Allocation of Resources for Fire Service and Emergency Medical Service
Allocation of Resources for Fire Service and Emergency Medical Service
0693-0047 Survey Instrument 7-1-09
Allocation of Resources for Fire Service and Emergency Medical Service
OMB: 0693-0047
OMB Control No. 0693-0047
Expiration Date: 7/31/20XX
National Institute of Standards and Technology (NIST)
Allocation of Resources for Fire Services and Medical Services
Economic Consequences Survey Instrument
Question D1. Total Annual Direct Economic Losses (Fire Loss) for years 2005, 2006, and 2007 (structure and contents)
To answer this question provide an estimate to the nearest U.S. dollar of the total fire loss including physical damages caused by fires to structures and their contents that has occurred in your entire department’s coverage area over the last 3 years. Consider only physical damages and not damages such as close of business.
Firefighter Incident Related Injury and Death
Question D2. Total Number of Workers Injured for years 2005, 2006, and 2007
Using your departmental records, provide a whole number of responding personnel (firefighters or paramedics) who sustained an injury while on duty, regardless of whether or not the injury occurred during a response. Leave the field blank if there were no injuries. Please note the separate boxes for “fire” and “EMS” injuries. Of greatest interest are injuries that required one or more of the following:
1) Medical attention.
2) Taking the rest of the shift off.
3) Missing one or more days of work.
Multiple injuries to an individual firefighter (or paramedic) may be counted more than once provided that their injuries occurred on different responses.
Question D3. Total Number of Work Hours Lost for years 2005, 2006, and 2007
Using your departmental records, provide the total number of 'hours of scheduled work' missed due to personnel injury or death, within the last three years. Please note the separate boxes for “fire” and “EMS.”
Question D4. Total Number of Hours on Work Restriction (Light Duty) for years 2005, 2006, and 2007
Using your departmental records, provide the total number of hours that your departmental staff spent on work restriction as a result of on-duty injuries, within the last 3 years. Work restriction is synonymous with "light duty."
Question D5. Total Number of Workers Killed for years 2005, 2006, and 2007
Provide the total number of line-of-duty deaths occurring in your department in the last 3 years. These are to include deaths occurring during fire ground activity or during an EMS response or transport.
Civilian Incident Related Injury and death
Question D6. Public Citizen /Civilian-Fire related injuries for years 2005, 2006, and 2007
Provide the total number of civilians injured as a result of fires in your community within the last three years.
Question D7. Civilian Fire Fatalities for years 2005, 2006, and 2007
Provide the total number of citizens/civilians killed as a result of fires in your community within the last three years.
4.1.2 Profile
This section of the guide details each question asked in the “Profile” tab of the department survey.
Fitness Program
The questions in this section are about your department’s fitness program, if one exists. Check the appropriate button for each question.
Question D8. Does the department have a formal fitness/wellness program?
If your department has organized and implemented a physical fitness or wellness program click “Yes”, otherwise click “No.”
Question D9. Do you have an annual physical fitness assessment for all responding personnel?
If your department conducts an annual physical fitness assessment click “Yes”, otherwise click “No.”
Question D10. What proportion of stations have fitness equipment for use by on-duty personnel?
If your department has fitness equipment in stations, click the appropriate response based on your situation.
Question D11. Do you allow time on duty for cardiovascular workout?
Click “Yes” If you are allowed time for cardiovascular exercise while on duty, otherwise click “No.”
Question D12. Do you have an incumbent employee physical ability test?
If your department conducts periodic (at least annual) physical ability tests, click “Yes”, otherwise click “No.”
Examples of physical ability tests:
Firefighting specific: dry/charged hose drags, victim rescue, attic crawl, etc.
Standard/Traditional: sit-ups, pushups, sit-and-reach, etc.
Question D13. Do you have medical physical exams for incumbent responders/firefighters/paramedics)?
Click “Yes” If your department conducts medical physical exams for firefighters/paramedics (sometimes known as sworn personnel), otherwise click “No.”
Training
These questions ask about your department’s fire and EMS training requirements. Check all appropriate buttons and boxes. For text boxes provide an estimate of the number of hours related to the specific question asked. It is important to know the quantity and types of training necessary to benefit fire departments and their communities.
D14. Do you have regular in-service training programs for all responders conducted at the Company or Department training level?
If your department has conducts regular training for all employees click “Yes”, otherwise click “No.”
Examples of training:
Company evolutions
Classroom sessions
Morbidity and Mortality rounds (“M&Ms”)
Close call bulletins
D15. How many hours of Fire suppression related training are provided per employee annually (on average)?
Enter the number of hours of fire suppression related training the average employee is provided annually into the field. Include both practical and classroom training.
D16. Do you conduct regular standard company evolutions?
If your department regularly conducts standard company evolutions for all employees click “Yes”, otherwise click “No.”
D17. Which evolutions are regularly conducted? [Pick all that apply]
From the list of options provided, check all the boxes next to the type of company evolutions that your employees participate in on a regular basis.
D18. How many hours of ALS related training are provided per ALS provider annually (on average per employee)?
Enter the number of hours of ALS related training provided to the average ALS provider annually. Include both practical and classroom training.
D19. How many hours of BLS related training are provided per BLS provider annually (on average per employee)?
Enter the number of hours of BLS related training provided (on average) per provider annually. Include both practical and classroom training.
D20. Which EMS topics are regularly taught? [Pick all that apply]
From the list of options provided, check all the boxes next to the type of EMS topics that are regularly offered to your employees.
Emergency Medical Dispatch
This section asks whether or not your department uses scripted dispatching. Scripted dispatching has dispatchers follow written guidelines for caller interaction to determine the severity (ALS or BLS) of a call and to send the appropriate resource. Some examples of scripted dispatch programs are the Medical Priority Dispatch system (MPD), the Association of Public-Safety Communications Officials system (APCO), or a generic Emergency Medical Dispatch system (EMD).
D21. Does your dispatch center use scripted dispatch for EMS calls (Medical Priority Dispatch, EMD, APCO etc.)?
Click “Yes” if your dispatching center uses any of the following protocols:
Medical Priority Dispatch system (MPD)
the Association of Public-Safety Communications Officials system (APCO)
Generic scripted Emergency Medical Dispatch system (EMD)
Otherwise, click “No.”
Call intake/Call Processing/Dispatch
The questions in this section regard whether your dispatch center is first to receive 911 calls (primary call center) or whether the calls are routed from another center that takes 911 calls. Also asked are the backgrounds of the personnel that dispatch calls.
D22. Is your dispatch center a primary 9-1-1 call intake center?
Click “Yes” if your dispatch center is the first to receive a 9-1-1. For any other case click “No.”
D23. Is your dispatch center a secondary answering point that receives calls from a 9-1-1 center?
Click “Yes” if 9-1-1 calls are routed to your dispatch center from another location that first answers 9-1-1 calls. For any other case click “No.”
D24. Which of the following best describes call takers in your dispatch center? [Mark all that apply]
Mark all the boxes that describe type of experience the call takers have in your dispatching center.
D25. Which of the following best describes dispatchers in your dispatch center? [Mark all that apply]
Mark all the boxes that describe type of experience the dispatchers have in your dispatching center.
Public Health Programs
The questions in this section regard the health related public education programs hosted by your department. School Presentations include programs offered at schools of any level, k-12, college, etc. Senior Presentations include programs that your department offers at senior centers and residences. The field entitled “Other” is left open as an option to input additional public health programs that your department conducts, separated by commas.
D26. Does your department spend time on public health programs?
Enter the total number of hours that your department spends annually on conducting public health programs. For examples of public health programs see question D27 in the survey.
D26a. How many hours per year does your department spend in Public Health programs? Estimation is appropriate.
D27. Which programs do you conduct? [Mark all that apply]
Mark all the boxes that describe type of public health programs your department conducts.
Fire Safety Programs
The questions in this section regard fire safety public educational programs hosted by your department. School Presentations include programs offered at schools of any level, k-12, college, etc. Senior Presentations include programs that your department offers at senior centers and residences. The field entitled “Other” is left open as an option to input additional fire safety programs that your department conducts, separated by commas.
D28. How many hours per year does your department spend in fire safety and health programs? Estimation is appropriate.
Enter the total number of hours that your department spends annually on conducting fire safety programs. For examples of fire safety programs see question D26.
D29. Which programs do you conduct? [Mark all that apply]
Mark all the boxes that describe type of fire safety programs your department conducts.
4.1.3 Response Capacity
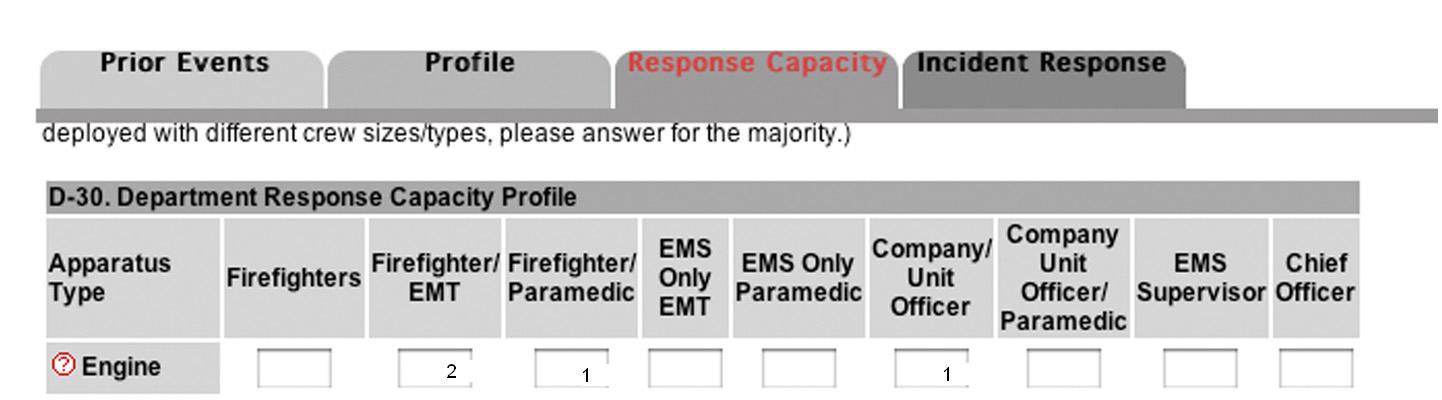
This section of the guide details each question asked in the “Response Capacity” tab of the department survey. Please provide a description of the crew typically deployed on each of the apparatus. This section is intended to record the number and level of training of personnel on each type of apparatus. (Note: If similar apparatus deployed with different crew sizes/types, please answer for the majority.) Drivers/Engineers should be categorized appropriately based on their level of training as a firefighter, paramedic or both.
Engine:
For this row, fill out the typical staffing of one of your department’s engine companies including officers. Each column corresponds to the training level of your personnel.
Example:
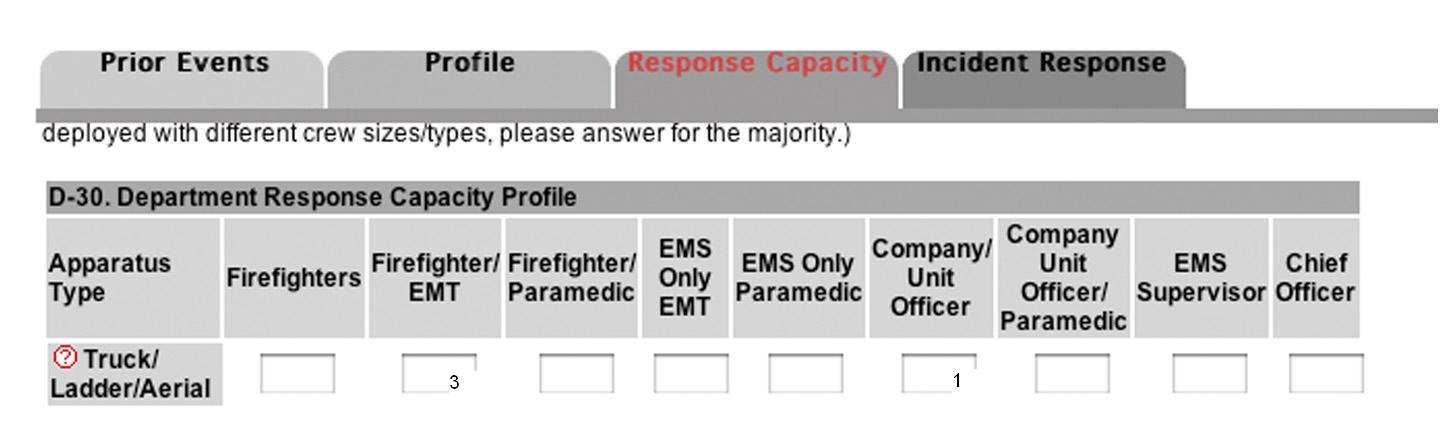
Truck/Ladder/Aerial:
For this row, fill out the typical staffing of one of your department’s Truck/Ladder/Aerial companies including officers. Each column corresponds to the training level of your personnel.
Example:
Other:
For this row, first input the type of “other” unit that describes any apparatus your department typically staff, then input the typical staffing for that apparatus. Each column corresponds to the training level of your personnel.
4.1.4 Incident Response
This section of the guide details each question asked in the “Incident Response” tab of the department survey. Please provide a description of resources typically sent to each call type. This section is intended to record the number and type of apparatus sent to each type of incident.
Investigate Odor:
For this row, input the number of each type of apparatus that you typically dispatch to ‘Investigate an Odor’
Example:

Fire Alarm Sounding Residential:
For this row, input the number of each type of apparatus that you typically dispatch to a "fire alarm sounding only."
Alarm Sounding Commercial:
Reported Single Family Residential Structure Fire:
For this row, input the number of each type of apparatus that you typically dispatch to a “reported single family structure fire.”
Reported Commercial or Multi-Family Residential Structure Fire:
For this row, input the number of each type of apparatus that you typically dispatch to a “reported commercial or multi-family structure fire.”
Reported High-Rise or other High Risk Occupancy Fire:
For this row, input the number of each type of apparatus that you typically dispatch to a reported high-rise or other high risk occupancy fire.
Other:
For this row, enter the number of apparatus the department typically dispatches to another relevant ‘structure’ not covered above. PLEASE DO NOT enter information for vehicle fires.
BLS:
For this row, input the number of each type of apparatus that you typically dispatch to a BLS incident.
Public Assistance:
For this row, input the number of each type of apparatus that you typically dispatch to a Public Service.
ALS – Cardiac:
For this row, input the number of each type of apparatus that you typically dispatch to an ALS - Cardiac incident.
ALS – Trauma:
For this row, input the number of each type of apparatus that you typically dispatch to an ALS - Trauma incident.
ALS – Other:
For this row, input the number of each type of apparatus that you typically dispatch to an ALS Call that is not Cardiac or Trauma. (e.g. Severe Respiratory distress or non breathing patient)
4.2 Station Background Information Survey
The following section will describe in detail the expected answers for the questions presented on the station background survey. To begin, start by navigating to the station survey page. You may do this from any page within the Fire Reporting System web site by clicking on the “Complete Surveys” button on the menu on the left side of your screen. The “Complete Surveys” page presents you with red buttons for the department, station and incident surveys as well as for changing your username/password. Click on the “Station Survey” button. If you need help to answer any of the questions, put your mouse over the question mark next to the number of the question and you will see a brief description of what to do. If you need more help, consult the explanations found below.
4.2.1 Community Profile
This section of the guide details each question asked in the “Community Profile” tab of the department survey.
Before you begin the numbered questions, you are asked to select the appropriate station from the drop down list. Select one of the stations that have been selected for your department. You will answer the questions that follow once for each station in the list. You will go through all questions for the station selected, then go back to ‘station survey’ and select a different station. You will then answer all the questions for that station and so on until the questions have been answered and submitted for each of your stations selected into the study. The list of stations was sent to your chief. If you do not have the list, please contact your chief or Dr. Lori Moore-Merrell at 202-824-1594 or Lmoore@iaff.org.
Demographic Profile
Question S1: Density: Please select the area description for your response area. (Estimation is appropriate - round off to nearest 10%)
Complete the four fields describing the population densities of your station coverage area. Please estimate the makeup of your area to within 10%. For example, a downtown city station may have 100% urban coverage, while another station in your department may cover 20% urban, 70% suburban and 10% wilderness. This applies only to a particular station. Please check to be sure that your selections total 100%.
Question S2: What percentage of buildings in your area are three stories or higher? (Estimation is appropriate – round off to nearest 10%)
Out
of the total number of buildings in your station coverage area, how
many of them are three full stories or greater in height on the
tallest side? Select the percentage that best matches your estimate
from the drop down list. Past fires have shown that building height
can have a significant impact on the effectiveness and outcome of
fire operations.
Question S3: What percentage of each type of structure does your station cover? (Estimation is appropriate - round off to nearest 10%)
For your station, what is the percentage of each occupancy category listed in under this question that makes up your coverage area? Estimate to within 10%. Ensure that your total of all occupancies sums to 100% by looking at the final box. Building occupancy is likely relevant to the outcome of fire operations as it relates the number of people and property at risk to the potential severity and occurrence of fires.
Coverage Area
Question S4: How many square miles does your station cover (your first due area)? Round off to the nearest mile.
What is the total coverage area of your station in square miles? Input a whole number into the field provided. Round your estimate to the nearest mile. This information is important to understanding the response and transport times as well as the deployment of your department's resources related to geography.
Population
Question S5: What is the approximate population of the area your station covers?
Please click one of the radio buttons corresponding to the range of population into which your immediate coverage area fits. This information is important to understanding your department's deployment of resources related to the population served.
Question S6: What is the annual incident volume for actual structural fires and actual ALS patients for your station?
For each general type of call, fill in each field using your department's records. This data helps to understand your department's deployment of resources related to the local demand for services. Please use the final ‘call type’ as opposed to ‘dispatch’ for determining which category to select.
Median Income
The median household income for ____ is $____
What is the average household income for your immediate coverage area? Median household income for your city/county will be shown.
Question S7: Is the median income in your coverage area higher, lower or roughly the same as the city/county/parish median?
You should estimate whether the jurisdiction the station services is higher, lower, or equal to this amount. Previous studies have shown that income levels significantly impact the occurrence and outcome of fires. Use the fields provided to break down the income of the population within your immediate coverage area. Provide estimations to the nearest 10%. For example, you may have a very affluent population that makes up only 10% of your coverage area. The rest may be 50% the same income and 40% lower income. Using the final box, ensure that your total is 100%.
Age Demographics
Question S8: What is the estimated age breakdown of your station coverage area during peak occupancy period? (Estimate to the nearest 10%.)
Use the fields provided to break down the ages of the populace in your station coverage area. Using the final box, ensure that your total is 100%. This information is important because previous studies have identified different risks for different age groups. Namely, the very young and very old are at a higher risk of death in a fire.
Race Demographic
Question S9: Please check the race groups that represent greater than 20% of the population in your coverage area during peak occupancy period.
Check all boxes that apply for the categories provided to describe the race/ethnic make-up of your immediate coverage area. Your occupancy may change seasonally because of college or tourist populations. Previous studies have identified that race/ethnicity may be related to the outcome of fires, but results of these studies are conflicted.
4.2.2 Code Enforcement
This section of the guide details each question asked in the “Code Enforcement” tab of the department survey.
Question S10: Excluding single and duplex structures, what is the percentage of structures in your response area that are inspected annually?
Input the percentage of structures annually inspected, excluding single and duplex residential structures. Building inspections are important to report as code compliance is critical to reducing the risk and improving the outcomes of fires. Single and duplex structures are not considered in this study because they are not traditionally inspected.
4.3 Incident Data Collection Survey
The following section will describe in detail the expected answers for the questions presented on the incident data collection survey. To begin, start by navigating to the incident data collection survey page. You may do this from any page within the Fire Reporting System web site by clicking on the “Complete Surveys” button on the menu on the left side of your screen. The “Complete Surveys” page presents you with red buttons for the department, station and incident surveys as well as for changing your username/password. Click on the “Incident Survey” button. If you need help to answer any of the questions, put your mouse over the question mark next to the number of the question and you will see a brief description of what to do. If you need more help, consult the explanations found below.
Once on the incident survey page, you will be asked to select either ‘Fire’ or EMS’ incident. Click the appropriate button based on the type of call for which you are entering data. Once you choose the call type, you will be asked another question regarding the magnitude of the incident. For ‘Fire’ incidents, you are asked to enter data for ‘working fire involving spread beyond the item of ignition’. For ‘EMS’ incidents, you are asked to enter data for ‘confirmed ALS events’.
If you answer ‘Yes’ to confirm that the incident for which you are prepared to enter data meets the described criteria for ‘Fire’ or ‘EMS’, you will be taken to the first question in the survey to begin data entry.
4.3.1 Notification
This section of the guide details each question asked in the “Notification” tab of the department survey.
Station:
Before beginning this survey, select the station for which you are entering incident data. You will enter multiple incidents, both for structure fires and ALS responses for each station.
Department Incident Code/Number:
Enter the Incident Number associated with the event you are entering. Use the incident numbering system for your department. This number allows you to track the call in this study if you wish to edit the information entered in the future.
Incident Response Profile
Question I1: Fire Dispatch Call Type
Select the call type as DISPATCHED from the drop down list.
Question I2: Scene Type/Location
Select the scene type reported in the initial dispatch by using the drop down list.
Question I2a: Did the first due responding company have a pre-plan for the structure?
A pre-plan is developed for each building/location and each plan should take into account the type and scale of an adverse risk event (incident), the potential mitigation approaches and the resources required to respond to the incident. In the event of an incident, the preplan should be rapidly converted into a realistic and effective operational response. Select yes or no.
Question I1: EMS Dispatch Call Type
Select the call type as DISPATCHED from the drop down list.
Question I2: Scene Type/Location
Select the scene type reported in the initial dispatch by using the drop down list.
Question I3: Mutual Aid?
Did this incident require the additional dispatch of resources outside of your department? Click the appropriate radio button.
Question I4: Automatic Aid?
Did this incident result in the simultaneous response of additional resources from outside of your Department as previously arranged with another community or district? Click the appropriate radio button.
4.3.2 Response
This section of the guide details each question asked in the “Response” tab of the department survey.
Question I5: Scene/Type Location
Select the observed call type ON ARRIVAL from the drop down list.
Incident Response Profile:
In
this section, please provide a description of resources typically
sent to each call type. This section is intended to record the number
and type of apparatus sent to each type of incident section. PLEASE
ENTER EVERY APPARATUS THAT WAS DISPATCHED TO THIS EVENT.
Question I6: What resources were deployed to this incident? Indicate the number of each apparatus below.
For each apparatus type, enter the number that was deployed to the incident.
Question I7: The 9-1-1 Call Pickup Time
Enter the exact time that the 9-1-1 call taker answered the phone (HH:MM:SS Format). If you did not record this time stamp and cannot enter it, please leave this field blank
Question I7 (EMS)
What resources were deployed to the incident. Indicate the number of each apparatus below.
4.3.3 Intervention
This section of the guide details each question asked in the “Community Intervention” tab of the department survey. This section is to be completed with the times at which specific response events occurred during your entire emergency response, beginning from when a 911 call is answered through arrival of the first apparatus on scene. Use 24-hour military “clock time” format: (HH:MM:SS Format)
Question I8 (For EMS only) - 9-1-1 Call Pick up time.
Time the 9-1-1- call taker answers the phone if this is different from fire department call intake, for example a secondary PSAP.
Question
I8 (Question I9 for EMS) : Fire Department Dispatcher = Fire
Department Alerted
Enter the exact time that your department’s dispatcher answered the phone (or was alerted by the primary call taker (HH:MM:SS Format). If you did not record this time stamp and cannot enter it, please leave this field blank.
Question I9 (Question I10 for EMS): Dispatch Time
Enter the exact time that your department’s dispatcher answered the phone (or was alerted by the primary call taker (HH:MM:SS Format)). If you did not record this time stamp and cannot enter it, please leave this field blank.
Question I10 (Question I11 for EMS): Enroute Time
Enter the exact time at which the unit dispatched was prepared to leave and began its response (apparatus wheels start to move (HH:MM:SS Format)). If you did not record this time stamp and cannot enter it, please leave this field blank.
Question I11: Arrival Time
Enter the exact time that the first apparatus arrived on scene (wheels stopped, responders ready to exit the vehicle (HH:MM:SS Format)). If you did not record this time stamp and cannot enter it, please leave this field blank.
Question I12: BLS Arrival Time (EMS only)
Enter the exact time that the BLS apparatus dispatched to this incident arrived on scene (wheels stopped, responders ready to exit the vehicle (HH:MM:SS Format)). If you did not record this time stamp and cannot enter it, please leave this field blank.
Question I12: Occupant Attempted Extinguishment
Click the button for yes if prior to your arrival a bystander or occupant attempted some method of extinguishment. Otherwise click no.
Question I13: ALS Arrival Time (EMS only)
Enter the exact time that the ALS apparatus dispatched to this incident arrived on scene (wheels stopped, responders ready to exit the vehicle (HH:MM:SS Format)). If you did not record this time stamp and cannot answer it, please leave this field blank.
Question I14: At Patient Side Time (EMS only)
Enter the exact time that emergency medical personnel arrived at the patient's side and began to assess the patient and administer medical aid (HH:MM:SS Format). If you did not record this time stamp and cannot enter it, please leave this field blank.
FIRE Early Intervention
Question I13: Sprinkler Activated
Click the button for “yes” if the building's sprinkler system automatically activated prior to your arrival. Otherwise click "no.”
Question I14: Monitored Alarm Activated
Click the button for “yes” if alarm activation occurred at an actively staffed alarm monitoring station. Otherwise click “no.”
Question I15: Automatic Alarm Activated
Click the button for “yes” if an automatic alarm was activated prior to your arrival. Otherwise click “no.”
Question I16: Smoke Detector Activated
Click the button for “yes” if one or more smoke detectors were activated prior to your arrival. Otherwise click “no.”
Question I17: Other
Click the button for “yes” if any other means of fire suppression, control, notification or some other intentional activity was carried out prior to your arrival. Otherwise click “no”
Question I18: What resources actually engaged on this incident? Indicate the number of each apparatus below.
In this section, indicate within the columns how many more units were dispatched to this incident in addition to your department’s normal response.
EMS Early Intervention
Question I15: Attempted Intervention – AED
Click the button for “yes” if prior to your arrival a bystander attempted automatic external defibrillation. Otherwise click “no.”
Question I16: Attempted Intervention – CPR
Click the button for “yes” if prior to your arrival a bystander attempted to perform CPR. Otherwise click “no.”
Question I17: Attempted Intervention - Medicine Administration
Click the button for “yes” if prior to your arrival, qualified medical personnel administered medicine to the patient. Otherwise click “no.”
Question I18: Other
Click the button for “yes” if prior to your arrival any other means of medical care was attempted by medical personnel/bystanders. Otherwise click “no.”
4.3.4 Final Response
This section of the guide details each question asked in the “Final Response” tab of the department survey.
Question I19: Number of additional apparatus dispatched
In this section, indicate within the columns how many more units were dispatched in addition to your department’s initial response for this type of call.
Question I20: Patient Status during Incident (EMS Only)
How many patients were assisted? (Enter data for up to ten patients). For each patient repeat the following process.
On-Scene Assessment:
Blood Pressure: Enter the patient’s systolic blood pressure in the first field and diastolic blood pressure in the second field.
Pulse: Enter the patient’s heart rate in beats per minute.
Respiratory Rate: Enter the patient’s respiratory rate, in breaths per minute.
Respiratory Value: Select the patient’s respiratory value from the drop down list
Respiratory Sounds: Click “Abnormal” if the patient has any respiratory sounds that are not “Normal.”
Skin Color/Temp: Click “Abnormal” is the patient’s perfusion is any condition other than “Normal.” In addition, describe this condition further using the categories available in the drop-down list.
Pulse Oximeter: Input patient’s pulse Oximeter reading. If you did not capture an on-scene pulse Oximeter reading, leave this field blank.
EKG: Using your best judgment, indicate whether the patient’s EKG reading is “Normal” or “Abnormal.” If you did not capture an on-scene EKG reading, leave this field blank.
Pain Level (scale 1-10): Using the drop-down list record the level of pain the patient gave in your patient interview. If the patient is unconscious, leave this field blank. If you did not capture an on-scene pain level, leave this field blank.
Patient status upon Hospital Arrival:
Blood Pressure: Enter the patient’s final systolic blood pressure in the first field and diastolic blood pressure in the second field.
Pulse: Enter the patient’s final heart rate in beats per minute.
Respiratory Rate: Enter the patient’s final respiratory rate, in breaths per minute.
Respiratory Value: Select the patient’s final respiratory value from the drop down list. If ‘other’ please describe?
Respiratory Sounds: Click “Abnormal” if the patient still has any respiratory sounds that are not “Normal.”
Skin\Color Temp: Click “Abnormal” is the patient’s perfusion is any condition other than “Normal.” In addition, describe this condition further using the categories available in the drop-down list.
Pulse Oximeter: Input patient’s final pulse Oximeter reading if available. Otherwise leave it blank.
EKG: Using your best judgment, indicate whether the patient’s final EKG reading is “Normal” or “Abnormal.”
Pain Level (scale 1-10): Using the drop-down list record the level of pain the patient gave in your patient interview. If the patient is still unconscious, leave this field blank.
4.3.5 Outcome
This section of the guide details each question asked in the “Outcome” tab of the department survey.
Economic Incident Related Consequences
Question I19: Direct Economic Losses ($ estimated)
In the field provided, enter a dollar estimate of the amount of damage incurred to the structure and its contents.
Question I20: What percentage of the building(s) is considered to be a total loss?
What percentage of the building(s) is considered to be a total loss? Estimation is appropriate, use the drop down box provided.
Worker Incident Related Injuries and Death - [From Dispatch to In-Quarters]
Question I21: Total Number of Workers Injured
Input the number of emergency responders injured during the response, while working on-scene or any other time related to this incident. The injuries of greatest interest are those that required either; 1) medical attention, 2) taking the rest of the shift off.
Question I22: Total number of worker fatalities.
Did the individuals in question require any medical aid of any kind? Check “Yes” if they did, otherwise check “No.” May enter data for up to 10 workers.
I23: Total number of civilian/public citizen injuries:
Enter the number of public citizens or civilians who were injured during this incident.
I24: Total number of civilian/public citizen fatalities.
Enter the number of public citizens or civilians who were killed during this incident.
NOTE: This questionnaire contains collection of information requirements subject to the Paperwork Reduction Act (PRA). Notwithstanding any other provisions of the law, no person is required to respond to, nor shall any person be subject to penalty for failure to comply with, a collection of information subject to the requirements of the PRA, unless that collection of information displays a currently valid OMB Control Number. The estimated response time for this questionnaire is 8 minutes. The response time includes the time for reviewing instructions, searching existing data sources, gathering and maintaining the data needed, and completing and reviewing the collection of information. Send comments regarding this estimate or any other aspects of this collection of information, including suggestions for reducing the length of this questionnaire, to the National Institute of Standards and Technology, Attn., Jason D. Averill, Fire Protection Engineer, 100 Bureau Drive, Gaithersburg, MD 20899-8664, (301) 975-2585; or by email at jason.averill@nist.gov
| File Type | application/msword |
| File Title | Economic Consequences |
| Author | Beverly Lewis |
| Last Modified By | dyonder |
| File Modified | 2009-07-01 |
| File Created | 2009-07-01 |
© 2026 OMB.report | Privacy Policy