Form VA Form 10-0472 VA Form 10-0472 MOVE! Weight Management Program for Veterans, Survey of
MOVE! Weight Management Program for Veterans, Survey of Patient Experiences
MOVE_Patient_Survey(v3)
MOVE! Weight Management Program for Veterans, Survey of Patient Experiences
OMB: 2900-0753
OMB
2900-XXXX
Estimated Burden: 15 minutes
MOVE!
Weight
Management Program for Veterans
Survey of Patient Experiences
Point of Contact:
Leila
C. Kahwati, MD MPH
Deputy
Chief Consultant for Preventive Medicine
National Center for Health Promotion and Disease Prevention
Office of Patient Care Services
Veterans Health Administration
(919)383-7874 Ext 251
The
Paperwork Reduction Act of 1995
requires us to notify you that this information collection is in
accordance with the clearance requirements of section 3507 of this
Act. The public reporting burden for this collection of information
is estimated to average 15 minutes per response, including the time
for reviewing instructions, searching existing data sources,
gathering and maintaining the data needed, and completing and
reviewing the collection of information. No person will be
penalized for failing to furnish this information if it does not
display a currently valid OMB control number. Response to this
survey is voluntary and failure to furnish this information will
have no effect on any of your applications for benefits. The
information requested on this form is solicited under the authority
of Title 38, U.S.C., Part I, Chapter 5, Section 527 that authorizes
the collection of data that will allow measurement and evaluation of
the Department of Veterans Affairs Programs. The purpose(s) for
collecting the information is to provide information for a research
study being conducted by the Department of Veterans Affairs related
to how patients experience the MOVE! Weight Management Program for
Veterans.
Thank you for agreeing to complete this survey about your experience with the MOVE! Weight Management Program for Veterans. We are interested in learning about your honest experiences with the treatment you received, whatever they may be. There are no right or wrong answers.
We realize that you may have received MOVE! Weight Management care at more than one VA location. However, it is important that you answer the questions in this survey based on your experience overall.
Most of the questions on this survey are about your experience during treatment, your physical activity or diet choices. You are free to skip any questions you do not want to answer, but we hope you will answer them all because we believe they are all important. Your answers will help us make MOVE! more effective and helpful for those in the future.
If you have not received MOVE! Weight Management treatment at a VA medical center or clinic and believe that you may have received this survey in error, please check this box and return the survey in the enclosed envelope.
Instructions:
For each question on the survey check the box or circle the number that best describes your experience. There are some questions, however, where you can check multiple boxes to tell us about your experience.
For items with a box, mark your selection(s) like this:
0 |
1 |
2 |
3 |
4 |
5 |

The first section of this survey asks about your current physical activity, eating habits, health, and neighborhood environment.
Physical Activities are activities where you move and increase your heart rate above its resting rate, whether you do them for pleasure, work, or transportation. The following questions ask about the amount and intensity of physical activity you usually do.
Examples of physical activity intensity levels:
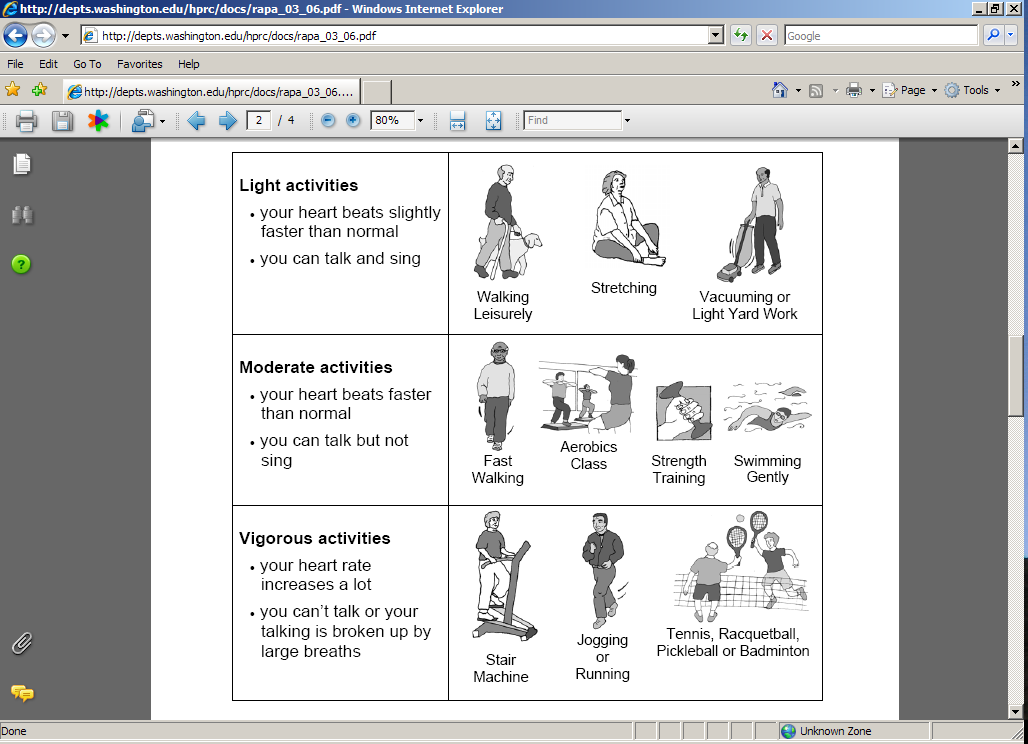
1. How physically active are you? (Check one box for each statement)
|
Does this accurately describe you? |
|
|
Yes |
No |
a) I rarely or never do physical activities. |
|
|
b) I do some light or moderate physical activities, but not every week. |
|
|
c) I do some light physical activity every week. |
|
|
d) I do moderate physical activities every week, but less than 30 minutes a day or 5 days per week. |
|
|
e) I do vigorous physical activities every week, but less than 20 minutes a day or 3 days a week. |
|
|
f) I do 30 minutes or more a day of moderate physical activities, 5 or more days a week. |
|
|
g) I do 20 minutes or more a day of vigorous physical activities, 3 or more days a week. |
|
|
h) I do activities to increase muscle strength, such as lifting weights or calisthenics, once a week or more. |
|
|
i) I do activities to improve flexibility, such as stretching or yoga, once a week or more. |
|
|
2. Circle the number of times in one week you typically …
|
Number of Times in One Week |
||||||||
a) Eat restaurant or fast food (for example, Chili's, McDonalds, Burger King, etc). |
0 |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
>7 |
b) Eat breakfast in the morning. |
0 |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
>7 |
c) Skip meals |
0 |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
>7 |
3. Circle the number of times in one day you typically eat or drink…
|
Number of Times in One Day |
||||||||
a) Juice drinks (for example, orange juice, apple juice, Sunny Delight, Hi-C, Juicy Juice). |
0 |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
>7 |
b) Cans or bottles of non-diet soda pop (for example, Coke, Pepsi, Sprite). |
0 |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
>7 |
c) Vegetables (for example, broccoli, spinach, greens, salad, etc). |
0 |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
>7 |
d) Fruit (for example, an apple, an orange, a hand full of grapes, etc). |
0 |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
>7 |
4. How often do you……. (Check one box for each statement)
|
Less than 1 time per month |
About 1-2 times/month |
About 1-2 times/week |
Daily |
a) Weigh yourself on a scale? |
|
|
|
|
b) Keep track of what you eat and drink in a journal or log? |
|
|
|
|
c) Keep track of your physical activity in a journal or log? |
|
|
|
|
5. Tell us about your surroundings. (Check one box for each statement)
|
Not at all |
Slightly |
Quite |
Extremely |
|
a) Rate your neighborhood as a pleasant place to be physically active. |
|
|
|
|
|
b) How safe from crime do you feel while you are walking in your neighborhood? |
|
|
|
|
|
|
Strongly disagree |
Disagree |
Agree |
Strongly agree |
|
c) There are many destinations within walking distance from my home. |
|
|
|
|
|
d) There are sidewalks on most streets in my community. |
|
|
|
|
|
e) A large selection of affordable fruits and vegetables is available in my neighborhood. |
|
|
|
|
|
f) A large selection of affordable low-calorie products is available in my neighborhood. |
|
|
|
|
|
6. For me, lack of access to adequate food shopping is: (Check one box)
A very serious problem
A somewhat serious problem
A minor problem
Not really a problem
7. In general, would you say your health is:
Excellent
Very good
Good
Fair
Poor
|
Days |
Don’t know |
8. Now, thinking about your physical health, which includes physical illness and injury, for how many days during the past 30 days was your physical health NOT good? |
_____ days |
|
9. Now, thinking about your mental health, which includes stress, depression, and problems with emotions, for how many days during the past 30 days was your mental health NOT good? |
_____ days |
|
10. During the past 30 days, for about how many days did poor physical or mental health keep you from doing your usual activities, such as self-care, work, or recreation? |
_____ days |
|
The second section of this survey asks about your experiences with weight management (MOVE!) treatment.
11. When I received weight management (MOVE!) treatment, I was:
(Check one box for each statement)
|
Almost never |
Generally not |
Sometimes |
Most of the time |
Almost always |
a) Satisfied that my weight management care was well organized. |
|
|
|
|
|
b) Helped to set specific goals to change my eating habits. |
|
|
|
|
|
c) Helped to set specific goals to increase my physical activity. |
|
|
|
|
|
d) Asked for my ideas to make a weight management treatment plan. |
|
|
|
|
|
e) Helped to make a weight management treatment plan that I could do in my daily life. |
|
|
|
|
|
f) Provided with easy to understand instructions to help manage my weight. |
|
|
|
|
|
g) Treated with respect. |
|
|
|
|
|
h) Satisfied with the changes I made in my weight. |
|
|
|
|
|
12. I used the following as part of my weight management (MOVE!) treatment plan:
(Check one box for each statement)
|
Never |
Rarely |
Sometimes |
Often |
Almost always |
a) A pedometer to track my steps |
|
|
|
|
|
b) MOVE! Patient Handouts (Information Sheets) |
|
|
|
|
|
c) MOVE! Internet Web Site |
|
|
|
|
|
|
13. When I received weight management (MOVE!) treatment……….(Check one box for each statement)
|
Strongly disagree |
Somewhat disagree |
Neither agree nor disagree |
Somewhat agree |
Strongly agree |
Not applicable |
a) Staff helped me keep track of the progress I made towards my personal goals. |
|
|
|
|
|
|
b) Staff listened and responded to my cultural experiences, interests, and concerns. |
|
|
|
|
|
|
c) The clinic waiting areas, exam rooms, and group treatment rooms had comfortable furniture that I could sit or lie on. |
|
|
|
|
|
|
d) Weight management treatment was provided in clinic areas that were sufficiently private. |
|
|
|
|
|
|
e) Weight management treatment was provided at times and days that were convenient for me. |
|
|
|
|
|
|
f) Weight management treatment was provided at a location that was convenient for me. |
|
|
|
|
|
|
g) Friends or family assisted me in shopping for healthy foods. |
|
|
|
|
|
|
h) Friends or family helped me prepare healthy meals. |
|
|
|
|
|
|
i) Friends or family helped me be physically active. |
|
|
|
|
|
|
j) Friends or family encouraged me to eat healthy or stay physically active. |
|
|
|
|
|
|
14. Are you currently participating in weight management (MOVE!) treatment? (Check one box)
Yes skip to question 16
No, I have already achieved my weight loss goals or have completed the treatment
program at my facility --> skip to question 16
No, I am no longer participating in weight management (MOVE!) treatment.
15. Please indicate the main reason why you are no longer participating in weight management treatment.
While there may be more than one reason, we are interested in the MAIN reason why you are no longer participating. (Check one box)
I was not getting the kind of help or support that I needed.
I did not feel comfortable participating.
Treatment was not offered at a convenient time for me.
Treatment was not offered at a convenient location for me.
Transportation to get to treatment was limited or too expensive
I have too much pain.
I have too many other health problems.
I have too many other responsibilities (for example work or family obligations).
I lost my interest or motivation to participate.
Other.
16. Did you have any expenses related to weight management treatment in the VA that you paid for yourself?
(Check one box)
Yes
No
I don’t know
17. In the last two years, did you use a weight management treatment program outside of the VA? (Examples include Weight Watchers, Jenny Craig, Nutrisystem, TOPS, private medical provider or a community-based program). (Check one box)
Yes
No skip to question 19
I don’t know skip to question 19
18. If you answered “Yes” to the above question, please indicate the MAIN reason you used a weight management treatment program outside of the VA. (Check one box)
More convenient than the treatment available at the VA.
Better support for my specific needs than treatment available at the VA.
Better weight loss results than what I was achieving with treatment available at the VA .
I was able to do these programs with someone else (like a friend or family member), which I can’t do at the VA.
I tried an outside VA program before participating in VA weight management treatment.
Other.
19. How likely are you to use the following for weight management (MOVE!) treatment?
(Check one box for each statement)
|
Very Unlikely |
Somewhat Unlikely |
Somewhat Likely |
Very Likely |
I don’t know |
a) Group clinic-based care with other patients receiving similar treatment |
|
|
|
|
|
b) Individual clinic-based care |
|
|
|
|
|
c). Telephone-based care |
|
|
|
|
|
d) Internet-based care |
|
|
|
|
|
e) Care delivered through home messaging devices that are connected to your home telephone |
|
|
|
|
|
f) Care delivered through messages sent to your cell phone |
|
|
|
|
|
Lastly, please tell us about yourself so that we can better understand your experiences and preferences.
20. What is the highest level of education you have completed? (Check one box)
Less than high school graduate
High school graduate
Some college, vocational or technical school
College graduate of 4 year school
Post college
21. What is your ethnicity? (Check one box)
Not Hispanic or Latino
Hispanic or Latino
22. What is your race? (Check one or more boxes to indicate what you consider yourself to be.)
White
Black or African American
American Indian or Alaska Native
Asian
Native Hawaiian or other Pacific Islander
Other
23. What is your marital status? (Check one box)
Married
Living as married (living with fiancé, boyfriend or girlfriend but not married)
Separated or Divorced
Widowed
Single, never married, and not living as married
24. Do you have internet access at home? (Check one box)
No
Yes Check the type of internet access you have at home (Check one box )
High speed (cable modem, DSL, T-1 line, satellite)
Dial-up
Unknown
25. Do you have internet access at work? (Check one box)
No
Yes
Not applicable
26. Please choose the box that best describes how much you agree with each of the following statements.
(Check one box for each statement)
|
Strongly disagree |
Somewhat disagree |
Neither agree nor disagree |
Somewhat agree |
Strongly agree |
Not applicable |
a) I regularly use computers. |
|
|
|
|
|
|
b) I am comfortable using computers. |
|
|
|
|
|
|
c) I am comfortable using a cellular/mobile phone for text messaging. |
|
|
|
|
|
|
VA
Form 10-0472
June 2009
| File Type | application/msword |
| File Title | Patient Experiences with the MOVE! Weight Management Treatment Program |
| Subject | Patient Experiences with the MOVE! Weight Management Treatment Program |
| Author | Leila Kahwati |
| Last Modified By | vhacoharvec |
| File Modified | 2009-07-09 |
| File Created | 2009-07-09 |
© 2026 OMB.report | Privacy Policy