MAI Report Instructions
OMB Attachment B Part A MAI Reporting Instructions_Jan 2010 v2.doc
Ryan White CARE Act Title I Minority AIDS Initiative (MAI) Report: Title I Report
MAI Report Instructions
OMB: 0915-0304
Part A Minority AIDS Initiative (MAI):
Program Reporting Instructions
Updated January 11, 2010
PUBLIC BURDEN STATEMENT: An agency may not conduct or sponsor, and a person is not required to respond to a collection of information unless it displays a currently valid OMB Control Number. The OMB Control Number for this project is 0915-0304. Public reporting burden for this collection of information is estimated to be 560 total hours for this activity per reporting year. This estimate includes the time for reviewing instructions, searching existing data sources, gathering and maintaining the data needed, and completing and reviewing the collection of information.
Table of Contents
1 Introduction 3
1.1 Updates and Reminders for Current MAI Web Application Release 3
2 Summary of Part A MAI Reporting Requirements 3
2.2 Overview of Plan and Annual Report Components 3
2.2.2 Narrative Plan Overview 3
2.2.3 Narrative Annual Report Overview 3
2.3 Part A MAI Report Electronic Submission Process 3
3 Detailed instructions for completing the MAI Plan 3
3.1 Start Submission in the EHBs 3
3.2 Data Entry - Complete MAI Report Data Collection Forms 3
3.2.1 Grantee and Funding Information Web Form 3
3.2.2 Service Categories Web Form 3
3.2.3 Race/Ethnicity Service Group Web Form 3
3.2.4 MAI Report Sheet Web Forms 3
3.3 Inserting Web Form Grantee Comments 3
3.4 Upload MAI Annual Plan Narrative 3
3.5 Submit Report for Review 3
3.6 Download MAI Plan for your record 3
4 Detailed Instructions for completing the MAI Annual Report 3
4.1 Start Submission in the EHBs 3
4.2 Complete MAI Report Data Collection Forms 3
4.2.1 Grantee and Funding Information Web Form 3
4.2.2 Service Categories Web Form 3
4.2.3 Race/Ethnicity Service Group Web Form 3
4.2.4 MAI Single Service Web Forms 3
4.2.5 Submitting Plan Revisions 3
4.3 Inserting Web Form Grantee Comments 3
4.4 Upload MAI Year-End Annual Report Narrative 3
4.5 Submit Report for Review 3
4.6 Download MAI Plan for your record 3
5 Selecting client level outcomes 3
6 Appendix I: Client Demographic Data 3
7 Appendix II: Recommended Service Unit Definitions by Service Category……………………3
8 APPENDIX III : Recommended Client Level Outcomes by Service Category 3
1Introduction
The Part A Minority AIDS Initiative (MAI) originated in fiscal year (FY) 1999, when the Congress directed a portion of the Part A supplemental appropriation to be used to address growing disparities in access to care and health outcomes among minority populations disproportionately impacted by the HIV/AIDS epidemic. The MAI continued in this way through FY 2006. Then, under the Ryan White HIV/AIDS Treatment Modernization Act in December 2006, the MAI was codified as a separate, competitive grant program beginning in FY 2007 through FY 2009.
Therefore, following a competitive grant application process in FY 2007, MAI grants were awarded to all 56 Part A eligible metropolitan areas (EMAs) and transitional grant areas (TGAs) for a 3-year project period beginning August 1, 2007 through July 31, 2010. Non-competing continuation grants were awarded for FY 2008 and FY 2009.
However, with the enactment of the Ryan White HIV/AIDS Treatment Extension Act of 2009, the Congress has directed that beginning in FY 2010 that the MAI be changed as follows: a) the grant period is to be "consistent" and "synchronized" with the Part A program application/award schedule, and b) MAI funds will be disbursed on a formula basis. 1 As a distinct component of the Part A Program, the purpose of the MAI remains unchanged, which is to provide targeted resources that are focused on reducing disparities in access and health outcomes in disproportionately impacted minority communities.
Accordingly, FY 2010 MAI funds will be awarded to all EMAs/TGAs based on the distribution of minority populations disproportionately impacted by HIV/AIDS; and these awards will occur at the same time the FY 2010 Part A awards are released, for the 1-year budget period beginning March 1, 2010 and ending February 28, 2011. Grantees were advised in December 2009 to plan and prepare for the initial 5-month overlap in MAI funding that will occur during 2010, since the FY 2009 budget period will not end until July 31, 2010.
The Health Resources and Services Administration (HRSA), HIV/AIDS Bureau (HAB), Division of Service Systems (DSS), which administers the Part A MAI, is issuing these updated MAI Program Reporting Instructions to assist Grantees in preparing and submitting required MAI reports. These include your EMA/TGA’s:
MAI Annual Plan (Plan) for FY 2010; and,
MAI Annual Reports (Annual Reports) for FY 2008, FY 2009, and FY 2010.
The Plan portion of the MAI Report details how funds will be used based on the actual award amount, including the unduplicated number of clients expected to receive each service and planed client-level health outcomes. The Annual Report documents expenditures, the number and demographics of clients served and outcomes achieved.
To
prepare the Plan and Annual Report, Grantees must use
the web-based MAI Report system approved in March 2007
by the Office of Management and Budget, which is accessible through
HRSA’s Electronic Handbooks (EHBs). Both the Plan
and Annual Report must be submitted via the
EHBs by the due date; no extensions are allowed.
The MAI Reporting Instructions are organized as follows.
Summary of Reporting Requirements
Overview of the Electronic Submission Process
An outline of instructions for completing the Annual Report.
Please read the instructions carefully. If you have MAI program-related questions, please contact your DSS Project Officer. If you have questions regarding the Electronic Submission Process, technical assistance is available through the following resources:
Online Help at: https://performance.hrsa.gov/hab/maiApp/help/, which includes a detailed PowerPoint presentation with EHB screen shots.
Contact the HRSA Call Center via email at CallCenter@hrsa.gov or by
telephone at: 1-877-Go4-HRSA (1.877.464.4772)
1.1Updates and Reminders
Below are several important reminders and updates regarding the MAI Report web application, as of the ‘releases’ for September 2009 and January 2010. More detailed information is provided in appropriate sections of these Instructions.
Preparing Submissions: On or before a reporting deadline, data submitted by Grantees in either the Plan or Annual Report Web Forms must be complete, pass HRSA’s internal system validation checks, and be consistent with information provided in the Grantee’s accompanying Plan or Annual Report narrative. Therefore, it is critical for Grantees to begin working on the each submission well before their respective deadlines.
Grantee Delays: Grantees that do not begin a required submission within 15 days of the deadline will receive an email reminder.
System Upgrade – Revising Your MAI Plan: Grantees that receive approval from their Project Officer to revise their Plan during the fiscal year, must submit certain types of revisions via the EHB approximately 30-45 days in advance of the Annual Report submission process. The types of changes requiring a Plan revision include the following.
The addition of an allowable service not previously included in a Grantee’s Plan.
For one or more services already included in a Grantee’s Plan, the addition of one or more target populations that received the service(s).
Note: This new feature was implemented successfully in November 2009, with Grantees requesting these two types of changes in relation to their FY08 Plan.
Reminders for Other Types of Plan Changes:
Reprogramming funds: HRSA grants policy requires Grantees to obtain written approval from your Project Officer before reprogramming funds that involve 20 percent or more of your grant award in any given fiscal year. Such requests should be submitted via email to your assigned Grants Specialist in the Division of Grants Management Operations (the name and email address are listed on the most recent Notice-of-Grant-Award); and a copy of that email should be sent to your Project Officer. However, Grantees are not required to enter this type of budget change in the MAI Report System Plan web-forms.
MAI approved carryover: MAI funds approved for carryover are documented in the MAI Report System when Grantees submit their MAI Annual Reports.
Note: Please keep in mind that carryover requests must be submitted via the EHB’s along with the final Financial Status Reports (FSR), which is due 90 days after the budget period end date. Or, Grantees may indicate on the FSR their intent to submit a request within 30 additional days, in which case the carryover request should be emailed to your Grants Specialist with a copy to your Project Officer. For FY09, a separate MAI FSR is due 90 days after the budget end-date, i.e., on 10/30/2010. For FY 2010 and beyond, Grantees will submit a Part A FSR only, which must include in the remarks section a breakout of Part A expenditures with respect to Formula, Supplemental and MAI funds. The FY 2010 Part A FSR will be due 90 days after the Part A budget end date, i.e. on 6/1/2011.
New Requirement – Narratives: Before uploading a Plan or Annual Report Narrative, you must make sure it is clearly identifiable. To do that, please include a:
“Title Page” specifying the Grantee Name, Grant Number, Fiscal Year and type of submission (i.e. Plan Narrative or Annual Report Narrative);
Header on subsequent pages, with the Grantee Name and Grant Number; and
Footer displaying page numbers, (i.e. "Page 1 of 4").
Recommended Service Unit Definitions: HRSA recommended definitions are provided in drop-down menus for each Part A service category. Grantees must use a recommended definition for each service category. Exceptions will be made only in unusual circumstances, and must be approved by your Grantee.
Recommended Outcome Measures: Grantees must use at least one HRSA recommended measure provided in the service-specific drop-down menus for each service category.
Correcting a Plan or Annual Report Submission: Grantees will receive an email notice generated by the MAI Report System if a submission is returned because it is inconsistent with their Narrative, incomplete, or not in compliance with HRSA Reporting Instructions.
The email will specify the turn-around time for making requested corrections and resubmitting the Plan or Report, usually within 3-5 working days.
Grantees can view the problems specific to each worksheet in comments provided by your Grantee. To view the comments, click the ‘Details of Report Sheet’ link from the Summary Page of your Plan or Annual Report.
Saving a Copy: Grantees may generate and save a copy of their entire Plan or Annual Report submission in either a PDF or Excel format.
1.2Background Information
HRSA recognizes that the MAI is not the sole source of Ryan White Program funds for addressing the unmet HIV/AIDS service needs of minority communities living within an EMA/TGA. Indeed, in order to establish priorities for the use of Part A formula and supplemental funds, each EMA/TGA must take into consideration the size and demographics of the local HIV/AIDS epidemic, paying particular attention to individuals who know their status but are not in care; to disparities in access and services among affected subpopulations and historically underserved communities; and beginning in FY 2010, also the identification of individuals who are unaware of their HIV status.2 Therefore, EMAs/TGAs are expected to use—and do use—Part A Formula and Supplemental funds as well as the MAI to address core medical and support services needs among disproportionately impacted minority communities.
The overarching goal of the MAI is to improve health outcomes by preventing transmission or slowing disease progression for disproportionately impacted communities by:
Getting persons living with HIV disease into care at an earlier stage in their illness,
Assuring access to treatments that are consistent with established standards of care, and
Helping individuals and families to remain in care.
In order for Grantees and HRSA to assess the effectiveness of the MAI Program in achieving these goals, Grantees are required to document client-level health outcomes that are consistent with HRSA guidelines. To do this, all Grantees:
Must ensure that MAI providers document and report client-level health outcomes and the unduplicated numbers of clients receiving each service, broken out by race/ethnicity; and
Must use at least one HRSA recommended outcome measures for each funded service; and all outcome measures used must be consistent with HRSA guidelines.
Grantees are reminded that the MAI Report system is designed so that ONE Web Form only can be used to report required data for each service provided to each racial or ethnic minority community.
If more than one provider/contractor will deliver a particular service to the same racial or ethnic population, then it is critical that the Grantee ensure that each provider tracks and reports at least one and preferably two client-level outcome measures that are the same across all providers delivering a particular service. (The Web Forms provide fields for reporting up to three client-level outcomes.) By doing so, the EMA/TGA also will be better able to assess service quality and effectiveness in achieving planned goals and objectives.
2Summary of Part A MAI Reporting Requirements
At the beginning of each fiscal year, Grantees submit a revised Plan that is based on their MAI award amount. The Plan consists of a descriptive narrative that is uploaded to the MAI Report system via the EHB, as well as quantitative data/information submitted through MAI Report Web Forms. Web Form data includes: MAI allocations for Grantee Administration, Clinical Quality Management, and each planned service; the racial/ethnic communities to be served; and for each community to whom a service is directed, the amount budgeted, number of planned service units, number of clients expected to be served, planned outcomes, and target percentage of clients expected to achieve each outcome.
An Annual Report submitted in the same way at the end of each fiscal year. Grantees use MAI Report Web Forms to document expenditures for each service delivered to each minority community. For each community that received a given service, Grantees report: the unduplicated number of total clients served; unduplicated numbers of women, infants, children and youth served; the total number of service units provided; and the total number of clients that achieved each planned outcome. Grantees also must upload an Annual Report narrative summarizing MAI program accomplishments, challenges and lessons learned.
2.1Reporting Deadlines
Below are the deadlines for Plans and Annual Reports for FY 2008 – FY 2010. Grantees will be able to begin working on each submission in the EHBs at approximately 30 days before each deadline.
Note that there are two Plan submission deadlines: the initial submission due date, and a deadline the next year for submitting any approved Plan revisions that were implemented during that year.
Reports
are submitted to Project Officers for review. If your Project
Officer requires changes or clarification, you will receive an email
notification directing you to make corrections to your initial
submission. You must return to the MAI web application through the
EHB to make the corrections
by the date specified in the
email, which will typically be within 5 work days.
-
Fiscal Year
Deadlines for submission of
MAI PlanDeadlines for submission of MAI Annual Report
2008
Completed (September 30, 2008)
January 29, 2010
2009
Completed (September 30, 2009)
January 28, 2011
2010
June 30, 2010
(To be determined)
2.2Overview of Plan and Annual Report Components
The Plan and Annual Report contain two parts: (1) Web Forms to collect standardized quantitative and qualitative information summarized above, and (2) an accompanying narrative report.
2.2.1Web Forms Overview
The Web Forms collect standardized quantitative and qualitative information describing how funds are budgeted and spent in relation to each service, broken out by the racial and ethnic communities served. For each service directed to each community this includes:
The planned and actual numbers of service units, total unduplicated clients, and unduplicated women, infants, children and youth receiving the service;
Whether services represent a new, continuing or expanded initiative in relation to Part A and MAI funded services provided the previous year (see page 9 for definitions); and
Up to three planned client-level health outcomes, together with the actual results achieved.
2.2.2Plan Narrative Overview
This is a 2 – 4 page description in which Grantees provide:
Title Page: the Grantee Name, Grant Number, Fiscal Year, type of narrative (Plan);
Header on subsequent pages with the Grantee Name and Grant Number;
Footer on subsequent pages showing page numbers (i.e. "Page 1 of 4");
Background information: provide an explanation of the data submitted in the Plan Web Forms;
Summary of the Plan based on the actual award amount that addresses any service-related capacity development activities and the timeline for disbursing funds. In addition, if the EMA/TGA revised any planned services, allocation amounts or target communities after their grant application was submitted, the changes must be highlighted and explained; and the Grantee’s plan and timeline for documenting client-level outcome measures.
2.2.3Annual Report Narrative Overview
This is a 2- 4-page document in which Grantees provide:
Title Page: Grantee Name, Grant Number, Fiscal Year, and type of narrative (Annual Report);
Header on subsequent pages with the Grantee Name and Grant Number;
Footer on subsequent pages showing page numbers (i.e. "Page 1 of 4");
Background information needed to explain data submitted in the Web Forms;
Summary of Accomplishments, including:
Progress toward achieving specific goals and objectives identified in the Grantee’s approved MAI Plan for that fiscal year and in linking MAI services/activities to Part A and other Ryan White Program services;
Achievements in relation to client-level health outcomes and any capacity development or provider-level technical assistance activities;
Summary of challenges or barriers at the provider or Grantee levels, the strategies and/or action-steps implemented to address them, and lessons learned; and
Discussion of MAI technical assistance needs identified by the EMA/TGA.
2.3Part A MAI Report Electronic Submission Process
Part A MAI Grantees are required to submit their MAI Plan and Annual Report electronically each fiscal year. Like the Ryan White Program Data Report (RDR), the MAI Report is a deliverable in HRSA’s Electronic Handbooks (EHBs).
Please visit https://performance.hrsa.gov/hab/ehbdemo/mai/ for instructions about registering in the EHBs and accessing the Part A MAI Plan and/or Annual Report web application.
3Detailed instructions for completing the MAI Plan
3.1Start Submission in the EHBs
Below are the steps for navigating to the MAI Web Application and starting the Plan.
Log in to the EHBs
Click the “View Portfolio” link in the left menu
Locate the Part A Grant in the Grants Portfolio and click the “Open Grant Handbook” link
Click the “Other Submissions” link in the left menu
Locate the Part A MAI Report and click the “Start Submission” link
The MAI Web Application will open in a new window.
Open the Annual Plan In the Action List to access the data entry Web Forms
3.2Data Entry - Complete MAI Report Data Collection Forms
3.2.1Grantee and Funding Information Web Form
Question 1A: Grantee Information
Prepared By: This field will be pre-populated with the name provided in your EHB Profile. Make sure it is up to date. HRSA will contact you if questions arise about information after it has been submitted.
Title: Your job title as the person preparing the report.
E-Mail Address & Telephone: Your e-mail address and phone number will be pre-populated with information in your EHBs Profile. If the information is incorrect, you may update it in this Web Form.
Question 1B: Funding Information
Part A MAI Award: Enter the amount of MAI funds awarded the EMA/TGA for the current fiscal year.
MAI $$ (funds) Approved for Carryover: This field will be disabled in the Plan section of the MAI Report; carryover funds will be reported when you submit your Annual Report.
MAI Funds to be used for Grantee Administration: Enter the amount of the FY MAI award allocated for Grantee administration. The amount cannot exceed ten percent of the total FY MAI Award. Once you enter this value, the percentage will be calculated and displayed.
MAI Funds to be used
for Clinical Quality Management: Enter the amount
of the FY MAI award allocated for clinical quality
management. The amount cannot exceed 5 percent of the total MAI
award. Once you enter this value, the percentage will be calculated
and displayed.
<Click the Next Page Button to Continue>
3.2.2Service Categories Web Form
This form will display all service categories eligible under the Part A MAI Grant Program. Select each service category to be funded during the fiscal year. See Appendix II for a list of allowable Part A Core Medical and Support Service categories.
<Click the Next Page Button to Continue>
3.2.3Race/Ethnicity Service Group Web Form
This form will display, in read-only mode, the services the EMA/TGA selected in the Service Categories Web Form (item above). (If you notice an error, return to the previous Web Form to make corrections.) For each planned service category and race/ethnicity listed, select the level of effort: New, Continuing, or Expanded. Once you select the level of effort, the budget field will become enabled. Enter the budget planned for each service and race/ethnicity combination. See Appendix I for the list of racial and ethnic communities contained on the Plan Web Form.
Definitions:
New: A service planned for the reporting FY that was not provided the previous year to the particular racial/ethnic population using either MAI or Part A funds.
Continuing: A service provided last year to the particular racial/ethnic population using MAI and/or Part A funds that will be continued wholly or in part with MAI funds for the reporting FY.
Expanded: A service provided last year to a racial/ethnic population using MAI and/or Part A funds that will be expanded wholly or in part in the reporting FY using MAI funds in order to serve an expanded geographical area, serve additional clients, or provide additional units of services.
<Click the Next Page Button to Continue>
3.2.4MAI Report Sheet Web Forms
After completing the steps above, your Plan will contain separate Web Forms for each racial and ethnic client group to whom a service/activity will be directed. This does NOT mean that Grantees should prepare an individual Web Form for each service provider. Information from multiple providers delivering the same service to the same ethnic/racial group should be consolidated into a single Web Form. If you need technical assistance with this requirement, contact the HRSA Call Center at 1-877-Go4HRSA.
The information fields described below are required for each service Web Form; i.e. for each service/activity to be provided to each racial/ethnic community.
Service Information: This information will be pre-populated on each service Web Form.
Service or Activity
Ethnicity and Race of Client Group to Receive This Service
New, Continuing or Expanded Effort.
Budget Information: 4.a, b. and c. are pre-populated from information in your Plan in step 3.2.3 above
Planned Budget and Expenditures for This Ethnic/Racial Group
MAI Funds Budgeted for this Service to this Client Group: The amount will be pre-populated.
MAI Carryover from Prior Year Budgeted for this Service to this Group: The carryover field will be disabled, as carryover into the next fiscal year will be reported in your Annual Report.
Total MAI Funds Budgeted for this Service to this Group: This field will be pre-populated with the value entered in item 4a above.
Service Units: Follow the instructions below to enter required information for service units.
Service Unit Name and Definition: Service unit definitions must be consistent with the type of service and HRSA recommended Service Category Definition in Appendix IV. For these reasons and also to enable aggregate analysis of data across Grantees, you must select a HRSA recommended Service Unit Definition from the service-specific drop-down menus provided. (Note: All Service Unit Definitions are listed in Appendix II.) If needed, provide clarification about the definition in a Web Form comment and/or in your Plan Narrative, e.g. with respect to amount or time duration. Examples:
For Outpatient/ Ambulatory Medical Care, 1 unit = 1 Visit is most consistent with the Service Category Definition. In the Plan Narrative or a comment, a Grantee might specify that visits will be documented and billed in 30-minute increments.
For Case Management (non-Medical), 1 unit = 1 Non-medical Case Management Encounter is most consistent with the Service Category Definition; and in the Plan Narrative or a comment, a Grantee might specify they will be documented in 15-minute increments.
If the Grantee thinks local circumstances warrant using a locally established Service Unit Definition, then you must first check with your Project Officer to explain and receive approval. To enter an alternative, local definition:
Choose ‘Other,’ and type the definition in the text box provided; and
Provide an explanation of the rationale for using the local Service Unit Definition, using the Web Form ‘Comment’ function. To insert a comment, click on the ‘Add comment to this report sheet’ link located near the top of the Report Sheet (with the clipboard icon).
Important: Your Project Officer must approve locally established Service Unit Definitions.
Record of Service Units Provided: Enter the number of service units you plan to provide in the reporting FY.
Record of Clients Served: Follow the instructions below to enter required information for clients expected to be served in the coming year.
Planned and Actual Total Number of Clients Served: Use fields 7a – 7e to enter the unduplicated number of clients planned to be served for this ethnic/racial community.
Total Unduplicated Number of Clients: The total number of clients planned for this community.
Total Unduplicated Number of Women: The unduplicated total number of women (25 years or older) planned for this community.
Total Unduplicated Number of Infants: The unduplicated total number of infants (< 2 years) planned for this community.
Total Unduplicated Number of Children: The unduplicated total number of children (2-12 years) planned for this community.
Total Unduplicated Number of Youth: The unduplicated total number of youth (13-24 years) planned for this community.
8A. Planned Client Level Outcome(s): Grantees are expected to use at least one HRSA-recommended, service-specific Client Level Outcome for each MAI-funded service. You may select up to three Planned Client Level Outcomes for each service report sheet Web Form.
Click on the drop-down menu containing HRSA-recommended outcomes measures to select each Planned Client Level Outcome. You MUST choose at least one recommended measure.
Grantees may also select “Other” from the drop-down list to enter a locally defined Client Level Outcome using the text box provided, provided it is consistent with HRSA guidelines.
For each Planned Client Level Outcome chosen, enter the target number/percentage of clients who are expected to achieve the outcome during the year.
Reminders:
The Plan Narrative must include a Title Page identifying the Grantee Name, Grant Number and fiscal year, and specifying that it is a Plan Narrative. On subsequent pages, it must include a header with the Grantee Name and Number and a footer showing page numbers.
Use the Plan Narrative to provide information to explain or describe outcome measures.
Using HRSA-recommended service-specific client level health outcomes will enable Grantees and HRSA to better assess program performance in improving access to care for minority communities, retaining clients in care, and preventing or slowing disease progression. Please refer to Section 5 for more information about selecting outcomes and technical assistance resources; and to Appendix III for a list of HRSA recommended outcome measures.
<Click the SAVE Button to Save Changes>
3.3Inserting Web Form Grantee Comments
Grantees may insert a comment on each Web Form/Report Sheet if needed to provide additional information about the data entered on each service Report Sheet, e.g. with respect to the Service Unit Definition and/or planned Client Level Outcomes. To enter a comment:
Go to the Web Form (Report Sheet) on which you want to insert a comment
Click the icon in the top right corner that says “Add comment to this report sheet”.
Type your comments in the text box provided and then click the Submit button.
Your comment is saved.
To review all comments, both at the MAI Report and Report Sheet levels, click the ‘View Comments’ link on the left menu on any data entry page. All comments will be listed chronically with the most recent comment at the top of the page.
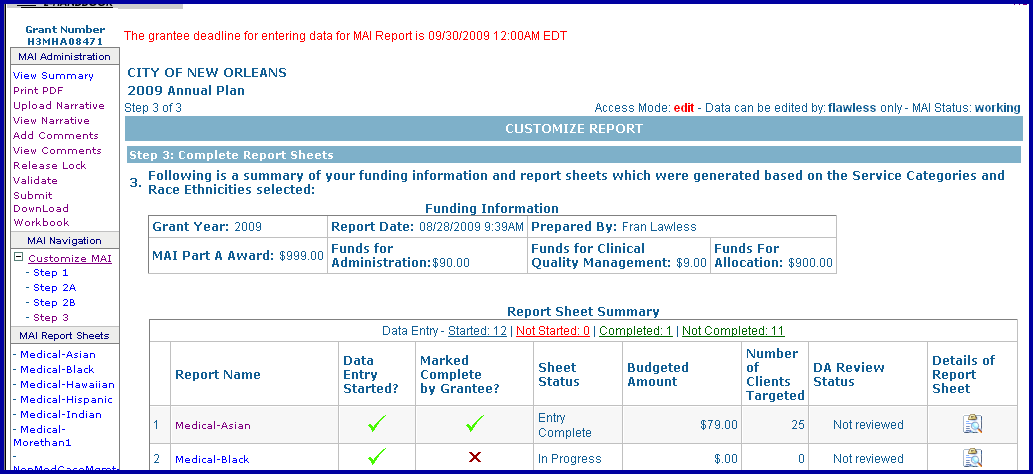
To view Report Sheet-specific comments, go to the Report Sheet Summary page by clicking the View Summary link on the left side of any data entry page.
Click the Comment icon under the Details of Report Sheet column for the report sheet whose comments you want to view. The details of the Report Sheet, including all comments related to this Report Sheet, will be displayed on a pop-up page.
3.4Upload MAI Annual Plan Narrative
Upload the MAI Plan Narrative via the EHB into HRSA’s Part A MAI Report system.
Click the ‘Upload Narrative’ link in the left menu.
Browse to locate and select the Plan Narrative file (Microsoft Word or WordPerfect files only) and then click the Upload File button.
The system will confirm that the file was uploaded successfully by refreshing the upload window and displaying the following confirmation message in red type:
File
uploaded and processed successfully.
Thank you
for uploading Narrative document. Your document has been
successfully uploaded to our database!
3.5Submit Report for Review
Once you have completed all Web Forms for each service provided to each racial/ethnic group, the data entered has passed validation, and you have uploaded your MAI Narrative, you will submit the Part A MAI Annual Plan to HRSA for review. Click the “Submit” button in the left menu to complete this process. You will see a ‘Submission Successful’ confirmation window when you have successfully submitted your Plan.
3.6Download MAI Plan for your record
Grantees may download a copy of their MAI Plan with the information you entered in the Web Forms for your records, in either Microsoft Excel or PDF file format.
To download the MAI Plan in Excel Format:
Click the Download Workbook link in the left menu
Select the type of file you wish to download and save
When the dialogue box opens, click the ‘Save’ option to save the file to your computer. Make sure the filename clearly identifies the content, e.g. Atlanta FY09 MAI Plan, 9-15-09.
To download the MAI Plan in PDF Format:
Click on any data entry page.
Click on the “Print PDF” link on the left navigation bar.
The PDF will appear in a pop-up page. You can save or print this PDF, identifying it as above.
Important: the Microsoft Excel Workbook and PDF files are for your convenience and reference only. They may NOT be used to submit your Plan. Any Plan revisions MUST be entered into the MAI Web Forms and submitted to HRSA via the EHB.
4Detailed Instructions for completing the MAI Annual Report
4.1Start Submission in the EHBs
Steps for navigating to the MAI Web Application and starting the MAI Annual Report:
Log in to the EHBs
Click the “View Portfolio” link in the left menu
Locate the Part A Grant in the Grants Portfolio and click the “Open Grant Handbook” link
Click the “Other Submissions” link in the left menu
Locate the Part A MAI Annual Report for the desired fiscal year and click the “Start Submission” link
The MAI Web Application will open in a new window with your selected annual report open.
4.2Complete MAI Report Data Collection Forms
4.2.1Grantee and Funding Information Web Form
Step 1A: Grantee Information
Prepared By: This field will be pre-populated with the name in your EMA/TGA’s EHB Profile. Make sure that information is correct before you begin. HRSA will contact this individual if questions arise about information after the Annual Report is submitted.
Title: Your job title as the person preparing the report.
E-Mail Address & Telephone: Your e-mail address and phone number will be pre-populated with information in your EHB's Profile. If the information is incorrect, you may update it in this Web Form.
NOTE: Pre-populated data fields in the Annual Report Web Forms are based on the Grantee’s last submitted and approved MAI Plan for the FY being reported. See Section 4.2.5 for instructions on submitting a revised Plan 45 – 60 days before the Annual Report cycle.
Step 1B: Funding Information
Part A MAI Award: The total amount of MAI funds awarded to your EMA for the fiscal year will be will be pre-populated and displayed as read only.
MAI $$ Approved for Carryover: This field is available for the FY08 Annual Report cycle. Grantees that received approval to carry forward FY 2007 MAI funds into FY 2008 must enter the total approved carryover in the field provided.
MAI Funds to be used for Grantee Administration: The amount and percentage of the MAI award budgeted for Grantee administration will be pre-populated and displayed as read only. Enter the amount of Grantee administration funds spent during the reporting FY.
MAI Funds to be used for Clinical Quality Management: The amount and percent of the MAI award budgeted for clinical quality management (CQM) will be pre-populated and displayed as read only. Enter the amount of CQM funds spent during the reporting FY.
4.2.2Service Categories Web Form
Funded services and budgeted amounts are pre-populated in the Annual Report, based on the Grantee’s most recent approved Plan submission for the FY being reported.
4.2.3Race/Ethnicity Service Group Web Form
This form will display in read-only mode, the services the EMA/TGA planned to deliver to each minority group, the amounts budgeted, and whether it was a new, continuing, or expanded service.
4.2.4MAI Single Service Web Forms
The Annual Report contains separate Web Forms for each racial and ethnic client group to whom a service is directed during the reporting FY. Information from multiple providers delivering the same service to the same ethnic/racial group must be consolidated into a single service MAI Web Form, as explained in Section 3.2.4 of these Instructions.
The fields described below are required for each service Web Form; i.e. for each service/activity to be provided to each racial/ethnic community.
Note: If one or more MAI providers served individuals from racial/ethnic communities that were NOT included in the Grantee’s Plan, then the Grantee should: a) insert a Comment on the Web Form for the particular service(s) to identify the other population(s); and b) briefly explain in the Narrative. However, if the EMA/TGA reprioritized their MAI funds during the FY in order to provide a service to an additional minority community, the Grantee should follow directions in Section 4.2.5 for submitting a revised Plan before the Annual Report submission cycle.
Service Information: This information will be pre-populated on each single service Web Form.
Service or Activity
Ethnicity and Race of Client Group to Receive This Service
New, Continuing or Expanded Effort.
Budget & Expenditure Information: Follow the instructions below to enter actual expenditures.
MAI Funds Budgeted for this Service to this Client Group: Pre-populated and in read-only mode.
Carryover Funds for this Service to this Client Group: This field is available for the FY08 Annual Report cycle. Enter the amount of FY 2007 MAI carryover funds used in FY 2008 to support this service. (Enter “0” of no carryover funds were used.)
Total MAI Funds Budgeted for This Service to this Group: Pre-populated based on your Plan and the carryover amount entered above.
Spent: Point and click in the field provided to report actual expenditures for this service.
Service Units: Follow the instructions below to enter required information for service units.
Service Unit Name and Definition: This field will be pre-populated from your Plan.
Record of Service Units Provided: Point and click in the field provided to report the actual total number of service units provided in the reporting FY.
Record of Clients Served: All “planned client” numbers will be pre-populated from your MAI Plan
Planned and Actual Total Number of Clients Served: Use fields 7a – 7e to report the actual total unduplicated number of clients within this ethnic/racial group that received the service.
Total Unduplicated Number of Clients: Report the unduplicated total number of clients in this community that actually received the service.
Total Unduplicated Number of Women: Report the unduplicated total number of women
(ages 25 years or older) in this community that actually received the service.Total Unduplicated Number of Infants: Report the unduplicated total number of infants
(< 2 years) in this community that actually received the service.Total Unduplicated Number of Children: Report the unduplicated total number of children
(2-12 years) in this community that actually received the service.Total Unduplicated Number of Youth: Report the unduplicated total number of youth (13-24 years) in this community that actually received the service.
Planned Client Level Outcome(s): These fields will be pre-populated with information submitted in your MAI Plan for the reporting FY.
Year-End Outcome Results: Follow the instructions below to enter information for outcome results. |
Documented Evidence of Outcomes Achieved:
Narrative Description of Outcomes Achieved: Use the text box fields provided in the Web Form to document results for planned Outcomes #1, # 2 and #3.
Number of Clients Served in Target Population: Report the total number of targeted clients to which each outcome applies. The number entered may not necessarily agree with the “Total Number of Clients Served” reported above, but cannot exceed that number.
Example: The total number of people in an ethnic/racial group that received a service might be 100 clients, but one of the outcomes being reported may pertain only to the 35 women who were served. In that case, you would enter 35 as the “Number of Clients Served in Target Population,” for that particular outcome.Number of Clients Achieving Outcome: Report the number of clients within the target population that achieved each outcome. (To continue the above example targeting women clients: if only 30 of the 35 women served achieved this outcome, then you would enter 30 as the “Number of Clients Achieving Outcome” for this particular outcome.)
Percent: The percentage field is locked and will automatically calculate the percent of clients that achieved each outcome. (For the above example, the calculated percentage would be 30 divided by 35, or 85.7 %.)
4.2.5Submitting Plan Revisions
Each year, approximately 30 – 45 days before the Annual Report submission process is scheduled to begin, Grantees will receive an email asking if their MAI Plan was revised during the FY with regard to the following types of changes.
A service was added that was NOT included in the approved Plan submitted via the EHBs.
A planned service was expanded to serve an additional racial/ethnic population.
Please follow the emailed instructions for submitting a Plan change request in the EHBs.
The deadline for submitting FY08 Plan revisions was 6 PM on December 11, 2009.
Important:
Your MAI Plan data is used to generate your Annual Report Web Forms, so it is critical that you make sure HRSA has correct, up-to-date information. However, HRSA will not be able to accept revisions after the published deadline, because the MAI Report system will be closed for upgrades and system maintenance to prepare for the Annual Report submission cycle.
Plan revisions must be approved by your Project Officer before being implemented, so Grantees must confirm that approval was obtained when submitting a revision request. Grantees are also reminded that you must obtain Project Officer approval before reprogramming 20 percent or more of the MAI grant award.
However, if the only approved Plan changes were to increase or decrease funds budgeted for a planned service(s), you do NOT need to submit a Plan change request for the MAI Report system. These changes are captured when you report your MAI expenditures for each service/population.
4.3Inserting Web Form Grantee Comments
Grantees may insert a comment on each Web Form/Report Sheet if needed to provide additional information about the data entered on each service Report Sheet, e.g. with respect to documented Client Level Outcomes. To enter a comment:
Click the “Add Comment to this Report Sheet” hyperlink located near the upper-right corner of the report sheet (accompanied by a clipboard icon).
Type your comments in the text box provided, and then click on the Submit button.
Your comment will be saved and associated with that report sheet.
To review all comments for all sheets as well as the report click on ‘View Comments’ in the left Navigation Bar. To view comments for a specific sheet only, click on ‘View Summary’ in the left Navigation Bar; then click on the clipboard icon under the “Details” column.
Reminder: Use the Narrative to provide additional
information explaining the outcomes achieved.
4.4Upload MAI Year-End Annual Report Narrative
You will upload the year-end Annual Report Narrative into the Part A MAI Report system to HRSA through the MAI System after you have completed data entry in the Annual Report sheets. Make sure you clearly identify the document on the ‘title page’ (Grantee name, grant number, FY, Annual Report Narrative) and on subsequent pages (header with Grantee name, grant number). Also be sure to insert a footer that includes page numbers (e.g., Page 1 of 4).
Click the ‘Upload Narrative’ link in the left menu
Browse to locate and select the Narrative file (Microsoft Word or WordPerfect files only) and click the ‘Upload Narrative’ button.
The system will confirm that the file was uploaded successfully by refreshing the upload window and displaying the following confirmation message in red type:
File uploaded and processed successfully.
Thank you for uploading Narrative document. You document has been successfully uploaded to our database!
4.5Submit Report for Review
Once you have completed all Web Forms for each service provided to each racial/ethnic group, uploaded your Annual Report Narrative, and the data reported has passed validation, you will submit your MAI Annual Report to HRSA for review. Click the “Submit” button in the left menu to complete this process. You will see a ‘Submission Successful’ confirmation window when you have successfully submitted your Annual Report.


4.6Download MAI Annual Report for your records
You can download a copy of your MAI Annual Report with the information you entered in the Web Forms for your records, in either Microsoft Excel or PDF file format.
To download the MAI Annual Report in Excel Format:
Click the Download Workbook link in the left menu
Select the type of file you wish to download and save
When the dialogue box opens, click the ‘Save’ option to save the file to your computer. Make sure the filename clearly identifies the content, e.g. Atlanta FY08 MAI Annual Report, 1-21-10.
To download the MAI Annual Report in PDF Format:
Click on any data entry page.
Click on the “Print PDF” link on the left navigation bar.
The PDF will appear in a pop-up page. You can save or print this PDF, identifying it as above.
Important: the Microsoft Excel Workbook and PDF files are for your convenience and reference only. They may NOT be used to submit any later changes to your Plan or Annual Report. All revisions MUST be submitted through the MAI System Web Forms.
5Selecting client level outcomes
Each fiscal year since 2000, Part A Grantees have been required to document client-level health outcomes for MAI-funded services provided to each racial/ethnic community. While Grantees have discretion in selecting client level outcomes, those selected must be consistent with published HRSA guidelines for core medical and related support services.
Most EMAs/TGAs have successfully implemented appropriate client-level health outcome measures and indicators that monitor the quality and effectiveness of MAI-funded services. For any that have not, Grantees must work with their providers and Project Officer to ensure that this is accomplished, in order to assess performance with respect to improving access for minority communities, retaining clients in care, and preventing or slowing disease progression.
Appendix III of these Instructions contains a list of recommended outcome indicators for specific core medical and support services that are consistent with HRSA outcomes guidelines and HAB performance measures. Grantees must use at least one recommended client level outcome measure for each MAI funded service.
Grantees also may choose to select one or two locally established client-level outcome measures, by selecting “Other” from the drop-down menu provided and typing in the definition. However, measures that are not client-level or appropriate to the particular service category will not be approved. Additionally, in defining a locally established measure, Grantees should not: (1) combine two or more measures in one text box; or (2) use “Other” to define an outcome measure that is essentially a rewording of an existing standard outcome measure already listed. For example, please select “Increase in the percent of clients with improved or stable CD4 counts” rather than selecting “Other” and typing in a detailed explanation of a specific target or range of CD4 count improvement, as that information is best reported in the Plan Narrative.
Grantees are reminded that the Congress defined support services as services “that are needed for individuals with HIV/AIDS to achieve their medical outcomes;” and medical outcomes were defined as “those outcomes affecting the HIV-related clinical status of an individual with HIV/AIDS.3 Therefore, in selecting outcomes Grantees and funded providers should focus on how the service will enable clients to achieve improved medical outcomes. For example, documenting whether or not MAI-funded Medical Transportation Services will result in a decrease in the number of missed health care appointments and/or an increase in the percentage of clients retained in care.
Technical assistance in selecting HIV/AIDS outcome measures and indicators, including the publication “Measuring Clinical Performance,” is available online through the National Quality Center at: http://www.ihi.org/IHI/Topics/HIVAIDS/TheNationalQualityCenterNQC.htm. You can also call toll-free: 1-888-ASK HRSA. For individualized technical assistance, please contact your Project Officer.
6Appendix I: Client Demographic Data
The MAI
Report collects demographic data elements with respect to
race and ethnicity and age that are consistent with elements in
HRSA’s Ryan White Program Data Report (RWDR). However,
Grantees must submit client-level outcomes data for the MAI
Report, in order to document progress toward achieving the Part
A MAI Grant Program’s mandated purpose of reducing disparities
in access and health outcomes for disproportionately impacted
minority communities.
Therefore, the MAI Report is
structured to collect: 1) data on specific services provided,
clients served and expenditures by race and ethnicity; and 2)
unduplicated client counts. Grantees are responsible for submitting
these required data, and therefore must ensure that MAI-funded
contractors/providers comply in collecting and reporting to the
Grantee all required client-level data elements for each service
that the contractor provides to each racial/ethnic population being
served.
Table I: MAI Report Race and Ethnicity Data |
Asian |
American Indian or Alaskan Native |
Black or African American (not Hispanic) |
Hispanic or Latino(a) |
Native Hawaiian/Other Pacific Islander |
White (not Hispanic) |
More than one race |
Unknown or Unreported |
6.1
Table 2: MAI
Report Gender and Age Data
for Each Service Provided to |
|
Total Number of Clients Served |
Unduplicated Total |
Unduplicated Total Number of Women Served |
25 years and older |
Unduplicated Total Number of Infants Served |
< 2 years |
Unduplicated Total Number of Children Served |
2 to 12 years |
Unduplicated Total Number of Youth Served |
13 to 24 years |
7
Core Medical Services
Outpatient/Ambulatory
Medical Care (health services)
1
unit = 1 Visit
Other
(define):
AIDS
Drug Assistance Program (ADAP)
1
unit = 1 Prescription
Other
(define):
AIDS
Pharmaceutical Assistance (local)
1
unit = 1 Prescription
Other
(define):
Oral
Health Care
1
unit = 1 Oral Health Care Visit
Other
(define):
Early
Intervention Services
1
unit = 1 Visit
1
unit = 1 Client Encounter
Other
(define):
Health
Insurance Premium & Cost Sharing Assistance
1
unit = 1 Month Premium or Cost-Sharing Payment
Other
(define):
Home
Health Care
1
unit = 1 Visit
Other
(define):
Home
and Community-based Health Services
1
unit = 1 Visit
Other
(define):
Hospice
Services
1
unit = 1 Day of Hospice Services
Other
(define):
Mental
Health Services
1
unit = 1 Visit
1
unit = 1 Individual or Group Encounter
Other
(define):
Medical
Nutrition Therapy
1
unit = 1 Visit
Other
(define):
Medical
Case Management
1
unit = 1 Medical Case Management Encounter
Other
(define):
Substance
Abuse Services- Outpatient
1
unit = 1 Visit
1
unit = 1 Individual or Group Encounter
Other
(define):
Appendix II: Recommended Service Unit Definitions by
Service Category
Core Medical Services |
Outpatient/Ambulatory Medical Care (health services) |
1 unit = 1 Visit |
Other (define): |
AIDS Drug Assistance Program (ADAP) |
1 unit = 1 Prescription |
Other (define): |
AIDS Pharmaceutical Assistance (local) |
1 unit = 1 Prescription |
Other (define): |
Oral Health Care |
1 unit = 1 Oral Health Care Visit |
Other (define): |
Early Intervention Services |
1 unit = 1 Visit |
1 unit = 1 Client Encounter |
Other (define): |
Health Insurance Premium & Cost Sharing Assistance |
1 unit = 1 Month Premium or Cost-Sharing Payment |
Other (define): |
Home Health Care |
1 unit = 1 Visit |
Other (define): |
Home and Community-based Health Services |
1 unit = 1 Visit |
Other (define): |
Hospice Services |
1 unit = 1 Day of Hospice Services |
Other (define): |
Mental Health Services |
1 unit = 1 Visit |
1 unit = 1 Individual or Group Encounter |
Other (define): |
Medical Nutrition Therapy |
1 unit = 1 Visit |
Other (define): |
Medical Case Management |
1 unit = 1 Medical Case Management Encounter |
Other (define): |
Substance Abuse Services- Outpatient |
1 unit = 1 Visit |
1 unit = 1 Individual or Group Encounter |
Other (define): |
Support Services |
Case Management (non-Medical) |
1 unit = 1 Non-medical Case Management Encounter |
Other (define): |
Child Care Services |
1 unit = 1 Child Care Session |
Other (define): |
Emergency Financial Assistance |
1 unit = 1 Assistance Voucher or Assistance Payment |
Other (define): |
Food Bank/Home Delivered Meals |
1 unit = 1 Meal or 1 Bag of Groceries |
Other (define): |
Health Education/Risk Reduction |
1 unit = 1 Individual or Group Encounter |
Other (define): |
Housing Services |
1 unit = 1 Day of Housing |
1 unit = 1 Housing Related Service |
Other (define): |
Legal Services |
1 unit = 1 Client Encounter |
1 unit = 1 Individual or Group Encounter |
Other (define): |
Linguistic Services |
1 unit = 1 Individual or Group Encounter |
Other (define): |
Medical Transportation Services |
1 unit = 1 one-way trip or medical transportation voucher |
Other (define): |
Outreach Services |
1 unit = 1 Individual or Group Encounter |
1 unit = 1 Client Contact |
Other (define): |
Psychosocial Support Services |
1 unit = 1 Individual or Group Encounter |
Other (define): |
Referral to Health Care/Supportive Services |
1 unit = 1 Client Contact |
Other (define): |
|
Rehabilitation Services |
1 unit = 1 Visit |
Other (define): |
Respite Care |
1 unit = 1 Session of Respite Care |
Other (define): |
Substance Abuse- Residential Services |
1 unit = 1 Day of Residential Substance Abuse Treatment Services |
Other (define): |
Treatment Adherence Services |
1 unit = 1 Individual or Group Encounter |
Other (define): |
8APPENDIX III: Recommended Client Level Outcomes by Service Category
The table below provides examples of recommended HIV/AIDS client-level outcome measures that are consistent with published HRSA guidelines referenced in these Reporting Instructions. The services are grouped into Core Medical and Support Services that are allowed under the Part A Ryan White Program, including the Minority AIDS Initiative. To ensure the appropriateness of MAI outcomes measures and improve consistency across EMAs/TGAs in documenting progress toward slowing/preventing disease progression, Grantees are expected and strongly encouraged to consider using at least one recommended outcome for each funded MAI funded service.
Part A MAI Standard Outcome Measures for Core Medical Services |
Outpatient/Ambulatory Medical Care (health services) |
Increase the percentage of new clients whose initial medical evaluation meets age and gender-specific PHS Clinical Guidelines for HIV/AIDS |
Increase in the percentage of clients with improved or stable CD4 counts |
Increase in the percentage of clients with improved or stable viral load test results |
Increase in the percentage of women clients that are receiving annual Pap smear |
Decrease in the percentage of clients served experiencing an AIDS-defining opportunistic disease |
Decrease in the percentage of clients served who experience an HIV/AIDS-related hospitalization |
AIDS Drug Assistance Program (ADAP) |
Increase in the number of clients with access to prescribed HIV/AIDS medications |
Increase in the percentage of clients with access to prescribed HIV/AIDS medications consistent with PHS Treatment Guidelines |
Decrease in the percentage of clients served experiencing an AIDS-defining opportunistic disease |
Increase in the percentage of clients with improved or stable CD4 counts |
Increase in the percentage of clients with improved or stable viral load test results |
AIDS Pharmaceutical Assistance (local) |
Increase in the number of clients with access to prescribed HIV/AIDS medications |
Increase in the percentage of minority clients with access to prescribed HIV/AIDS medications consistent with PHS Treatment Guidelines |
Decrease in the percentage of clients served experiencing an AIDS-defining opportunistic disease |
Increase in the percentage of clients with improved or stable CD4 counts |
Increase in the percentage of clients with improved or stable viral load test results |
Oral Health Care |
Increase in the percentage of clients who are accessing oral health/dental services |
Increase in the percentage of clients who are able to maintain good nutritional status following treatment of oral pain and oral disease |
Decrease in the percentage of clients served experiencing an AIDS-defining opportunistic disease |
Early Intervention Services |
Increase in the number and percent of PLWH who know their HIV status |
Among PLWH who know their status, an increased percentage are successfully linked to HIV/AIDS medical care |
An increased percentage of clients who know their HIV status will remain in care |
Increase in the percentage of clients with improved or stable CD4 counts |
Increase in the percentage of clients with improved or stable viral load test results |
Health Insurance Premium & Cost Sharing Assistance |
Increase in the percentage of clients who maintain their health insurance |
Increase in the percentage of clients who are accessing health insurance including prescription medication coverage |
Increase in the percentage of clients with improved or stable CD4 counts |
Increase in the percentage of clients with improved or stable viral load test results |
Home Health Care |
Increase in the percentage of clients who are receiving this service based on a written plan of care established by an appropriate and licensed health care team |
Decrease in the percentage of clients served experiencing an HIV/AIDS-related hospitalization |
Decrease in the percentage of clients served experiencing an HIV/AIDS- related emergency room visit |
Increase in the percentage of clients with improved or stable CD4 counts |
Increase in the percentage of clients with improved or stable viral load test results |
Home and Community-based Health Services |
Increase in the percentage of clients who are receiving this service based on a written plan of care established by an appropriate and licensed health care team |
Decrease in the percentage of clients served experiencing an HIV/AIDS- related emergency room visit |
Decrease in the percentage of clients served experiencing an HIV/AIDS-related hospitalization |
Increase in the percentage of clients with improved or stable CD4 counts |
Increase in the percentage of clients with improved or stable viral load test results |
Hospice Services |
Increase in the percentage of clients able to remain at home while receiving appropriate medical and related supportive services at the end stage of illness |
Increase in the percentage of clients at end stage who are medically evaluated for AIDS-related salvage therapies consistent with PHS Guidelines |
Mental Health Services |
Increase in the percentage of clients with mental health condition/illness who are successfully linked to licensed mental health services |
Increase in the percentage of clients with mental health condition/illness who comply with or complete their mental health treatment plan. |
Increase in the percentage of clients with mental health conditions who are remaining in HIV/AIDS medical care |
Increase in the percentage of clients with improved or stable CD4 counts |
Increase in the percentage of clients with improved or stable viral load test results |
Medical Nutrition Therapy |
Increase in the percentage of clients counseled on dietary issues |
Decrease in the percentage of clients with wasting syndrome |
Increase in the percentage of clients maintaining healthy weight status |
Increase in the percentage of clients with diagnosed nutritional needs who are accessing necessary nutritional supplements |
Increase in the percentage of clients with improved or stable CD4 counts |
Increase in the percentage of clients with improved or stable viral load test results |
Medical Case Management |
Among new clients who are out of care, an increase in the percentage who receive an initial HIV/AIDS medical evaluation within 2 weeks of completing intake. |
Increase in the percentage of client files containing a case management plan consistent with established standards that includes a medical treatment plan |
Increase in the percentage of clients who receive treatment adherence counseling |
Among clients receiving antiretroviral (ARV) medications, an increase in the percentage of clients who adhere to their prescribed medication regimen |
Increase in the percentage of clients with improved or stable CD4 counts |
Increase in the percentage of clients with improved or stable viral load test results |
Increase in the percentage of clients retained in care |
Decrease in the percentage of clients lost to follow-up |
Among clients whose substance abuse and/or mental health evaluation indicates a service need, an increased percentage receive appropriate follow-up. |
Substance Abuse Services- Outpatient |
Increase in the percentage of clients with a substance abuse diagnosis who enter and complete an outpatient substance abuse treatment program |
Increase in the percent of clients with addictions who remain in medical care |
Decrease in the percentage of clients experiencing AIDS-defining opportunistic disease |
Increase in the percentage of clients retained in care |
Increase in the percentage of clients with improved or stable CD4 counts |
Increase in the percentage of clients with improved or stable viral load test results |
Part A MAI Standard Outcome Measures for Support Service Categories |
Case Management (non-Medical) |
Increase in the percentage of clients receiving advice and assistance in obtaining medical, social, community, legal, financial, and other needed services |
Increase in the percentage of clients retained in care |
Increase in the percentage of clients with improved or stable CD4 counts |
Increase in the percentage of clients with improved or stable viral load test results |
Child Care Services |
Increase in the percentage of HIV+ clients with children who keep medical or other care-related appointments |
Increase in the percentage of clients retained in care |
Emergency Financial Assistance |
Increase in the percentage of clients retained in care |
Food Bank/Home Delivered Meals |
Increase in the percentage of clients receiving food/meals needed to help meet their daily living needs |
Increase in the percentage of clients maintaining healthy weight status |
Increase in the percentage of clients adherent to treatment regimens that require medications taken with food |
Increase in the percentage of clients retained in care |
Health Education/Risk Reduction |
Increase in the percentage of clients who are educated about HIV transmission and how to reduce the risk of transmission. |
Increase in the percentage of clients who are educated about available medical, psycho-social support services |
Increase in the percentage of clients retained in care |
Housing Services |
Increase in the percentage of clients in stable housing |
Increase in the percentage of clients retained in care |
|
Legal Services |
Increase in the percentage of clients receiving powers of attorney, medical directives, and interventions necessary to ensure access to eligible benefits |
Increase in the percentage of clients retained in care |
Linguistic Services |
Increase in the percentage of clients receiving interpretation and translation services needed to support the provision of HIV/AIDS health care and related support service |
Increase in the percentage of clients retained in care |
Medical Transportation Services |
Decrease in the number of missed health care appointments |
Increase in the percentage of clients retained in care |
Outreach Services |
Increase in the number of clients who know their HIV status |
Increase in the number of clients entering care at an earlier stage of illness |
Psychosocial Support Services |
Increase in the percentage of clients with identified HIV support group and caregiver support group needs are receiving these services |
Among clients receiving psychosocial support services, an increased percentage are being retained in care |
Referral to Health Care/Supportive Services |
Increase in the percentage of clients referred to appropriate HIV/AIDS health care and supportive services |
Increase in the percentage of clients linked to HIV/AIDS health care and supportive services as measured by kept initial appointments |
Increase the percentage of clients retained in care |
Rehabilitation Services |
Increase in the percentage of clients receiving rehabilitation services from a licensed or authorized provider in accordance with an individualized plan of care |
Increase in the percentage of clients that are able to perform activities of daily living and self-care |
Respite Care |
Among caregivers receiving respite care services, an increase in the percentage able to continue serving as the primary caregiver |
Increase in the percentage of HIV+ clients being cared for at home |
Decrease in the percentage of clients requiring institutional care |
Substance Abuse- Residential Services |
Increase in the percentage of clients with substance abuse diagnosis who enter and complete an inpatient substance abuse treatment program |
Increase in the percentage of clients retained in care |
Increase in the percentage of clients with improved or stable CD4 counts |
Increase in the percentage of clients with improved or stable viral load test results |
Decrease in the percentage of clients experiencing AIDS-defining opportunistic disease |
Decrease in the percentage of clients experiencing an HIV/AIDS related emergency room visit |
Increase in the percentage of HIV+ clients with substance abuse diagnosis who are receiving medical care |
Treatment Adherence Services |
Increase in the percentage of clients who receive treatment adherence counseling |
Among clients receiving antiretroviral (ARV) medications, an increase in the percentage of clients who adhere to their prescribed medication regimen |
Increase in the percentage of clients with improved or stable CD4 counts |
Increase in the percentage of clients with improved or stable viral load test results |
Increase the percentage of clients retained in care |
1 Section 2693 (a), (b). (c), and (d)(1) of the Public Health Service (PHS) Act
2 Section 2602(b)(4)(A)(B)(C) and (D) of the PHS Act
3 Sections 2604(d)1 and (d)(2) of the PHS Act
| File Type | application/msword |
| File Title | Part A Minority AIDS Initiative (MAI): |
| Subject | Updated Report Instructions |
| Author | M.Wieland/HRSA & C.Kwon/SAIC |
| Last Modified By | Hrsa |
| File Modified | 2010-07-07 |
| File Created | 2010-07-07 |
© 2026 OMB.report | Privacy Policy