THE SUPPORTING STATEMENT- Revised 6-21-2011 Section A
THE SUPPORTING STATEMENT- Revised 6-21-2011 Section A.doc
Retention Survey of NHSC Clinicians and Alumni/NHSC Site Administrators
OMB: 0915-0341
THE SUPPORTING STATEMENT
EVALUATING RETENTION IN THE NATIONAL HEALTH SERVICE CORPS (NHSC)
CONTENTS
1. Circumstances of Information Collection 1
2. Purpose and Use of Information 1
3. Use of Improved Information Technology 2
4. Efforts to Identify Duplication 2
5. Involvement of Small Entities 2
6. Consequences If Information Collected Less Frequently 3
7. Consistency With the Guidelines in 5 CFR 1320.5(d)(2) 3
8. Consultation Outside the Agency 3
9. Remuneration of Respondents 3
10. Assurance of Confidentiality 4
11. Questions of a Sensitive Nature 4
12. Estimates of Annualized Hour Burden 4
13. Estimates of Annualized Cost Burden to Respondents 5
14. Estimates of Annualized Cost to the Government 5
16. Time Schedule, Publication and Analysis Plans 6
A. Justification
1. Circumstances of Information Collection
The Bureau of Clinician Recruitment and Service (BCRS) within the Health Resources and Service Administration (HRSA) is responsible for managing the National Health Service Corps (NHSC), the government's primary program for placing health care clinicians in locations to care for the underserved. Rural states appealed to Congress and NHSC was authorized under The Emergency Health Personnel Act of 1970 (P.L. 91-263) to improve the delivery of health services to persons living in communities or areas of the United States where health personnel and services are inadequate to meet the health needs of the residents of such communities and areas. Currently, the NHSC is authorized under 42 USC Sec. 254d – 254q-1.
The last study analyzing NHSC retention information is more than ten years old. The purpose of this request is to obtain information to evaluate where the NHSC is today with its ability to retain clinicians within underserved settings and compare it to where it was 12 years ago. This will allow BCRS to recognize the program’s successes, strengthen its weaknesses, and fill in areas where information gaps exist. The evaluation will allow BCRS to develop strategies to enhance the program to run more effectively and to retain even more clinicians to meet the health care needs of rural and urban communities.
This request is to repeat the 1998 survey of NHSC participants, updating the earlier questions to obtain the latest information reflective of changes in the NHSC Program over the past 12 years. Hence, this request is for a revision of the earlier survey. The earlier survey was authorized by OMB and issued control number 0915-0221, that expired 12/31/1998.
2. Purpose and Use of Information
In order for the NHSC to retain health professionals in settings where they provide care for the underserved, it must compete with the private sector and other public sector agencies for these highly valued clinical resources. Comparing the findings of the earlier survey with those of the proposed survey will provide information to the BCRS to optimize the program in terms of: recognizing the factors that influenced NHSC clinicians to remain in their service sites; or if they chose to leave, the factors that influence them to relocate to other practices that provide care to the underserved. The NHSC helps bring committed clinicians into underserved settings for their periods of service obligation; the NHSC’ contribution’s to care in these communities is magnified when its alumni remain beyond their obligations to provide, ideally, decades more care. Having invested in covering the costs of its clinicians’ education, BCRS wishes to determine how optimally to retain them.
The prior survey was used extensively to manage the program. A major evaluation report was prepared1 and subsequent analyses were conducted that allowed NHSC and BCRS staff to manage the program over the past 12 years. However, the size, composition and operations of the Corps have changed substantially, necessitating a new and revised survey. The NHSC’s application process and systems for supporting clinicians as they serve have been updated. Compared to 12 years ago, the Corps now supports many other types of clinicians beyond those in primary care and dentistry, including a variety of mental health professionals and dental hygienists, among others. The broadening of the practitioner types requires survey items that address these professionals’ experiences and perspectives.
The findings of the survey will be used to assess the efforts the Corps has taken, how these efforts have impacted the participants, and the actions the Corps should now take to retain its committed clinicians, and determine how best to strengthen the NHSC.
3. Use of Improved Information Technology
The proposed survey will use a variety of data collection strategies that seek to improve response rates as well as minimize respondent burden. Since the great majority of the clinicians are relatively young and technology-oriented, the survey team proposes to send the initial inquiries via email. The BCRS data system, BMISS, contains the email addresses for the vast majority of current clinicians and many clinicians serving in 2005 and 2006. For clinicians having invalid or missing email addresses, the team will use telephone numbers and mailing addresses to establish contact. A service company will be used to identify contact and email information for hard to reach respondents. The details of the approach are presented in Section B.3.
To minimize respondent burden, respondents will not be asked to describe their communities; instead, this information will be appended from available secondary data, e.g., U.S. Census, DHHS/HRSA/Area Resource File, etc.
4. Efforts to Identify Duplication
As noted, the BCRS manages the NHSC and is current with the literature available. Additionally, the survey team regularly scans the health services research literature and can attest to the fact that since the 1998 survey of the NHSC, no similar broad, national surveys have been conducted of Corps participants.
With regard to duplication of persons to be surveyed, as noted, the BCRS maintains a database containing all current and recent NHSC participants. This database has been searched for duplications, by name, year of birth, address, and profession. This unduplicated list has then been used to subdivide the participants into relevant cohorts.
5. Involvement of Small Entities
All of the persons to be surveyed fall into one of two categories: (1) current and past NHSC clinicians and (2) administrators of current NHSC sites. In the second category, the vast majority of the personnel to be surveyed are administrators of public and community-owned organizations, including Migrant and Community Health Centers, Indian Health Service and tribal health centers, county and city health departments, and prisons. There will be very few privately held entities that will be contacted in this evaluation, as few qualify as NHSC sites. In the first category are individuals who currently are or were employed in and by these same public and community-owned agencies. These individuals are not themselves small or privately held entities and none or virtually none were employed by such agencies. It is also anticipated that none or almost none of the clinicians in the current sample will be owners of practices, but a small minority of recent and remote alumni will be. A few physician, dentist and clinical psychologist NHSC alumni may be owners of small practices, but likely no alumni of other disciplines (e.g., dental hygienists and clinical social workers) would be owners of small entities. It is recognized that some site administrators and some of the surveyed clinicians will be working in small clinics or small group practices. The anticipated burden on these facilities/organizations in these instances is 9 minutes of the site administrator or clinician’s time.
Nevertheless, the survey team has reworded, reduced and streamlined the previously-used instruments to make them more relevant to the participants, thereby minimizing respondent (and facility/organization) burden. In fact, the pre-test of representative respondents has shown a reduction in completion time for each instrument.
With regard to ‘small entities,’ by the very nature of the NHSC, 40% of practice sites are located in small, remote communities. The efforts identified above have recognized the potential burden on these entities, and have worked to remediate the burden.
6. Consequences If Information Collected Less Frequently
Each person must respond only once.
Without this survey, the managers of the program will not have the information needed to strengthen the program or improve retention after program completion.
7. Consistency With the Guidelines in 5 CFR 1320.5(d)(2)
Not applicable, as no special collection or response requirements are to be placed on or required of respondents.
8. Consultation Outside the Agency
The notice required in 5 CFR 1320.8(d) was published in the Federal Register on December 13, 2010 (Vol 75, No. 238, pages 77648/9). A copy of the notice is appended to this submission.
The following is a list of the individuals who reviewed the materials:
Adrain Billings, MD PhD (Family Medicine) 432-887-3434
Dereck Davis, MD (Pediatrics) 601-634-8850
Aaron Huizenga, DO (Family Medicine) 315-482-2094
Alison Bromley, LCSW (617-542-7286)
Lane Hansen, DO (Family Medicine) 208-436-0360
Jonathan Mason, PA (Physician Assistant) 907-443-3404
Courtney Walsh Marsh, CNM (Certified Nurse Midwife) 563-359-6633
Priscilla Durand-Mitchelle, MD (Family Medicine) 251-368-5117
9. Remuneration of Respondents
There are no plans to remunerate respondents for completing the survey instruments.
10. Assurance of Confidentiality
No personal identifiers are to be requested of respondents on the survey instruments.
11. Questions of a Sensitive Nature
No questions of a personally sensitive nature are asked of respondents on the survey instruments. Social security numbers will not be asked or used in any way in this project. Respondents are asked to rate their experiences with NHSC staff and operations and to assess their NHSC experience overall. Some will prefer that the NHSC staff not know that they specifically have given the assessments and comments they provide, i.e., they will want anonymity. Accordingly, the data from this study will not be provided to the NHSC in any form in which the identities of specific respondents can be linked to their comments.
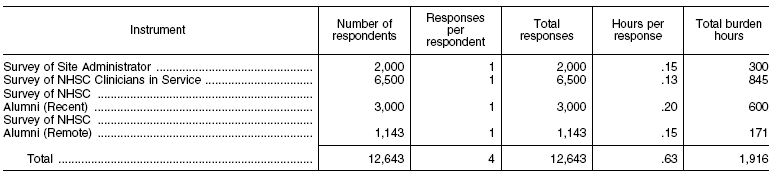
12. Estimates of Annualized Hour Burden
A set of representative respondents was contacted and asked to complete the questionnaires and to record the time taken to complete the instruments. The findings were published in the Federal Register notification, as shown in the table below. As noted earlier, this is a one-time survey; hence one completion constitutes the entire burden on respondents. Also, it should be noted that each respondent falls into one category and therefore, is only requested to complete a single survey instrument.
Administrators are asked in their surveys to estimate the percentages of their patients who are covered under Medicaid, Medicare, are non-English speakers, etc. The questions about insurance coverage and sliding fee scale use are items that administrators routinely track and can readily report. In reporting percentages of non-English speakers, migrant/seasonal farm workers, homeless and substance abuse patients, for the vast majority of administrators there will be no records or files to check, and they can only provide their impressions. To ease their work and time on the survey, we do not want them to take time to look up this information by asking administrators to “estimate” these percentages. Nevertheless, we anticipate that there will be a small number of administrators who will have some information they want to look up in office files and will take an extra 5 to 15 minutes to do so. But as demonstrated in the pilot testing above, we anticipate that the 9 minutes for survey completion for administrators is accurate and will not be much affected by the few administrators who will have data to look on substance abusers, non-English speakers, and such and will go beyond what is requested of them to look up these details.
Since estimating respondents’ time burden reflected in the table above, we have refined our estimates of the numbers of respondents needed to permit stable analyses. These refined estimates of numbers of respondents (see below) are significantly lower than the initial estimates on which the respondent time burden was calculated. The updated numbers below reflect an 80% response rate for each questionnaire/group, which may well be achieved, and our goal is for at least a 75% response rate. (The sample size calculations presented in B.1 of this document are based on a more conservative 65% anticipated response rate, to ensure that even if the target response rate is not met, that respondent group sizes will still be large enough to allow all the study’s most important questions to be answered with enough statistical power.)
Group # surveyed # responding
Survey of 2010 site administrators 500 400
Survey of NHSC clinicians currently in service—Loan Repayment 2,740 2,192
Survey of NHSC clinicians currently in service—Scholars 536 429
Survey of recent NHSC alumni—Loan Repayment 2,393 1,914
Survey of recent NHSC alumni—Scholars 435 348
Survey of remote NHSC alumni (Loan Repayment and Scholars) 860 688
Total 7,464 5,971
13. Estimates of Annualized Cost Burden to Respondents
The one-time respondent burden is estimated to be 1,176 hours. This is based upon surveying 7,464 subjects who yield 5,971 respondents at an average of 0.1575 hours per respondent. While most respondents will complete the surveys in their work setting, we have assumed a nominal hourly rate of $10.00, in accordance with OMB guidance.2 Hence the estimated cost burden is $9404.
14. Estimates of Annualized Cost to the Government
A one-time survey is planned with the cost for contractor support being $290,803.00, inclusive of survey design, sample selection, respondent contact, follow-up, and data assembly. The government personnel costs of federal employees involved in oversight and analysis of the project is estimated to be $25,000.00.
15. Changes in Burden
There are no changes in program burden.
16. Time Schedule, Publication and Analysis Plans
Upon receipt of OMB approval, the survey will be implemented. It is anticipated that survey responses will be received within 75 days of sending the first wave of questionnaires to subjects.
Survey Universe: There is always a concern about correct contact information in surveys, and especially in the case of persons that may have relocated a number of times. In order to ensure a more complete set of contact information and thereby reduce the number of follow-ups, QRS has been in touch with an organization that updates contact information, and can provide email information for many individuals.
As noted in other sections of this document, the BCRS maintains BMISS that contains up-to-date information on current NHSC participants. Less complete information is available for recent participants that have completed their Corps service and may have left their service practices. It will be primarily for these latter cases that both an external service will be used as will internal resources (e.g., telephone follow up).
Survey Design: Section B presents the outline of the proposed stratification approach and the survey design. The design incorporates many of the study questions and recognizes the work performed in the 1998 study. Also, since disciplines participating in the Corps have expanded since 2000, the earlier study will not be useful as a baseline for the newer disciplines. The design also utilizes data sources other than responses to this survey, such as that from the US Census and Area Resource File, thereby providing a richer pool of data for analyses with no added burden to subjects.
For current clinicians, the sampling design will replicate the approach taken in the earlier study, which employed a cross-sectional design. Section B.1 below presents conservative estimates of the cell sizes that are expected for respondent cohorts.
Survey Implementation: Survey instruments will be sent to respondents via email, using web-based instruments for completion. Rejected emails and other indications of bad addresses will be sent to the external address finder service. After this approach has run its course, staff will attempt contacting the targeted respondents by calling the most recent NHSC site that the clinicians worked to determine current addresses, etc. Sometimes we will learn of a state where a clinician moved, which makes on-line licensure files the next source of contact information. On- line rosters of the various national professional associations, e.g., American Academy of Family Medicine, also provide information by which clinicians can be located.
As noted, some respondents may not wish to complete an on-line survey, and these individuals will immediately be sent paper instruments to complete. Close monitoring of the responses, by strata will be important; hence, staff will monitor the responses closely. As strata fall behind expected response rates, staff will immediately follow-up with the non-respondents to promote participation.
Analysis of Responses: Data from the survey will be analyzed and compared for all NHSC participants at each time period, for all participants of the Loan Repayment vs. Scholarship Programs at each time period, for each discipline within each program at each time period, for groups of like-disciplines within each program at each time period, and for rural vs. urban vs. frontier county locations for groups of like disciplines within each program at each time period. As in the previous NHSC evaluation, MDs and DOs will be grouped together within sampling strata for analyses. Various groups will be combined to answer specific questions to meet the particular priorities and concerns of the NHSC. The comparisons of retention and other outcomes for NHSC clinicians in rural vs. urban vs. frontier counties have been explicitly requested by BCRS. Relatively more controlled estimates to identify other correlates of longer retention will be generated through multivariate modeling. Nevertheless, the BCRS’s principal interests are to learn how retention varies for scholars versus loan re-payors, for the various disciplines within each program, and the rural/urban/frontier location of service, and therefore power calculations are based on these group comparisons as the principal analyses. The additional analyses to identify how retention varies with clinicians’ age, race, ethnicity, gender, educational background and experiences, prior practice experience and motivations, as well as with characteristics of practices, will be secondary. Unlike a traditional epidemiological study, the principal purpose of this study is not to generate a full model of the correlates of retention with all “confounding” addressed; these analyses instead are structured to address best the BCRS’ principal need to understand and report the (unadjusted) retention within its various programs, disciplines and location cohorts.
Preliminary Findings: The response rates by strata will be provided on a routine basis to the Project Officer.
Reporting: Staff will discuss the format and audience for the reports that go beyond the Bureau with the Project Officer.
17. Exemption for Display of Expiration Date
No exemption is requested.
18. Certifications
No exceptions are requested as:
The requested survey is necessary for the proper performance of the functions of BCRS, including that the information to be collected will have practical utility;
The survey is not duplicative of information otherwise reasonably accessible to the agency;
Reduces to the extent practicable and appropriate the burden on persons who shall provide information to or for BCRS, including with respect to small entities;
Has been prepared using plain, coherent, and unambiguous terminology and is understandable to those who are to respond;
Is to be implemented in ways consistent and compatible, to the maximum extent practicable, with the existing reporting and recordkeeping practices of those who are to respond;
Indicates for each recordkeeping requirement the length of time persons are required to maintain the records specified;
Informs potential respondents to the information called for under 5 CFR 1320.8(b)(3), including: why the information is being collected; use of the information; burden estimate, nature of response (voluntary, required to obtain or retain a benefit, or mandatory); nature and extent of confidentiality; and need to display currently valid OMB number;
Has been developed by an office that has planned and allocated resources for the efficient and effective management and use of the information to be collected, including the processing of the information in a manner which shall enhance, where appropriate, the utility of the information to agencies and the public;
Uses effective and efficient statistical survey methodology appropriate to the purpose for which the information is to be collected; and
To the maximum extent practicable, uses appropriate information technology to reduce burden and improve data quality, agency efficiency and responsiveness to the public.
1 Konrad, TR, et. al. Evaluation of the Effectiveness of the National Health Service Corps, Contract No. HRSA 240-95-0038, May 31, 2000
2 HRSA PRA Manual - How to Write and Submit Requests for OMB Review and Approval Under the Paperwork Reduction Act and 5 CFR 1320
| File Type | application/msword |
| File Title | THE SUPPORTING STATEMENT |
| Author | Alfred J. Meltzer |
| Last Modified By | Creative Services |
| File Modified | 2011-07-05 |
| File Created | 2011-07-05 |
© 2026 OMB.report | Privacy Policy