Appendix L3_StudySummary_120802
Appendix L3_StudySummary_120802.doc
Head Start Health Managers Descriptive Study
Appendix L3_StudySummary_120802
OMB: 0970-0415
Head Start Health Managers Descriptive Study Summary
August 2012
Study Overview
The Office of Planning, Research, and Evaluation within the Administration for Children and Families (Department of Health and Human Services) has contracted with the RAND Corporation to conduct the Head Start Health Manager Descriptive Study. The goals of the study are to:
describe the characteristics of health managers and related staff in Early Head Start (EHS) and Head Start (HS) programs1;
identify the current landscape of Head Start health programs and services being offered to children and families;
determine how Head Start health initiatives are prioritized, implemented, and sustained; and
identify the programmatic features and policy levers that exist to support Head Start health services including staffing, environment, and community collaboration.
The purpose of the study is to provide a current snapshot of health-related activities and programming within Head Start programs, to better understand the context in which the Head Start health service area operates, and to identify the current needs of health managers and health staff as they work towards improving the health of Head Start children, parents and staff. The study is intended to provide information on services currently provided and the challenges that Head Start programs face. This study is descriptive and is not designed to capture individual child or family data or program performance standards compliance. Data will be presented in the aggregate and will not be used to make individual program funding decisions or for the designation renewal system (DRS). The study proposes to include the universe of Head Start programs and will include Tribal and American Indian/Alaska Native (AIAN) Head Start programs.
Approach
These study objectives will be accomplished through four proposed data collection components. Data collection will take place once the Office of Management and Budget (OMB) has reviewed and approved the data collection plan and instruments. The goal is to collect data from November to February 2012. These proposed components are:
Head Start Director Survey. Based on contact information available in the Head Start Program Information Reports, the universe of directors for Head Start grantees and delegates—including Tribal and American Indian/Alaska Native grantees—will be invited to complete a short online survey to obtain basic information about the Head Start program and the activities in the health services area. The director will also be asked to provide the name and contact information for the health manager in their program.
Head Start Health Manager Survey. Based on the contact information provided by the director, the universe of health managers for Head Start grantees and delegates will be invited to complete an online survey. This survey questionnaire will take about 75 minutes to complete (including the time needed to gather relevant information) and will include seven modules, summarized in the conceptual framework below.
Head Start Health Manager Interviews. In order to obtain more in-depth information not possible with a structured survey question, a purposive sample of 40 health managers that completed the online survey will be invited to participate in a semi-structured telephone interview to probe more deeply into the topics covered by the online survey. The respondents will be selected to ensure that the sampled respondents capture variation along key Head Start program features.
Head Start Teacher, Family Service Worker, and Home Visitor Interviews. In recognition of the important role played by other Head Start staff in the delivery of the health services area, a purposive sample of 60 teachers, family service workers, and home visitors, nominated by the health managers who complete the semi-structured phone interview, will be invited to participate in a semi-structured telephone interview to learn more about their role in the provision of the health services area. The approach to selecting the sample for this component of the study will be similar to that used for the semi-structured health manager interviews.
An additional component of this project will be the identification and compilation of publicly available geocoded datasets relevant to health. This aspect of the project does not require contact with any individuals or Head Start programs. Given that a major challenge of Head Start Centers is in identifying and establishing linkages with community service providers and other health-related experts, the data will be used by the Office of Planning, Research, and Evaluation and the Office of Head Start to gain a better understanding the geographic distribution of these resources in the communities surrounding Head Start centers, and may help to inform and elucidate some of the findings of the study. Given the utility of the geocoded data for other health-related inquiries and research projects, the Office of Planning, Research, and Evaluation may choose to release the geocoded dataset for use by the general public after the conclusion of the study; however this data will not be linked with the survey or interview data.
Conceptual Framework
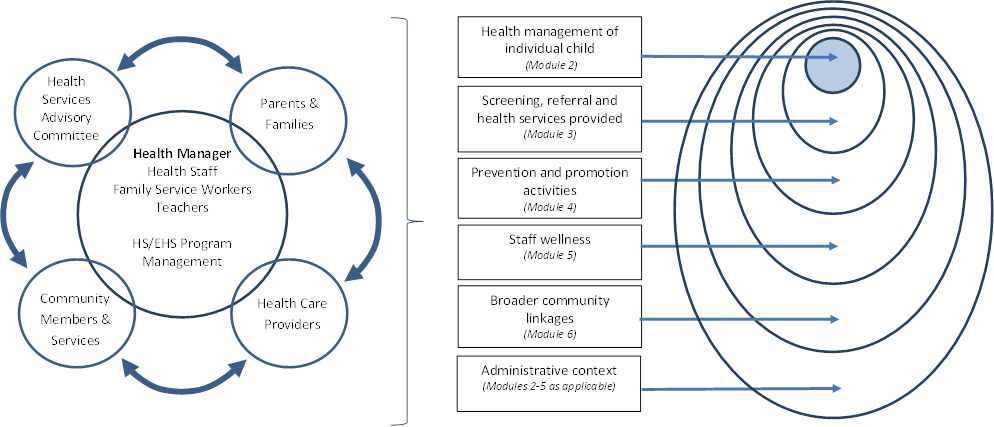
We developed a framework to help conceptualize the vast components and activities of the health service area in Early Head Start and Head Start programs. The framework is presented visually at the end of this letter, and described in more detail below. Although each program is likely to conduct at least some activities related to each level of the framework, we expect the relative emphasis to vary by program based on resources and needs of the population served. To ensure that the Health Managers Descriptive Study captures each of these activities, we have divided the survey into the following seven modules:
Modules 1 and 7 are focused on health managers, the health services advisory committee, staffing model and management structure of the health component, and professional development. Module 7 contains additional questions about the health manager’s background.
Module 2 is focused on understanding the breadth and prevalence of health conditions among the Head Start population, the effort undertaken by Head Start staff in regular management of those conditions, and communication strategies with parents/guardians about specific health concerns of a child.
Module 3 is designed to describe the screening and referral processes of Head Start programs including linkages with health providers in the community and availability of regular sources of care.
Module 4 is focused on Head Start activities in the areas of health promotion and disease prevention/prevention including topic selection and prioritization, implementation challenges, other family health promotion activities and the influence of state or local policies on such activities.
Module 5 describes the Head Start activities to support staff wellness.
Module 6 is designed to capture the network of health-related community partners (beyond medical/oral health providers) that support health activities in Head Start, as well as community engagement strategies undertaken by the program.
The broader administrative context (e.g., follow-up, funding, monitoring) is assessed in Modules 2-5, where applicable. Some of these questions are also included in the Head Start Director’s Survey.
Technical Workgroup and Feedback from Health Managers
In addition to staff within the Office of Head Start and Office of Planning, Research, and Evaluation, we identified nine experts who agreed to serve as a technical workgroup to consult on all aspects of this study. One of our members, Michelle Sarche, has extensive experience working with Tribal populations including serving as a Co-Principal Investigator on the Tribal Research Center on Early Childhood under the Affordable Care Act's (ACA) Maternal, Infant and Early Childhood Home Visiting (MIECHV) Program and the Head Start Act's Head Start and Early Head Start Programs. Dr. Sarche worked with the study staff to ensure proper reviews and approvals for this study (see below for more information). In addition, we asked two health managers in AIAN Head Start programs to review the survey and provide feedback during the design and development stage. We are also currently forming a smaller advisory panel of AIAN representatives who will review and provide feedback on analyses, reporting, and dissemination of findings.
Communication of Findings
Although the majority of study findings will be reported in aggregate across the full range of Head Start programs, the study will also assess how these aspects vary by program characteristics including program option (home versus center-based), urban versus rural location, and culture and language of populations served. The Office of Head Start is interested, for example, to learn more about the particular activities and needs of AIAN Head Start programs. For all reports, all AIAN programs will be aggregated and presented together. No specific program, Tribe, Nation, or location will be identifiable or singled out in reports. Further, the information collected for this study is limited to activities occurring within the Head Start program; we will not be collecting information about broader Tribal populations or activities. The geocoded database that will be compiled will help to provide a context for Early Head Start/Head Start programs, but will not be used to describe a single Tribe, Nation, or location.
Informed Consent and Data Safeguarding
All persons who participate in this data collection, either through the web survey or the semi-structured interviews, will be assured that the personally identifiable information they provide will be kept private to the fullest extent allowed by law. Informed consent from participants will be obtained to ensure that they understand the nature of the research being conducted, the study benefits and any associated risks, and their rights as survey respondents. Respondents who have questions about the consent statement or other aspects of the study will be instructed to call the RAND principal investigators or the administrator of RAND’s Institutional Review Board.
In the case of Head Start directors and health managers who participate in the online survey, the consent script will appear on an introductory screen and the survey will only continue after the respondent has given their consent to participate. For those participating in the semi-structured interviews (e.g., health managers, teachers, family service workers, and home visitors), the consent script will be read as part of the introduction to the survey and the interviewer will not proceed unless oral consent is given.
The study has a Data Safeguarding Plan and standard operating procedures to further ensure the privacy of the information that is collected. For the online survey and semi-structured interviews, RAND will assign a unique data ID to each respondent. Neither names of respondents or HS/EHS grantee name nor any other kinds of identifiers will appear in the survey or interview data used for analysis. For the semi-structured interviews, personal identifiers that could be used to link individuals with their responses will be removed from all interview recording instruments and stored under lock and key at the RAND research team offices. All contact data (including personal identifiers) collected during the study and stored in the Multimode Interviewing Capability (MMICTM) system will be encrypted using a Rijndael 256 standard and stored on a secure server. Personally identifiable information (including names and contact information) and survey data will never be combined into one dataset. RAND will store the raw survey data in a MMICTM database format on a secure server in a directory that is not externally accessible over the web, via shares, or via FTP. It is possible that some survey participants will contact RAND for technical assistance. In this regard, RAND will have access to participant-provided email addresses and names. RAND staff will respond directly to participants when they request assistance with the MMICTM survey but will destroy participant contact information obtained as part of this request as soon as the technical problem has been resolved.
A final dataset will be developed using the above approach that will be accessible only to study staff. At the conclusion of the project, the data will be stripped of any direct or indirect identifiers, including study ID, and will be forwarded to the Office of Planning, Research, and Evaluation. The unidentifiable survey data will be available to the public as a restricted data file. Prior to releasing the dataset, however, a data disclosure analysis to ensure that neither individuals nor programs can be identified will be conducted. The geocoded dataset will not be linked to the survey data when released. RAND will destroy all personally identifiable information within one year of study completion.
The consent procedures and Data Safeguarding Plan have been reviewed and approved by RAND’s Institutional Review Board. Interview and data management procedures that ensure the security of data and privacy of information will be a major part of study staff training.
Human Subjects Protections and Study Review
This study has been reviewed and approved (noted below) or is otherwise in the process of being reviewed by the following committees:
RAND Corporation Institutional Review Board (IRB) [study number: 2011-0874; status is approved: 5/31/2012]
National Indian Health Service IRB (Headquarters) [status is pending]
Each of the 10 regional boards of the Indian Health Service IRB
Aberdeen Area (South Dakota)
Alaska Area
Bemidji Area (Minnesota)
Billings Area (Montana)
Nashville Area (Tennessee)
Navajo Nation
Oklahoma Area
Phoenix Area (Arizona)
Portland Area (Oregon)
Tucson Area (Arizona; approval is referred to National IHS IRB)
Five independent Tribal IRBs [status is pending]
California Rural Indian Health Board
Cherokee Nation
Chickasaw Nation
Choctaw Nation
Rocky Mountain Tribal IRB (Montana and Wyoming)
For More Information
If you have any additional questions or concerns, please feel free to contact the RAND Corporation Principal Investigators or the Federal Project Officer. The consent scripts and survey and interview questions can be accessed via the OMB website: http://www.reginfo.gov/public/do/PRAViewICR?ref_nbr=201203-0970-003.
Laura Hoard, Ph.D., Office of Planning, Research, and Evaluation, Administration for Children and Families, email: Laura.Hoard@acf.hhs.gov
Lynn Karoly, Ph.D., study director, RAND Corporation, email: Lynn_Karoly@rand.org
Laurie Martin, Sc.D., M.P.H., co-study director, RAND Corporation, email: Laurie_Martin@rand.org
Conceptual Framework
KEY STAKEHOLDERS (Modules 1-7) HEALTH COMPONENT FRAMEWORK
1 All EHS/HS grantees must have a health manager who is responsible for managing, facilitating and coordinating health services (including selecting providers and negotiating payments) that promote child health; supervising the nutrition and mental health staff or consultants and other HS staff as they perform health-related duties; and is responsible for maintaining, monitoring, tracking, overseeing and assuring the confidentiality of health records.
| File Type | application/msword |
| Author | RAND Authorized User |
| Last Modified By | DHHS |
| File Modified | 2012-11-07 |
| File Created | 2012-11-07 |
© 2026 OMB.report | Privacy Policy