2900-0727_Justification_A1(v2)
2900-0727_Justification_A1(v2).doc
Survey of Post-Deployment Adjustment Among OEF and OIF Veterans
OMB: 2900-0727
Survey of Post-Deployment Adjustment Among OEF and OIF Veterans
A. JUSTIFICATION
1. Explain the circumstances that make the collection of information necessary. Identify legal or administrative requirements that necessitate the collection of information.
Legal authority for this data collection is found under 38 USC, Part I, Chapter 5, Section 527, authorizing the collection of data that will allow for measurement and evaluation of the Department of Veterans Affairs Programs, the goal of which is improved healthcare for veterans. VHA Directive 2002-049, dated September 11, 2002, authorizes the Veterans Health Administration to provide free medical care and medical services to veterans of Operation Enduring Freedom (OEF) and Operation Iraqi Freedom (OIF) regardless of proof of service connection for a period of two years following discharge from the military. On January 28, 2008, when President Bush signed the National Defense Authorization Act of 2008, this benefit was expanded to five years of free care following discharge. Given the array of mental health issues potentially associated with combat service in the war zone and the recent influx of OEF/OIF service members seeking treatment for these conditions from the Veterans Health Administration under this benefit, the mental healthcare needs of this population are of great interest. Of note, the mental health needs of female OEF/OIF veterans are particularly understudied. This data collection is responsive to several of the priorities identified in “Mapping the Landscape of Deployment Related Adjustment and Mental Disorders,” the final report of a working group convened by the Department of Veterans Affairs, the National Institute of Mental Health and the United States Army Medical Research and Material Command (May 17 – 18, 2006) to identify research needs among the OEF/OIF cohort. Specifically, this data collection will be responsive to the need for increased assessment of co-occurring health conditions associated with deployment to Afghanistan and/or Iraq, the assessment of occupational, family, and social adjustment and functioning, and the assessment of access to VA healthcare, with particular regard to issues of similarities and differences across genders.
2. Indicate how, by whom, and for what purposes the information is to be used; indicate actual use the agency has made of the information received from current collection.
While female service members have long played a critical role in our nation’s military, their numbers and the scope of their contributions have grown substantially in the ongoing wars in Iraq and Afghanistan. Approximately 180,000 women have been deployed in support of OEF and OIF (U.S. Department of Defense, 2007). While women are officially prohibited from serving in direct ground combat positions, women are being exposed to and participating in combat, given the type of warfare employed in the wars in Iraq and Afghanistan (i.e., guerilla warfare with no defined front lines). The experiences of female service members serving in combat support positions in combat-heavy areas are often very similar to the experiences of the all-male infantry. The changing role of women in the military is evidenced by data suggesting that the need for women-specific healthcare within VA is growing. Considering veterans from all eras, women comprise 5% of users of VA healthcare. However, considering only OEF/OIF veterans, women comprise 12% of users of VA healthcare (VHA Office of Public Health and Environmental Hazards, May 2008). Given the potential mental health burden associated with OEF/OIF deployment and the growing role of women in these conflicts, it is imperative that researchers, clinicians and policymakers work together to plan for the unique mental healthcare needs of female veterans returning from war.
Women’s increasing roles in recent combat operations have raised significant questions regarding women’s readjustment following combat. Unfortunately, there is very little research data on the mental health concerns of female OEF/OIF service members.
This data collection is aimed at addressing questions of critical importance for identifying the gender-specific treatment needs of returning OEF and OIF veterans with an emphasis on the needs of female veterans. The survey will incorporate items that focus on issues of particular relevance to female veterans, including war zone experiences (e.g., war zone stressors beyond traditional combat; sexual trauma during deployment) and homecoming experiences that may differentially affect males and females (e.g., relationship and parenting readjustment). In order to most clearly understand female veterans’ treatment needs, women will be over-sampled relative to the proportion of women serving in OEF/OIF in this data collection. Male veterans will also be sampled in order to allow for a direct test of gender differences. True gender differences can not be tested unless data is collected from male and female veterans using an identical study methodology, sampling frame and survey instrument. Comparing the results of a survey of female veterans to the results of a different survey of male veterans will not yield definitive information regarding gender differences between these two groups.
The global goal of identifying the gender-specific treatment needs of returning OEF and OIF veterans subsumes four specific aims as follows:
1.) Identify the frequency, by gender, of combat exposure and military sexual trauma in a sample of military personnel who were deployed to OEF and OIF.
2.) Examine gender differences in post-deployment adjustment and mental health following exposure to combat during OEF and OIF and examine gender differences in post-deployment adjustment and mental health following exposure to military sexual trauma during OEF and OIF.
3.) Identify the additive effects of experiencing both combat and military sexual trauma on post-deployment adjustment and mental health among military personnel from OEF and OIF.
4.) Examine gender differences in VA healthcare usage and satisfaction with VA healthcare among military personnel from OEF and OIF.
3. Describe whether, and to what extent, the collection of information involves the use of automated, electronic, mechanical, or other technological collection techniques or other forms of information technology, e.g. permitting electronic submission of responses, and the basis for the decision for adopting this means of collection. Also describe any consideration of using information technology to reduce burden.
We considered three methodologies for surveying participants: mail survey, phone survey and web-based survey. After comparing the relative advantages and disadvantages of these methods in terms of participants’ convenience, privacy, data validity, logistics and cost, we chose a mail survey approach for this project. Accordingly, improved information technology will not decrease the burden on the public.
A mail survey has several advantages over a phone survey for this type of project. Unlike phone surveys, mail surveys can be completed at participants’ leisure and so are more convenient. They also may offer greater privacy than phone interviews, which in some cases can be overheard. In addition, mail surveys reduce the potential for interviewer bias and may increase participants’ comfort disclosing personal or sensitive information by providing an additional level of perceived anonymity. By following rigorous and recommended procedures (e.g., verified addresses, engaging packaging, repeat mailings), mail surveys can reach a greater proportion of the target audience than phone surveys, which encounter barriers related to unlisted numbers, decreased landline usage, answering machines, caller ID, and quick hang-ups. The main advantages to phone surveys, including lower demands for literacy and automated skip patterns, can be offset by using scales that have been validated with similar populations, carefully formatted instructions about which sections to complete and which to leave blank, and pre-testing the instrument before widespread use – all strategies we are using for the current project.
A mail survey also has several advantages over a web-based survey. First, mail surveys offer increased convenience for members of the target population who do not have easy access to the Internet. Further, it is easier to track who responds to a mail survey in order to ensure that our final sample is balanced on factors like gender. Whereas mail surveys can print an identification number or barcode on the survey, web-based surveys rely on participants accurately keying in an identification number. Web-based surveys may also raise Internet security concerns for some participants, reducing potential response rates. The main advantage of web-based surveys – automated skip patterns – can be addressed by using a well-designed mail survey, using the strategies described above.
4. Describe efforts to identify duplication. Show specifically why any similar information already available cannot be used or modified for use for the purposes described in Item 2 above.
To date, there have been no large-scale investigations of OEF/OIF service members that are aimed at identifying the gender-specific treatment needs of returning veterans or emphasizing the needs of female veterans. The current project is therefore unique in its emphasis on these issues. Existing information collected from OEF/OIF veterans has not oversampled women and so cannot directly test gender differences. Further, existing information has not incorporated survey items that focus on issues of particular relevance to female veterans including military sexual trauma. Existing surveys of mental health and post-deployment readjustment among OEF/OIF service members that have been focused primarily on male service members can inform hypothesis testing for the current investigation but cannot be substituted in any way for the collection of data proposed for this project.
5. If the collection of information impacts small businesses or other small entities, describe any methods used to minimize burden.
The collection of information involves randomly selected individuals in their residences, not small businesses or other small entities.
6. Describe the consequences to Federal program or policy activities if the collection is not conducted or is conducted less frequently as well as any technical or legal obstacles to reducing burden.
This data collection is aimed at addressing questions of critical importance for identifying the gender-specific treatment needs of returning OEF/OIF veterans. If these data are not collected, then the call for gender-specific research identified in “Mapping the Landscape of Deployment Related Adjustment and Mental Disorders” will go unanswered. Despite the growing number of female OEF/OIF service members seeking treatment from VA, existing studies of OEF/OIF veterans focus almost exclusively on male service members. Accordingly, if this information is not collected in a timely fashion, the ability of the Veterans Health Administration to provide empirically derived information about the treatment needs of female OEF/OIF veterans will be impaired; VA would not be responsive to the unique needs of this minority patient population.
7. Explain any special circumstances that would cause an information collection to be conducted more often than quarterly or require respondents to prepare written responses to a collection of information in fewer than 30 days after receipt of it; submit more than an original and two copies of any document; retain records, other than health, medical, government contract, grant-in-aid, or tax records for more than three years; in connection with a statistical survey that is not designed to produce valid and reliable results that can be generalized to the universe of study and require the use of a statistical data classification that has not been reviewed and approved by OMB.
There are no such special circumstances.
8. a. If applicable, provide a copy and identify the date and page number of publication in the Federal Register of the sponsor’s notice, required by 5 CFR 1320.8(d), soliciting comments on the information collection prior to submission to OMB. Summarize public comments received in response to that notice and describe actions taken by the sponsor in responses to these comments. Specifically address comments received on cost and hour burden.
The notice of Proposed Information Collection Activity was published in the Federal Register on November 22, 2011, at pages 72242-72243. We received no comments in response to this notice.
b. Describe efforts to consult with persons outside the agency to obtain their views on the availability of data, frequency of collection, clarity of instructions and recordkeeping, disclosure or reporting format, and on the data elements to be recorded, disclosed or reported. Explain any circumstances which preclude consultation every three years with representatives of those from whom information is to be obtained.
In addition to conducting a thorough review of all documents, both those distributed by the Federal Government and those published in the scientific literature, the Principal Investigators and the investigative team have engaged in numerous discussions with other agencies and experts on post-deployment adjustment and women veterans’ unique healthcare needs. Consultants from the VA’s Environmental Epidemiology Service (EES) have agreed to provide a list frame for sampling, a process of establishing a sampling frame with this population that has been used successfully in the past. The Principal Investigators have also consulted with Education Development Center (EDC), a highly respected not-for-profit research and development firm that has extensive experience in designing and conducting large-scale surveys addressing mental health issues. EDC has been contracted to conduct the data collection. Research staff from the National Center for PTSD who are unfamiliar with the project have reviewed the survey document for clarity of instructions and survey items. Additional outside consultation is conducted with the public through the 60- and 30-day Federal Register notices. There is no evidence that an endeavor of this type—a large-scale survey of OEF/OIF veterans designed to answer questions with particular relevance to women veterans—has been undertaken or is planned by any other research team.
9. Explain any decision to provide any payment or gift to respondents, other than remuneration of contractors or grantees.
Each participant will be sent a $5 cash incentive with the initial survey mailing, with the primary goal of increasing the response rate. Studies have shown that sending an up-front incentive increases the likelihood of response by 61% and that sending a monetary incentive doubles the likelihood of response (Edwards, P., Roberts, I., Clarke, M., DiGuiseppi, C., Pratap, S., Wentz, R., Kwan, I. & Cooper, R. [2007] Methods to increase response rates to postal questionnaires. Cochrane Database of Systematic Reviews, 4). The amount of $5 was chosen because studies have shown that large monetary incentives are not notably more effective than small monetary incentives; as incentives increase, returns begin to diminish (Fox, R.J., Crask, M.R., Kim, J. [1988] Mail survey response rate: A meta-analysis of selected techniques for inducing response. Public Opinion Quarterly, 52, 467-491). It has been demonstrated that potential participants respond more positively to incentives that are conceptualized as small tokens of appreciation than large incentives conceptualized as payment for time. As Dillman (1978) indicates, “the closer the monetary incentive comes to the value of the services performed, the more the transaction tends to move into the realm of economic exchange and the easier it becomes for many people to refuse it” (Dillman, D.A. [1978] Mail and Telephone Surveys: The Total Design Method. New York: John Wiley and Sons).
10. Describe any assurance of confidentiality provided to respondents and the basis for the assurance in statue, regulation, or agency policy.
Information supplied to respondents in the form of a pre-survey letter and introductory comments to the survey will be reviewed and approved by the VA Boston Healthcare System’s Research and Development and Human Studies Committees (Institutional Review Boards) to insure the protection of study participants. Information collected will become part of the system identified as Veteran, Patient, Employee and Volunteer Research and Development Project Records-VA (34VA11), established at 40FR38095 (8/26/75), and amended at 47FR43244 (9/30/82); 49FR36188 (9/14/84); 50FR28867 (7/16/85); 51FR25968 (7/17/86); 55FR42534 (10/19/90); 55FR52934 (12/24/90); and 58FR40852 (7/30/93). The protocol will also be submitted for review to the EDC IRB (Federal Wide Assurance 00000038).
11. Provide additional justification for any questions of a sensitive nature (Information that, with a reasonable degree of medical certainty, is likely to have a serious adverse effect on an individual's mental or physical health if revealed to him or her), such as sexual behavior and attitudes, religious beliefs, and other matters that are commonly considered private; include specific uses to be made of the information, the explanation to be given to persons from whom the information is requested, and any steps to be taken to obtain their consent.
As addressed above in question A.2, one of the primary aims of this investigation is to identify the frequency of military sexual trauma in a sample of military personnel who were deployed to OEF and OIF. Accordingly, respondents will be questioned about experiences of sexual trauma victimization during deployment, including experiences of sexual harassment and sexual assault. The investigative team has significant experience in the successful collection of information from victims of interpersonal violence, has a reputation for collecting such information in a compassionate manner and is sensitive to the possibility that participants may become distressed when recalling experiences of military sexual trauma. Additional information about Education Development Center’s (EDC’s) experience collecting data on sensitive topics and the data collection procedures is provided in B.2 below. As addressed above in question A.10, all information provided to respondents, including the survey instrument, will be reviewed and approved by the VA Boston Healthcare System’s Research and Development and Human Studies Committees (Institutional Review Boards) prior to the initiation of data collection to insure the protection of study participants, as well as the EDC IRB. The cover letter sent to participants with the survey instrument will explain the purpose of the survey and state that all analyses will be performed on aggregate-level data; no individual-level data will be reported. To provide further privacy protection for participants, the investigative team will obtain a Certificate of Confidentiality from the National Institutes of Health (NIH) to protect identifiable research information from forced disclosure. This Certificate of Confidentiality will allow the investigative team to refuse to disclose identifying information on research participants in any civil, criminal, administrative, legislative, or other proceeding, thereby assuring confidentiality and privacy to participants.
12. Estimate of the hour burden of the collection of information:
a. The number of respondents, frequency of responses, annual hour burden, and explanation for each form is reported as follows:
Every effort has been made to minimize the data collection burden. The survey instrument was designed specifically to assess the critical constructs using the smallest number of reliable and valid items. Further, the survey instrument includes “skip-outs” so that respondents will not be required to respond to irrelevant questions. Data collection will involve a mailed survey to randomly selected respondents, with a final target sample size of 4000. The survey instrument requires approximately 20 minutes to complete. Using these values, we compute the estimated burden as follows:
4000 respondents x 20 minutes/60 = 1333.33 total hours of respondent burden.
b. If this request for approval covers more than one form, provide separate hour burden estimates for each form and aggregate the hour burdens in Item 13 of OMB 83-I.
This request covers only one form.
c. Provide estimates of annual cost to respondents for the hour burdens for collections of information. The cost of contracting out or paying outside parties for information collection activities should not be included here. Instead, this cost should be included in Item 14.
The total cost to respondents for completing the survey is $19,999.95.
1333.33 hours x $15/hour = $19,999.95.
13. Provide an estimate of the total annual cost burden to respondents or recordkeepers resulting from the collection of information. (Do not include the cost of any hour burden shown in Items 12 and 14).
a. There is no capital start-up, operation or maintenance costs.
b. Cost estimates are not expected to vary widely. The only cost is that for the time of the respondent.
c. There is no anticipated recordkeeping burden.
14. Provide estimates of annual cost to the Federal Government. Also, provide a description of the method used to estimate cost, which should include quantification of hours, operation expenses (such as equipment, overhead, printing, and support staff), and any other expense that would not have been incurred without this collection of information. Agencies also may aggregate cost estimates from Items 12, 13, and 14 in a single table.
Itemization of all costs entailed in this collection of information is itemized in the budget developed by Rebecca Stoeckle, Project Director, Education Development Center, Inc. This budget, included on the next page, contains detailed itemizations for supplies and equipment, overhead, and personnel and associated fringes.
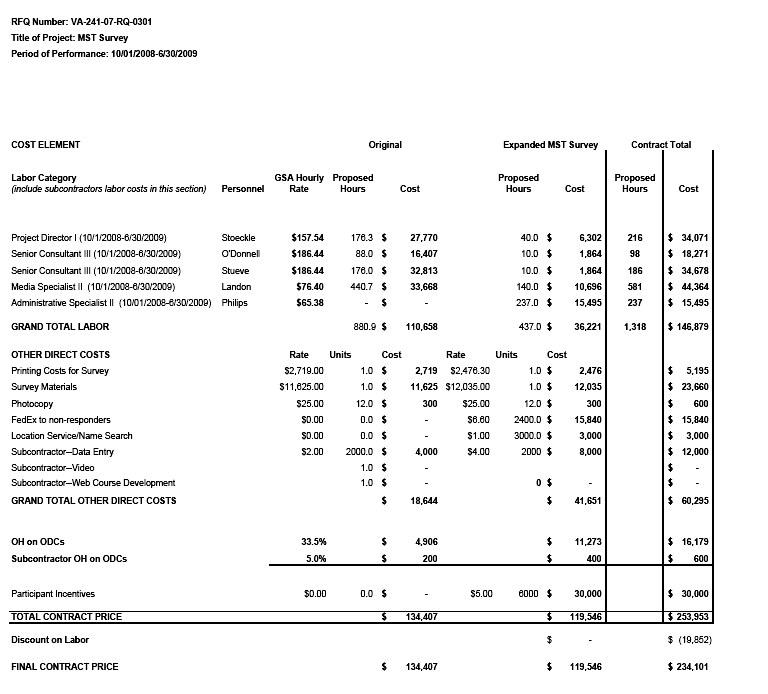
The annual cost to the Federal Government is estimated at $234,101.
15. Explain the reason for any burden hour changes since the last submission.
There is no change in burden.
16. For collections of information whose results will be published, outline plans for tabulation and publication. Address any complex analytical techniques that will be used. Provide the time schedule for the entire project, including beginning and ending dates of the collection of information, completion of report, publication dates, and other actions.
Data will be tabulated and analyzed as follows. First, the data will be cleaned and checked for data entry errors, unusual variable distributions, potential errors due to skip patterns, the extent and patterns of missing data and outliers. For the items that are accompanied by multipoint Likert-type response formats ("strongly disagree"-to-"strongly agree"), the data will be checked by examining frequency distributions and calculating descriptive statistics. For dichotomous items, (e.g., "yes"/"no" responses), the probabilities of endorsement, or the proportion of respondents providing an affirmative response, will be reviewed. Next, we will construct scales using published scoring rubrics (when available) and compute Cronbach’s alpha for internal consistency reliability, where appropriate.
After these initial steps in data checking, cleaning, and reduction, we will begin our analyses. Our first analysis will involve determining the proportion of respondents who were exposed to combat or military sexual trauma, stratified by gender (primary aim 1). Before initiating regression analyses, bivariate coefficients will be calculated between the predictors and outcomes of interest and potential confounders (e.g., age) will be identified. Any variable that is identified as a confounder will be controlled in the regression analyses. Next, to address primary aim two, two hierarchical linear regression analyses will be conducted to examine whether there are gender differences in post-deployment adjustment following exposure to either form of trauma. For the first analysis, gender, combat exposure and the interaction of gender and combat exposure will be entered into a regression analysis, predicting the different measures of post-deployment adjustment. The second analysis will explore gender, military sexual trauma and the interaction of gender and military sexual trauma as predictors of the different measures of post-deployment adjustment. The third primary aim of this study is to explore the additive effect of experiencing both combat and military sexual trauma on post-deployment adjustment. To achieve this specific aim, we will conduct two separate linear regression analyses for males and females to explore these associations in each group. Combat and military sexual trauma exposure will be entered into the regression analyses as well as their interaction to predict post-deployment adjustment. This regression analyses will allow us to calculate the risk due to interdependence of experiencing both combat and military sexual trauma exposure. The risk due to interdependence is used in epidemiology to describe the synergistic risk that occurs when two exposures (e.g., exposure to combat trauma and sexual trauma) are experienced simultaneously. A risk due to interdependence (i.e., in a linear regression model the beta coefficient for the interaction term) that is greater than zero implies that the simultaneous co-occurrence of the risk factors is conferring greater risk than could be expected based on individual risk of either risk factor alone. Finally, to address our last primary aim, hierarchical linear regression analyses will be conducted to examine gender differences in VA healthcare usage and satisfaction.
17. If seeking approval to omit the expiration date for OMB approval of the information collection, explain the reasons that display would be inappropriate.
No exception is requested.
18. Explain each exception to the certification statement identified in Item 19, “Certification for Paperwork Reduction Act Submissions,” of OMB 83-I.
There are no exceptions.
Page
| File Type | application/msword |
| File Title | Bold black = OMB questions |
| Author | vhacobickoa |
| Last Modified By | vhacoharvec |
| File Modified | 2012-03-09 |
| File Created | 2012-03-09 |
© 2026 OMB.report | Privacy Policy