Lake Ontario sportfish consumers: the New York State Angler Cohort Study.
Environmental Research. 2005; 97:178–194
Galea, S. and Tracy, M. Participation rates in epidemiologic studies. Annals of Epidemiology. 2007;17(9):643-653.
La Corte E, Wuttke S. The First Nations Biomonitoring Initiative-FNBI. Int J Hyg Environ Health. 2012;215(2):168-71.
Lansky A, Abdul-Quader AS, Cribbin M, Hall T, Finlayson TJ, Garfein RS, Lin LS, Sullivan PS. Developing an HIV Behavioral Surveillance System for Injecting Drug Users: The National HIV Behavioral Surveillance System. Public Health Rep 2007; 122 Suppl 1:48-55.
Lee R, Ranaldi J, Cummings M, Crucetti JB, Stratton H, McNutt L. Given the increasing bias in random digit dialing sampling, could respondent-driven sampling be a practical alternative? Ann Epidemiol 2011; 21(4):272-9.
Levy, P. & Lemeshow, S. (1991). Sampling of populations: Methods and applications.
New York, N.Y.: John Wiley and Sons.
Mackellar, D., Valleroy, L., Karon, G., Lemp, G. and Janssen, R. (1996). The Young
Men's Survey: Methods for estimating HIV seroprevalence and risk factors among young
men who have sex with men. Public Health Reports, 111: 138-144.
Sabin K. (23 May 2011). Comment: Snowball is not the only method for sampling refugees and similar populations. BMC International Health and Human Rights.
| File Type | application/msword |
| Author | sgd8 |
| Last Modified By | Davis, Stephanie I. (ATSDR/DHS/HIBR) |
| File Modified | 2012-07-12 |
| File Created | 2012-07-12 |
© 2026 OMB.report | Privacy Policy