Racial and Ethnic Approaches to Community Health 2010 Information Network (REACH IN)
Racial and Ethnic Approaches to Community Health 2010 Information Network (REACH IN)
FINAL REACH IN supporting statement Dec 4
Racial and Ethnic Approaches to Community Health 2010 Information Network (REACH IN)
OMB: 0920-0603
REACH IN OMB Package Supporting Statement
OMB Package Supporting Statement
Racial and Ethnic Approaches to Community Health 2010 Information Network
Andrea M. Hegedus, Ph.D.
Northrop Grumman
Centers for Disease Control and Prevention (CDC)
National Center for Chronic Disease Prevention and Health Promotion (NCCDPHP)
Division of Adult and Community Health (DACH)
(770) 488-5462
Table of Contents
A. Justification……………………………………………………………………… 3
1. Circumstances Making the Collection of Information Necessary…...…… 3
2. Purposes and Use of Information Collection………………………………. 4
3. Use of Improved Information Technology and Burden Reduction………. 5
4. Efforts to Identify Duplication and Use of Similar Information…………. 5
5. Impact on Small Businesses or Other Small Entities……………………... 7
6. Consequences of Collecting the Information Less Frequently…………… 7
7. Special Circumstances Relating to the Guidelines of 5 CFR 1320.5……... 7
8. Comments in Response to the Federal Register Notice
and Efforts to Consult Outside the Agency.................................................. 7
9. Explanation of Any Payment or Gift to Respondents.................................. 7
10. Assurance of Confidentiality Provided to Respondents............................. 8
11. Justification for Sensitive Questions............................................................ 8
12. Estimates of Annualized Burden Hours and Costs.................................... 9
13. Estimates of Other Total Annual Cost Burden
to Respondents or Record Keepers............................................................... 9
14. Annualized Cost to the Government...........................................................10
15. Explanation for Program Changes or Adjustments..................................10
16. Plans for Tabulation and Publication and Project Time Schedule..........10
17. Reason(s) Display of OMB Expiration Date is Inappropriate..................10
18. Exceptions to Certification for Paperwork
Reduction Act Submissions...........................................................................11
B. Collections of Information Employing Statistical Methods..............................12
1. Respondent Universe and Sampling Methods..............................................12
2. Procedures for the Collection of Information...............................................12
3. Methods to Maximize Response Rates and Deal with Nonresponse..........12
4. Tests of Procedures or Methods to be Undertaken......................................12
5. Individuals Consulted on Statistical Aspects and Individuals
Collecting and/or Analyzing Data.................................................................12
A. Justification
1. Circumstances Making the Collection of Information Necessary
In 1999, the Centers for Disease Control and Prevention (CDC) launched the Racial and Ethnic Approaches to Community Health (REACH) 2010 demonstration project as authorized by Public Health Service Act, Title 42 United States Code, Chapter 6A - Public Health Service, Subchapter II - General Powers and Duties, Section 241 Research and Investigation (42USC241). (Attachment 1) REACH 2010 is designed to eliminate racial and ethnic disparities in the following six health priority areas: breast and cervical cancer screening and management, cardiovascular disease, diabetes, HIV infections/AIDS, immunizations, and infant mortality. Racial and ethnic groups targeted by REACH 2010 include African Americans, American Indians, Alaska Natives, Asian Americans, Hispanic Americans, and Pacific Islanders. The project is designed to:
Support community-based coalitions with high potential to implement and evaluate innovative strategies aimed at eliminating local racial/ethnic health disparities;
Document activities within local environments and analyze differences and similarities among environments; and
Develop novel approaches that target effectiveness of programs aimed at eliminating health disparities nationally.
REACH 2010 uses a program logic model to link activities and processes to short- and long-term outcomes. Five stages are used in the logic model to capture and assess effects of REACH grantee activities. These stages are: (1) capacity building; (2) targeted action; (3) community and systems changes and change among change agents; (4) widespread risk/protective factors change; and (5) health disparity reduction.
The REACH IN system is a customized internet-based support system that allows Racial and Ethnic Approaches to Community Health (REACH 2010) Program grantees to perform remote data entry and retrieve data on grantees' evaluation activities. These activities track the first stages of the REACH 2010 logic model, including capacity building, targeted action, community and systems change, and change among change agents. This support system also is designed to create on-demand graphs and reports of grantees’ actions and accomplishments. The system may be used to meet the reporting requirement of their cooperative agreements with CDC. There is no cost to users. For purposes of this OMB Supporting Statement, grantee users are considered respondents.
To support grantees’ evaluation efforts, CDC has approved the customization of this internet-based data warehousing application (www.reach2010.net). This system, the REACH Information Network (REACH IN), enables users to document and systematize activities related to organizational and community efforts. User documentation includes identification of interventions, maintenance of progress notes, and creation of outcome and process indicators to monitor progress. These efforts are related to three stages of the REACH 2010 logic model:
Capacity building,
Targeted actions, and
Community and systems changes, and change among change agents.
All data collection and entry are performed by REACH 2010 grantees. Users are supported with technical assistance and training, covering the usage of the system from a content/project goals perspective, and technical operations. Grantees may use the system to meet evaluation reporting requirements contained within their existing cooperative agreements with CDC. No adverse actions are imposed on grantees for refusing to use or discontinuing use of the REACH IN system. The REACH IN system allows users to enter contact information to facilitate communication within and between grantee organizations. However, users have the ability to make this contact information private (that is, not viewable by other users).
Attachment 3 contains the complete REACH IN design document and screen captures of the system.
2. Purposes and Use of Information Collection
CDC’s REACH 2010 grantees that use the system are considered respondents for the purpose of this supporting statement. The REACH IN system provides a vehicle for grantees to store information regarding their evaluation activities related to capacity building, targeted actions, community and systems change, and change among change agents. This information includes descriptions of project issues and interventions, progress notes, indicators measures, and numerical indicator data. Information collected is used to meet CDC’s evaluation reporting requirements for the REACH 2010 project. Grantees are required to submit reports twice a year to CDC. The system allows each respondent to generate easily a report of evaluation data they have entered. Grantee/respondents have secure access to the web-based system at any time from any computer connected to the Internet.
REACH IN is an efficient and accessible means to document the challenging hurdles encountered as coalitions address health disparities issues. Lessons learned through the use of such a system can be applicable to other community and governmental organizations facing similar health change challenges, as well as other organizations seeking to document the naturally occurring lessons born of experience that are often lost due to the lack of such a recording system. REACH IN creates an electronic record of these events, allowing relatively easy, albeit secure, sharing of information. It also allows opportunities for qualitative analysis not available previously to grantees or CDC staff.
A substantial benefit of the system is the reduction in respondent burden. This reduction in burden is represented by the increased efficiency in documenting activities as they occur, rather than recollecting experiences when reports are prepared.
Use of the system has two primary benefits to the government. Foremost and most practical is the increased quality, accuracy, consistency, comparability, and evaluability of the contents of REACH 2010 grantee reports. Simply put, CDC program staff is better able to make policy decisions based on improved reporting from its grantees. The second benefit stems from the first. Through better documentation of the challenges, and the mechanisms put into place to overcome these challenges, the public health field is better equipped to identify the most effective and efficient means to reduce racial and ethnic health disparities. These efforts lead to improved public resource allocation in this area.
3. Use of Improved Information Technology and Burden Reduction
REACH IN is a web-based data warehousing application that is made available to grantees that are documenting and organizing evaluation of community activities. The system is available through a secured Internet web interface. Fundamentally, it is a system designed to reduce burden through the use of improved information technology. This objective is achieved by increasing the ability of respondents to document activities in pursuit of the aims of their cooperative agreement, and then generating a report of those activities to fulfill their evaluation reporting requirements. While the system is available at all times, the assumption is that data entry occurs quarterly and reports are submitted semi-annually.
While the system does not fully automate the data entry process, users of the system can easily cut and paste existing electronic narrative and numerical data into the system. In the case of numerical data, for instance, respondents identify an outcome or process indicator measure to monitor progress. For example, the number of new diagnoses of diabetes cases within the community might be a measure of program effectiveness. As these data are available, the respondent can create and complete a data table for this measure. The system is automated to the extent that once health disparity or other data have been entered to allow monitoring of one activity; these data are automatically available to monitor any other activity using the same indicator measure.
Other examples of system automation can be found in the reporting tool within the system. Respondents have the option of generating a standard progress report with a single click on the reporting page. This activity extracts specified data into a report format defined by CDC REACH 2010 program staff that forms the basis of required evaluation reports.
4. Efforts to Identify Duplication and Use of Similar Information
No other centralized system of similar capability for storage and retrieval of existing evaluation data are available to REACH 2010 grantees.
The CDC REACH 2010 program requires the collection of data suitable for process and outcome evaluation of capacity building, targeted action, and systems change and change among change agents intervention activities. In its initial development, effort was made to establish the kind and extent of data the REACH IN system allows grantees to document. These efforts included consulting various government officials with knowledge of the subject area, including Dr. Terrie Sterling, Chief, Community Health and Program Services Branch, Division of Adult and Community Health, National Center for Chronic Disease Prevention and Health Promotion, Centers for Disease Control and Prevention.
Additionally, CDC staff consulted with REACH 2010 grantees regarding their current access to tools that capture, evaluate, and report intervention activities related to capacity building, targeted action, and community and systems change and change among change agents. Less than twenty five percent of these grantees indicated they had or planned to develop a “system” for collecting such data. The difficulty is that each system developed is idiosyncratic to the grantee organization, regardless of the quality of the system. CDC’s need for uniform and systematic documentation of all grantee efforts necessitated the creation of a single tool for such data warehousing.
Researchers working in the areas of community and public health, were consulted during the initial development of REACH IN, including Dr. Robert Gold, Dean of the College of Health & Human Performance at the of the University of Maryland; and Mr. Michael Bilton, Executive Director of the Association for Community Health Improvement, Health Research and Educational Trust. To the best of their knowledge, there was no existing web-based application that performed functions similar to those designed into REACH IN. Further, it was their independent opinion that high quality data sought by REACH IN did not exist. It was also their understanding that REACH 2010 grantees are responsible for determining and collecting specific community-level data for local projects. The unique contribution of REACH IN is the assembly and organization of these data into meaningful contexts for effective evaluation, planning, decision-making, and actions by grantees. Mr. Bilton communicated that based on his research, various performance management and improvement systems, project management systems and data handling systems are available. However, he did not find a tool that takes population and program data and allows the user to put it in the context of community health improvement goals, as offered by REACH IN.
Attempts were made to identify existing web based systems to assist in evaluating community based activities as well as databases and published literature on community based approaches to reduce health disparities. Searches for existing web-based applications that would allow grantees to collect and document efforts were unsuccessful. Several web sites exist to guide the development of intervention and evaluation efforts, but these sites do not allow data warehousing of local or other aggregate level data. These sites do not specifically address the ability to evaluate effectiveness of various capacity building, targeted action, or systems change and change among change agent interventions.
A literature search also was conducted to identify any existing data or evidence regarding scientifically valid interventions to address health disparities. Many of these extrapolate their conclusions into recommending the need to identify targeted interventions. Hogan, Njoroge, Durant, Ferre (2001) cite the value of qualitatively understanding the social context of infant mortality and preterm delivery, and in the potential for applying the results of qualitative studies to the reduction of health disparities. In documenting the existence and impact of disparities related to the distribution of disease knowledge and self management to patients, Souraya (2002) indicates the need for improved information collection regarding interventions. It is particularly important to collect formative outcome data that could inform the continuous improvement of interventions.
While there are examples of local intervention efforts (e.g., Hae-Ra et al. 2002), the literature lacks research-based descriptions of specific interventions and methods used to gather, analyze, and evaluate activities geared toward reducing health disparities at the local level (i.e., building community capacity, developing targeted actions, changing existing systems and fostering change among change agents). The literature search verifies a need for the results anticipated by the use of REACH IN.
5. Impact on Small Businesses or Other Small Entities
REACH 2010 grantee organizations may be small businesses or small entities or they may work closely with small businesses or small entities to fulfill the work of their individual cooperative agreements. Every effort was made during the design and development of the REACH IN system to minimize the effort and burden on the respondent. These efforts stem from the design principles of never asking for data inputs that will not be used, and if a specific datum is used as input, it is only asked for once. The absolute minimum amount of information input from the respondent is provided for in the system, and where ever appropriate and possible data is retrieved automatically for the user from previous data entries. REACH 2010 grantees’ use of the system increases their efficiency to meet evaluation reporting requirements, and therefore, represent a reduction in burden.
6. Consequences of Collecting the Information Less Frequently
The consequences of not using REACH IN quarterly would be an increased burden on the respondents to produce their semi-annual evaluation report as required by their cooperative agreements with CDC. Further, the consequences of using the REACH IN less frequently or not using such a system would include a reduced capacity of each grantee to systematically record ephemeral knowledge related to the implementation of their demonstration project. This can reduce the accuracy in recording barriers and successes related to reducing racial and ethnic health disparities. In turn, less frequent data collection would reduce the amount, validity, and reliability of information available to resource and policy decision makers from the community and government, including CDC. There are no legal obstacles to reducing the burden.
7. Special Circumstances Relating to the Guidelines of 5 CFR 1320.5
The REACH IN system fully complies with the regulation.
8. Comments in Response to the Federal Register Notice and Efforts to Consult Outside the Agency
A. A copy of the Federal Register Notice required by 5 CFR 1320.8(d) was published on June 23, 2006 (volume 71, number 121, page 36096). Two public comments were received in response to this notice (see Attachment 2).
B. No effort was made to consult with persons outside the agency for this extension since no major changes to REACH IN were made. However, the following individuals were consulted during the initial development of the system:
Dr. Terrie Sterling
Behavioral Health Scientist
Centers for Disease Control and Prevention
National Center for Injury Prevention and Control
4770 Buford Highway, NE, MS K-60
Atlanta, GA 30341
770-488-1557
tsterling@cdc.gov
Dr. Robert Gold,
Dean of the College of Health & Human Performance
University of Maryland
2387 HHP Bldg, Valley Drive
College Park, MD 20742
301.405.2437
rsgold@umd.edu
Mr. Michael Bilton
Executive Director of the Association for Community Health Improvement Health Research and Educational Trust
One
North Franklin
Suite 2800
Chicago, IL 60606
(312)
422-2600
mbilton@aha.org
9. Explanation of Any Payment or Gift to Respondents
There is no payment to respondents, understanding that respondents are members of grantee organization staff or subcontractors who will use REACH IN to document their grant efforts.
10. Assurance of Confidentiality Provided to Respondents
The CDC Privacy Act Officer has reviewed this Request for OMB Clearance and determined that the Privacy Act is not applicable because personally identifiable information is not being collected through the “Racial and Ethnic Approaches to Community Health 2010 Information Network (REACH IN). Identifiable information related to licensed users of REACH IN is filed by the affiliate CDC REACH 2010 grantee organization and cannot be retrieved by the individual’s name.
REACH IN is designed to receive and process data from CDC’s REACH 2010 grantees, and does not specify data collection activities from individual respondents or ask questions of a sensitive nature. The program allows grantees to perform remote data entry and retrieval of data on the grantees’ evaluation activities related to capacity building, targeted action, community and systems change, and change among change agents. It is also designed to create on-demand graphs and reports of the grantees’ actions and accomplishments. The system may be used to meet the reporting requirement of their cooperative agreements with CDC. Users are allowed to enter contact information to facilitate communication within and between grantee organizations, however, users have the ability to make this contact information private (not viewable by other users).
For the purpose of identifying users, a login name and password is required for each user. This information is not available to anyone other than the user. REACH IN follows applicable governmental security guidance in the DHHS Automated Information Systems Security Program Handbook. Data submitted by grantees will be encrypted during transit. Grantees are advised to not submit and store personal data on the REACH IN site and the site is audited for such information. The REACH IN site does not itself collect personal information.
Individual contact information regarding licensed users of the site is maintained exclusively in electronic form on secured servers. This contact information includes the individual’s name, title, role, mailing address, email address, telephone number, and fax number. The user’s password and a hint question and answer are recorded for access purposes. Users are reminded that all information, except the login and password, is optional. But, other REACH 2010 users would have access to contact information if entered into this system.
REACH IN is processed on a stand-alone network protected by a firewall, entirely separate from local area networks (LAN), and will be processed on dedicated servers. Access to the server is restricted. There are no direct electronic connections between project data and other business information systems. Electronic access to REACH IN is password protected. The web site servers are housed in an access controlled room and security is also provided by physical isolation of the network.
11. Justification for Sensitive Questions
REACH IN does not specify data collection activities from individual respondents, and does not ask questions of a sensitive nature.
12. Estimates of Annualized Burden Hours and Costs
A. The total burden is estimated to be 84 hours, with the assumption of 42 respondent/grantee organizations, and 4 instances of using the system each year. The estimated burden table is provided below (Table A.12-1). This burden estimate was determined through experience developing and managing a similar system and through experience gained while pilot testing the REACH IN system.
Table A.12-1 Estimates of Annualized Burden to Respondents |
||||
Respondents |
No. of Respondents |
No. of Responses per Respondent |
Average Burden per Response (in hours) |
Total Burden (in hours) |
REACH 2010 Grantees |
42 |
4 |
30/60 |
84 |
Total |
|
|
|
84 |
B. The estimate of annualized cost to respondents is $992.00, as presented in the table below (Table A.12-2). This estimate is based on the assumption of respondents holding positions similar to the Bureau of Labor Statistics occupation title of Data Entry Keyers, with a mean hourly rate rounded up to $11.81.
Table A.12-2 Estimates of Annualized Costs to Respondents |
||||
Type of Respondents |
No. of Respondents |
Frequency of Responses |
Hourly Wage Rate |
Respondent Cost |
Data Entry Keyers |
42 |
4 |
$11.81 |
$992.00 |
Total |
|
|
|
$992.00 |
13. Estimates of Other Total Annual Cost Burden to Respondents or Record Keepers
There are no additional costs to respondents.
14. Annualized Cost to the Government
The average annual cost to the Government for design, development, maintenance, and management of the REACH IN system is $485,760. There are three years remaining in the contract, and the total three-year cost to the Government is $1,457,281. The figures below (Table A.14) indicate the cost category breakdown for the project-related expenditures.
|
|
Year 1 (09/01/2006 – 08/31/2007) |
Year 2 (09/01/2007 – 08/31/2008) |
Year 3 (09/01/2008 – 08/31/2009) |
Total |
Federal Government |
Project Officer |
$24,200 |
$24,200 |
$24,200 |
$72,600 |
Contract Specialist |
$18,700 |
$18,700 |
$18,700 |
$56,100 |
|
Labor |
Task 1. System Management; Task 2. Information Needs; Task 3. System Customization; Task 4. User Access and Support; Task 5. Training and Technical Assistance |
$421,103 |
$429,525 |
$438,116 |
$1,288,744 |
Other Direct Costs |
Travel and Subsistence; Office Expenses; Computer; Facilities and Equipment; Training/Meeting |
$11,934 |
$11,934 |
$11,934 |
$35,802 |
Total Indirect Cost |
G&A |
$1,345 |
$1,345 |
$1,345 |
$4,035 |
Total |
|
$477,282 |
$485,704 |
$494,295 |
$1,457,281 |
15. Explanation for Program Changes or Adjustments
No major changes have been made to the data information collection.
16. Plans for Tabulation and Publication and Project Time Schedule
This project does not use a statistical method, and there is no statistical analysis plan.
A.16-1 Project Time Schedule |
|
Activity |
Time Schedule |
REACH IN available for data entry |
Upon OMB approval |
Respondent data entry |
Quarterly, beginning four months after OMB approval |
Respondent reports due |
Semi-annually |
Publication |
12 to 18 months after OMB approval |
17. Reason(s) Display of OMB Expiration Date is Inappropriate
The OMB expiration date is displayed prominently on the website as required.
18. Exceptions to Certification for Paperwork Reduction Act Submissions
No exemptions from the certification statement are being sought.
B. Collections of Information Employing Statistical Methods
There are no applicable statistical methods involved in this project.
1. Respondent Universe and Sampling Methods
The respondent universe includes all REACH 2010 grantees using the REACH IN system. All are being provided secure access to the system for the purposes of quarterly data entry and semi-annual report creation. No sampling from this universe will be undertaken.
2. Procedures for the Collection of Information
Upon receipt of OMB approval, each respondent is notified of the availability of the system and each will enter data into the system at their own discretion. The staff is available to meet with or otherwise consult with each respondent to ensure the proper and most efficient use of the system.
3. Methods to Maximize Response Rates and Deal with Nonresponse
Response rate is maximized through the design and development of an inviting web-based application that is easy to use, and the use of which will ease the burden of grantees to fulfill their evaluation reporting requirements. Further, ongoing technical assistance by electronic mail, telephone, and in-person site visits encourage grantees to use the system. Nonresponse is addressed through regular system audits, which indicate the quantity of data being entered into the system by respondent while preserving the private nature of the data itself. Grantee organizations not using the system to an adequate level are contacted to encourage their use of the system and to provide input on ways to improve it.
4. Tests of Procedures or Methods to be Undertaken
Procedures for the collection of information in this extension are the same as those approved previously. REACH IN has been in use by 42 respondents since its initial approval. The use of REACH IN has decreased the burden on the respondents in that it is a means to produce their semi-annual evaluation report as required by their cooperative agreements with CDC. In addition, a single data collection system reduces error in the amount, validity, and reliability of information available to resource and policy decision makers from the community and government, including CDC.
5. Individuals Consulted on Statistical Aspects and Individuals Collecting and/or Analyzing Data
No statistical analysis is undertaken for this effort and therefore individuals were not consulted on the statistical aspects of the project.
The following individuals will oversee data collection:
Andrea M. Hegedus, Ph.D.
Northrop Grumman
CDC, NCCDPHP
770-488-5445
Dianne Fragueiro (contractor)
ORC Macro
301-572-0927
List of Attachments
Attachment 1. Authorizing Legislation
Attachment 2. Published 60 Day Federal Register Notice, Question/Comment and Responses
Attachment 3. REACH 2010 Information Network Design Document
ATTACHMENT 1
AUTHORIZING LEGISLATION
Public Health Service Act.
Title 42. United States Code.
Chapter 6A - Public Health Service.
Subchapter II - General Powers and Duties.
Section 241. Research and Investigation
A.Sec. 301 [Sec. 241] (a) The Secretary shall conduct in the Service, and encourage, cooperate with, and render assistance to other appropriate public authorities, scientific institutions, and scientists in the conduct of, and promote the coordination of, research, investigations, experiments, demonstrations, and studies relating to the causes, diagnosis, treatment, control, and prevention of physical and mental diseases and impairments of man, including water purification, sewage treatment, and pollution of lakes and streams. In carrying out the foregoing the Secretary is authorized to -
collect and make available through publications and other appropriate means, information as to, and the practical application of, such research and other activities;
make available research facilities of the Service to appropriate public authorities, and to health officials and scientists engaged in special study;
make grants-in-aid to universities, hospitals, laboratories, and other public or private institutions, and to individuals for such research projects as are recommended by the advisory council to the entity of the Department supporting such projects and make, upon recommendation of the advisory council to the appropriate entity of the Department, grants-in-aid to public or nonprofit universities, hospitals, laboratories, and other institutions for the general support of their research;
secure from time to time and for such periods as he deems advisable, the assistance and advice of experts, scholars, and consultants from the United States or abroad;
for purposes of study, admit and treat at institutions, hospitals, and stations of the Service, persons not otherwise eligible for such treatment;
make available, to health officials, scientists, and appropriate public and other nonprofit institutions and organizations, technical advice and assistance on the application of statistical methods to experiments, studies, and surveys in health and medical fields;
enter into contracts, including contracts for research in accordance with and subject to the provisions of law applicable to contracts entered into by the military departments under sections 2353 and 2354 of title 10, except that determination, approval, and certification required thereby shall be by the Secretary of Health and Human Services; and
adopt, upon recommendations of the advisory councils to the appropriate entities of the Department or, with respect to mental health, the National Advisory Mental Health Council, such additional means as the Secretary considers necessary or appropriate to carry out the purposes of this section.
The Secretary may make available to individuals and entities, for biomedical and behavioral research, substances and living organisms. Such substances and organisms shall be made available under such terms and conditions (including payment for them) as the Secretary determines appropriate.
(b) (1) The Secretary shall conduct and may support through grants and contracts studies and testing of substances for carcinogenicity, teratogenicity, mutagenicity, and other harmful biological effects. In carrying out this paragraph, the Secretary shall consult with entities of the Federal Government, outside of the Department of Health and Human Services, engaged in comparable activities. The Secretary, upon request of such an entity and under appropriate arrangements for the payment of expenses, may conduct for such entity studies and testing of substances for carcinogenicity, teratogenicity, mutagenicity, and other harmful biological effects.
(2) (A) The Secretary shall establish a comprehensive program of research into the biological effects of low-level ionizing radiation under which program the Secretary shall conduct such research and may support such research by others through grants and contracts.
(B) The Secretary shall conduct a comprehensive review of Federal programs of research on the biological effects of ionizing radiation.
(3) The Secretary shall conduct and may support through grants and contracts research and studies on human nutrition, with particular emphasis on the role of nutrition in the prevention and treatment of disease and on the maintenance and promotion of health, and programs for the dissemination of information respecting human nutrition to health professionals and the public. In carrying out activities under this paragraph, the Secretary shall provide for the coordination of such of these activities as are performed by the different divisions within the Department of Health and Human Services and shall consult with entities of the Federal Government, outside of the Department of Health and Human Services, engaged in comparable activities. The Secretary, upon request of such an entity and under appropriate arrangements for the payment of expenses, may conduct and support such activities for such entity.
(4) The Secretary shall publish a biennial report which contains -
(A) a list of all substances ( i ) which either are known to be carcinogens or may reasonably be anticipated to be carcinogens and ( ii ) to which a significant number of persons residing in the United States are exposed;
(B) information concerning the nature of such exposure and the estimated number of persons exposed to such substances;
(C) a statement identifying (i) each substance contained in the list under subparagraph (A) for which no effluent, ambient, or exposure standard has been established by a Federal agency, and
(ii) for each effluent, ambient, or exposure standard established by a Federal agency with respect to a substance contained in the list under subparagraph (A), the extent to which, on the basis of available medical, scientific, or other data, such standard, and the implementation of such standard by the agency, decreases the risk to public health from exposure to the substance; and
(D) a description of (i) each request received during the year involved -
(I) from a Federal agency outside the Department of Health and Human Services for the Secretary, or
(II) from an entity within the Department of Health and Human Services to any other entity within the Department, to conduct research into, or testing for, the carcinogenicity of substances or to provide information described in clause (ii) of subparagraph (C), and (ii) how the Secretary and each such other entity, respectively, have responded to each such request.
(5) The authority of the Secretary to enter into any contract for the conduct of any study, testing, program, research, or review, or assessment under this subsection shall be effective for any fiscal year only to such extent or in such amounts as are provided in advance in appropriation Acts.
(c) The Secretary may conduct biomedical research, directly or through grants or contracts, for the identification, control, treatment, and prevention of diseases (including tropical diseases) which do not occur to a significant extent in the United States.
(d) Protection of privacy of individuals who are research subjects
The Secretary may authorize persons engaged in biomedical, behavioral, clinical, or other research (including research on mental health, including research on the use and effect of alcohol and other psychoactive drugs) to protect the privacy of individuals who are the subject of such research by withholding from all persons not connected with the conduct of such research the names or other identifying characteristics of such individuals. Persons so authorized to protect the privacy of such individuals may not be compelled in any Federal, State, or local civil, criminal, administrative, legislative, or other proceedings to identify such individuals.
ATTACHMENT 2
PUBLISHED 60- DAY
FEDERAL REGISTER NOTICE
QUESTION/COMMENT AND RESPONSES
[Federal Register: June 23, 2006 (Volume 71, Number 121)] [Notices] [Page 36096]
From the Federal Register Online via GPO Access [wais.access.gpo.gov]
[DOCID:fr23jn06-49]
=======================================================================
DEPARTMENT OF HEALTH AND HUMAN SERVICES
Centers for Disease Control and Prevention
[60Day-06-0603]
Proposed Data Collections Submitted for Public Comment and Recommendations
In compliance with the requirement of section 3506(c)(2)(A) of the Paperwork Reduction Act of 1995 for opportunity for public comment on proposed data collection projects, the Centers for Disease Control and Prevention (CDC) will publish periodic summaries of proposed projects. To request more information on the proposed projects or to obtain a copy of the data collection plans and instruments, call 404-639-5960 and send comments to Seleda Perryman, CDC Assistant Reports Clearance Officer, 1600 Clifton Road, MS-D74, Atlanta, GA 30333 or send an e-mail to omb@cdc.gov.
Comments are invited on: (a) whether the proposed collection of information is necessary for the proper performance of the functions of the agency, including whether the information shall have practical utility; (b) the accuracy of the agency's estimate of the burden of the proposed collection of information; (c) ways to enhance the quality, utility, and clarity of the information to be collected; and (d) ways to minimize the burden of the collection of information on respondents, including through the use of automated collection techniques or other forms of information technology. Written comments should be received within 60 days of this notice.
Proposed Project
Information Network (REACH IN)--Extension (0920-0603)--National Center for Chronic Disease Prevention and Health Promotion (NCCDPHP), Centers for Disease Control and Prevention (CDC).
Background and Brief Description
Racial and Ethnic Approaches to Community Health 2010 (REACH 2010) currently funds forty local coalitions to establish community based programs and culturally appropriate interventions to eliminate racial and ethnic health disparities. Two previously funded grantees also retain access to the system. Communities served by REACH 2010 include: African American, American Indian, Hispanic American, Asian American, and Pacific Islander. These communities can select among infant mortality, deficits in breast and cervical cancer screening and management, cardiovascular diseases, diabetes, HIV/AIDS, and deficits in childhood and adult immunizations to be the focus of their interventions. Guided by logic models, each community articulates goals, objectives, and related activities; tracks whether goals and objectives are met, ongoing, or revised; and evaluates all program activities. This information is then entered into the REACH Information Network (REACH IN). REACH IN is a customized Internet-based support system that allows REACH 2010 grantees to perform remote data entry and retrieval of data.
This support system is designed to create on-demand graphs and reports of grantees' activities and accomplishments, monitor progress toward the achievement of goals and objectives, and share and synthesize information across grantees' activities. Both quantitative and qualitative analyses can be performed. These analyses relate primarily to three stages of the REACH 2010 logic model: Capacity building targeted actions (interventions), and community and systems change and change among change agents. Users are supported with technical assistance and training, covering the usage of the system from a content/project goals perspective, and technical operations.
The annualized estimated burden is based on 42 respondents, including 40 currently funded grantees and two that were funded previously who retain access to the system. It is estimated that they each use the system four times a year to enter data, each data entry taking about 30 minutes. There are no costs to respondents except their time to participate.
Estimated Annualized Burden Hours
---------------------------------------------------------------------------------------------------
Number of Average burden
Respondents Number of responses per per response Total burden
respondents respondent (in hrs.) hours
-------------------------------------------------------------------------------------------------------------------------------------------
REACH 2010 grantees...............42 4 30/60 84
--------------------------------------------------------------------------------------------------------------------------------------------
Dated: June 15, 2006.
Joan F. Karr,
Acting Reports Clearance Officer, Centers for Disease Control and Prevention.
[FR Doc. E6-9919 Filed 6-22-06; 8:45 am]
BILLING CODE 4163-18-P
Comment/Question and Responses to the Publication
Of the 60 Day Federal Register Notice
Comment 1.
i
think the focus of spending of u.s. tax dollars should be on benefits
for majority of u.s. population and which impact all peoples, not
just some. i think the selection of funnelling u.s.t ax dollars
to hand selected minorities is against the principles of democracy -
projects should benefit all - not just some.
b. sachau
15
elm st
florham park nj 07932
Thank you for your comment regarding federal register of 6/23/06 vol. 71 #121 pg 36096.
One of the biggest failures of our society and the healthcare system is that a large proportion of American citizens do not receive adequate health care. For example, Native Americans die at higher rates than other Americans from tuberculosis (600% higher) and diabetes (189% higher). National infant mortality among Black infants occurred at a rate of 13.6 per 1,000 live births, which is almost double the national average. Vietnamese women have five times the rate of cervical cancer compared with White women.
Racial and Ethnic Approaches to Community Health 2010 attempts to eliminate these and other health disparities by strengthening American communities. By changing communities, work is underway to increase access to the healthcare system and implement initiatives to promote healthier lifestyles. In these ways, REACH 2010 seeks to improve the health of Americans who otherwise would not receive adequate health care. Please visit our website at www.cdc.gov/REACH2010 for additional details.
Question 2.
1. Is client-level data collected? If so, is it identifiable? If not, how is it de-identified?
No client level data are collected through this system. REACH IN is designed to collect data on the community coalition's activities addressing health disparities. This system also collects data on community changes and progress in meeting the goals and objectives of this cooperative agreement. Other data, such as the project's evaluation and sustainability plans, also are collected. This system assists the grantees with preparing community level reports and with meeting their reporting requirements to CDC .
2. Is this data transmitted to CDC? If so, how is the security of the data transmission assured?
These data are collected via a web-based system developed by a CDC contractor. REACH IN is a support system that allows remote data entry and reporting from each community site. Both CDC and grantees have access to the system. The contractor is very experienced in the design and security of such systems. Security measures include a stand-alone network protected by a firewall, dedicated servers, login and password protections, and all data are encrypted during transit. REACH IN follows applicable government security guidance in the DHHS Automated Information Systems Security Program Handbook.
ATTACHMENT 3
DESIGN DOCUMENT
Form: Approved
OMB No.: 0920-0603
Exp. Date: 12/31/06
REACH 2010 Information Network
Design Document
October 30, 2006
Prepared for:
Public Health Service
Centers for Disease Control and Prevention
Atlanta, GA
Prepared by:
ORC Macro
11785 Beltsville Drive
Calverton, MD 20705
CDC Contract #
Public reporting burden of this collection of information is estimated to average 60 minutes per response, including the time for reviewing instructions, searching existing data sources, gathering and maintaining the data needed, and completing and reviewing the collection of information. An agency may not conduct or sponsor, and a person is not required to respond to a collection of information unless it displays a currently valid OMB control number. Send comments regarding this burden estimate or any other aspect of this collection of information, including suggestions for reducing this burden to CDC/ATSDR Reports Clearance Officer; 1600 Clifton Road NE, MS D-74, Atlanta, GA 30333; ATTN: PRA (0920-0603)
Table of Contents
3.1 Content Grouping and Labeling 6
3.6 Objectives and Measures 10
3.8 Reports 15
The Centers for Disease Control and Prevention began working with ORC Macro to customize an existing Internet-based outcomes-based application to facilitate their efforts with Racial and Ethnic Approaches to Community Health (REACH) 2010 grantees (the users). This design document guides the development of the customized REACH Information Network (REACH IN) system and is the basis for incorporating any modifications.
This design document begins by articulating the goals of the web-based application, discussing the anticipated user experience, outlining the site contents, presenting the site structure, and demonstrating the visual design of the application.
Comments and questions regarding this design document and the developing web application should be emailed to feedback@reach2010.net.
The purpose of the REACH IN is to provide an Internet-based data warehousing application that will enable REACH 2010 grantees to document and organize their activities related to their organization and community efforts. These efforts are related to three stages of the REACH project logic model:
Capacity building,
Targeted actions,
Community and system changes and change among change agents.
The primary goals of REACH IN include the following:
Provide data entry, storage, management, retrieval, and reporting and interactive graphing functions of qualitative and quantitative data.
Document grantee coalitions’ current resources, identify specific needs, and document efforts and outcomes to build organization and community capacity so that existing resources match identified needs.
Capture qualitative and quantitative information and data about a coalition's actions and interventions, targeted indicators of change, and indicator data tracking.
Track indictor data related to change among influential individuals or groups.
Monitor public health indicator outcomes related to each coalition’s identified health priority area.
Facilitate internal and cross-coalition learning, including information sharing.
Produce reports about grantee activities following CDC prescribed formats.
Allow grantee to produce reports following custom formats for their own purposes.
Three primary audience segments will use and benefit from the REACH IN.
CDC Project Officer and Program Consultants. The interests of this audience segment include monitoring the grant-related activities of the users; evaluating the extent of system use; evaluating the efficacy of providing a web-based data warehousing tool for effective capacity building, targeted actions, and community and systems changes and change among change agents; and analyzing aggregate data to assess and monitor grantee activity effectiveness for reducing health disparities.
Grantee Coalitions. This broad audience segment contains several likely types of end users, including project directors, evaluators, principal investigators, project staff, and interested members of the grantee communities. Each of the first three types of users in this segment can be further differentiated as those who are likely to frequently use the system for data entry, activity monitoring, and/or reporting versus those who are most likely interested in occasional browsing through the system.
Others. There are potentially other audience segments, including other federal and State grant making administrators and officials who may look to CDC for insight regarding the use of web-based tools for grantee monitoring, reporting, training, and technical assistance. There may be other community members who are interested in CDC activities or whose interest stems from concern regarding health disparities. Users from these segments typically will require an experience similar to interested community members. That is, read-only access to the system will be necessary for certain public areas and editing access will not be available usually.
The site provides the following functional requirements:
Allow users to enter and retrieve narrative (i.e., qualitative) data related to activity processes.
Allow users to enter and retrieve statistical (i.e., quantitative) data related to activity process.
Allow users to interrelate qualitative and quantitative data related to a single activity.
Allow users to relate qualitative and quantitative data across multiple activities.
Display data in textual, tabular, and graphic formats.
Incorporate quality control checks and validation processes at the time of data entry.
Incorporate quality control checks and validation processes for contractor and client review and follow-up.
Various levels of security allowing users control of which users to provide read-only, read and write, or no access (public or private).
File upload and storage capability for word processing, graphic, and spreadsheet files, but excluding executable program files, to a file library shared within grantee organization.
Ability to attach previously uploaded files from the grantee library to various places within the system.
3.1 Content Grouping and Labeling
Content within REACH IN will be grouped under the following headings:
Grantee
Project
Capacity Building
Targeted Action
Community and Systems Changes
Change Among Change Agents
Indicator Library
Data Sets
Reports
Resources
Exhibit 3-1. LOG IN Home Page
Grantee Organization information includes the Grantee Name and a brief description of the grantee’s REACH 2010 project. In addition, the grantee’s primary and secondary health priority areas, target population, and State are displayed. The designated grant administrator has the ability to edit the information on this page for their community.
The Grantee Information page contains a link to a Public Grantee Report. This link directs to a page displaying an extraction of the publicly available information for this community. In this way, and only in this way, a member of one grantee organization can view the REACH 2010 available information from another grantee.
A list of REACH IN licensed users for the grantee organization appears on this page. Users can edit their own contact information and specify if their contact information is public (viewable by other REACH IN users) or private (not viewable by others). The Grantee Information page also contains a list of Coalition Partners. Both of these lists are present to facilitate communication within and across grantees.
The system assists in the task of maintaining a list of licensed members of the local grantee coalition who have access to the system.
Data elements include all standard contact fields and the level of the individual’s access (read only, full edit rights).
When users enter or edit their contact information, they specify whether their contact information is to be public (and available to all other licensed REACH IN users) or private (and not accessible to others).
Exhibit 3.2 Grantee Information Page
Grantees can create a Project. A Project is the primary organizational root of the documentation entered by the users. A Project has Goals and Objectives. The Goals and Objectives are categorized within one of the four stages areas defined by the REACH 2010 evaluation logic model. In addition, a Project can have an unlimited number of Activities and Subactivities attached, like Goals and Objectives each Activity falls within one of the four stage areas according to the REACH 2010 logic model. A Project and its Activities can have an unlimited number of Measures, Progress Notes and (sub) Activities attached to them.
Data elements for a Project include Project Name, Principle Investigator, Cooperative Agreement number, Period of Performance, Abstract, Evaluation Plan, Primary and Secondary Health Priority Areas, Project Measures(s), and Progress Notes.
Access to the Project Information page is limited to the logged in user’s REACH IN community area.
Grantees need to document their progress as each Project is developed and as each Activity is planned and implemented. The system allows for the easy entry of sequential Progress Notes for both Projects and Activities.
Data elements for Progress Notes include: Note Name, Automatic Date Stamp (editable), Sharing Status (Public, or available in the Public Grantee Report; Private, or only available to members of the same Grantee community), and Note Contents.
Exhibit 3-4. Progress Notes Edit Page
Stages, Goals, Objectives and Activities
Objectives, and activities represent the plans and efforts to improve the readiness or ability of a coalition and its members to take action aimed at changing risk/protective behaviors, and transforming community conditions and systems so that a supportive context exists to sustain behavior changes over time. The system allows for Grantees to document their Goals and Objectives. The process for adding Goals and Objectives to a stage is similar across Stages.
3.5 Stages and Activities
The navigation bars on the left side of the browser window include links to pages representing each of the REACH 2010 evaluation stages. It is on these pages that the user enters new activities, by default adding each to the stage the user is working within. Stages include: (a) Capacity Building, (b) Targeted Action, (c) Community and Systems Changes and (d) Change Among Change Agents. Sidebars have different text and resources available, but the operation and fields for adding Goals, Objectives and Activities to a stage are similar across the Stages.
The first view of each Activity page is a list of the Activities previously entered.
Levels of Activities and (sub) Activities are viewable through an expand/collapse control. The default view will be fully expanded.
Only owners, i.e., the user who created an Activity or (sub) Activity can move the Activity.
On each edit form for each root Activity, there is an interface for deciding (a) whether other grantee organizations can view the Activity and all nested (sub) Activities, and (b) whether other members of the same grantee organization can (i) view only or (ii) view, copy, edit, and delete, and add (sub) Activities.
Each Activity and (Sub) Activity has data inputs for actual and targeted start and end dates.
Data elements for Activities include Activity Name, Description, Target Start Date, Target End Date and Actual End Date.
Future customizations and enhancements to REACH IN may include the following features related to copying and moving Activities.
Users are able to change the Stage of an Activity once it has been created. This function occurs on the edit form for any Activity.
Users are able to copy and/or move any Activity they created. Users are able to copy, and then move, any Activity for which they have been given permission by the owner/creator of the Activity (i.e., no user is able to move another user's Activity, but are able to create a copy, which they then own, and move that Activity).
If an Activity is moved, and that Activity has attached (sub) Activities, all attached, or nested, levels are moved as well.
Users can change the level at which an Activity is created. That is, a (sub) Activity can be moved "up" and become an Activity.
If a (sub) Activity is moved to the root position, permissions are automatically set based on the permissions from its former root.
Future customized features may also include:
Users are able to filter the view of Activities on the screen by indicating a status value. Status is controlled on the edit form and include the values of planned, active, and complete.
The Activity view can include/exclude based on status values.
There will be 3 types of Objectives: Health Priority Objectives, Community Level Objectives and Process Objectives. For Health Priority Objectives, there is a standard of categories, which include the 6 health priority areas within the REACH program.
EXHIBIT 3-6-1. Health Priority Objectives
Categories for Community Level Objectives are provided. Community Level Objectives are adapted from the Outcomes Toolkit web-based application (www.ACT-Toolkit.com).

Exhibit 3-6-2. Process Objectives List
A standard set of Process Objective categories are provided and include the following: Attendance, Level of Exposure, Satisfaction, Fidelity, Level of Effort, Resource Utilization, Quality Assurance, and Environmental Influences. Users are able to add and categorize their own Process indicators.
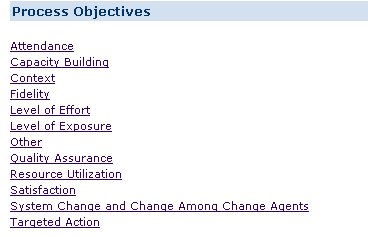
Exhibit 3-6-3. Process Indicators Category List
Features of the Indicator Library include the following:
Indicators are listed alphabetically within each category.
REACH 2010 Objective Indicators have been developed based on Healthy People 2010 and the Outcomes Toolkit.
Sample Community Level Objective Indicators are developed based on standard public health process measures.
Users are not able to change or add Indicators.
Users are able to create new custom Measures.
Users are not able to make the Measures public, i.e., other users in other grantee coalitions are not able to see custom created Measures.
The system currently has over 200 Measures in the Indicator Library. ORC Macro will add any additional Indicators for use by all grantee users if suggested by a grantee, CDC or other responsible source, upon CDC's approval.
System standard Measures are distinguished from custom created measures by displaying the latter in a bold font.
Data elements for Indicators Measures include: Objective, Indicator, Measure Name, Measure, Background, Data Type (number, ratio/percent/rate, index, text), Denominator, Measure Definition, Key Words and Access Information (to specify the level of access for others in the same REACH IN community).
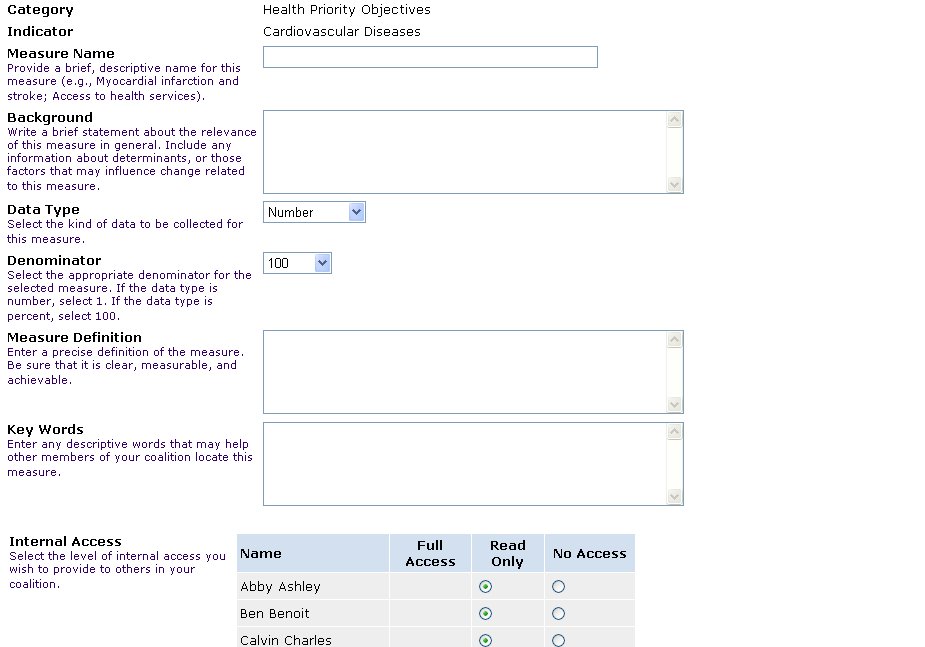
Exhibit 3-6-4. Indicator Measure Edit or Add Page
Data elements for attached Measures (i.e., those Measures that have been identified as relevant and in use for a specific Activity) additionally include Baseline Data Value, and Target Data Value.
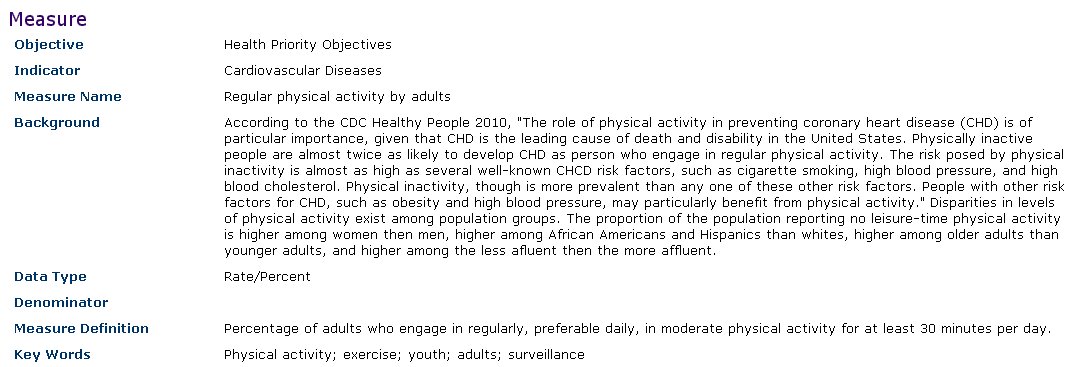
Exhibit 3-6-5. Indicator Display Page
Grantees enter numerical data to be connected to the Project and its (Sub) Activities through the relationship to a specific Indicator. The Data pages of the REACH IN system allow users to define a Data Set. From each Data Set, the user can generate several Data Tables by specifying which variables and which values of each variable are displayed. The user specifies which selected variable will be displayed as the row heading and which will be the column heading. When multiple variables are selected for table rows or columns, the user specifies which variables will be nested within others.
As an example, a user may create a data set for the number of newly diagnosed cases of diabetes for certain ethnic groups within certain Census tracts by the age of each patient. Each variable in this example (e.g., ethnicity, Census tract, and age) have values. The values for age, for instance, could be ten-year increments covering the life span. The user then enters known data corresponding to the definition of each cell in the Data Table. When working with the Project or (Sub) Activities, and a user specifies the same Measure (number of newly diagnosed cases of diabetes), this Data Set is automatically available with its associated Data Tables.
Data elements for Data Sets include Name, Measure Name, Measure, and Access Information (to specify the level of access for others in the same REACH In community).
Data elements for Tables include Name, specified Variables and included Variable Values. Because Data Tables are a specified subset of the contents of a Data Set, the Data Set Measure details are associated.
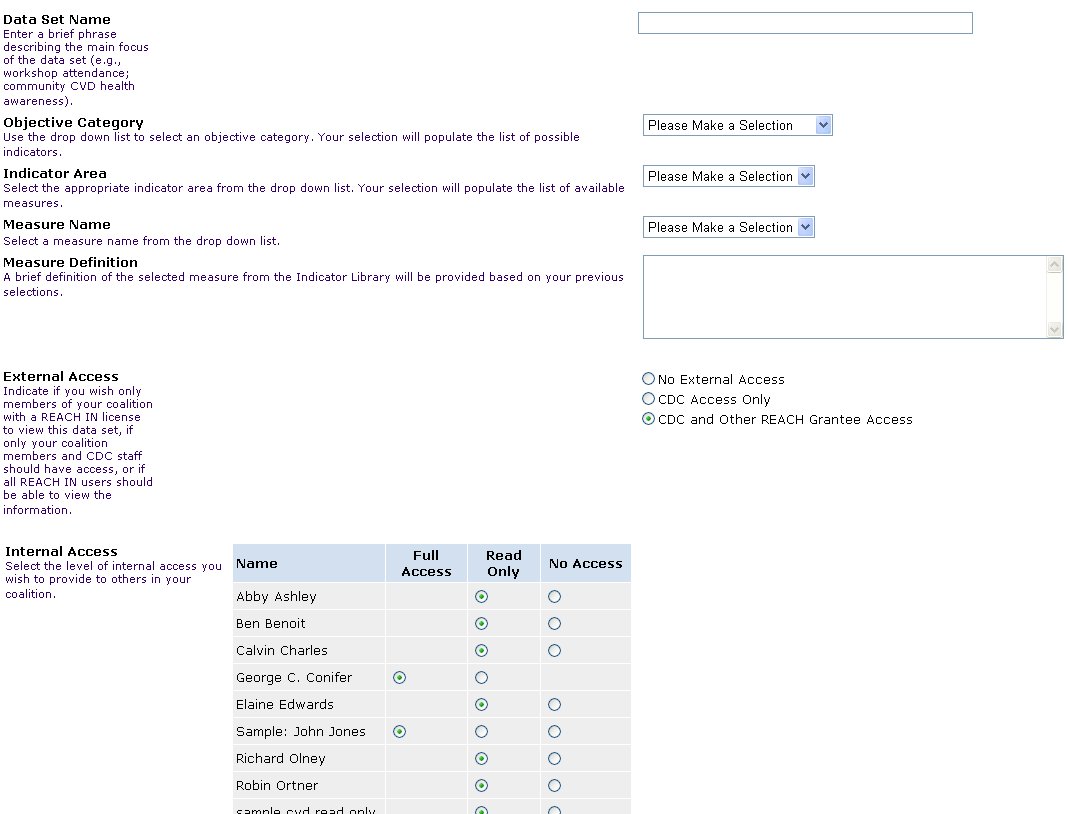
Exhibit 3-7-1. Data Table Edit Form
A future customization of the system will include the following features:
The data value can be entered with denominator value to convert the data to a rate.
The system will allow several summary statistics to be displayed in data reports, including: % of row or column; average of row or column; and total by row or column.
The system could include other basic statistics, such as row and column total, mean, and standard deviations.
Each Data Table can be displayed in graphic form. For this, the user-specified measure is treated as the Y-axis variable and the selected variables are displayed appropriately along the X-axis. Graph types include bar, pie, and line charts.
The preceding section presents how quantitative data are stored and displayed in Data Sets and Tables in REACH IN. Qualitative data are stored throughout the system in the form of the Project and (Sub) Activity descriptions and associated Progress Notes. Additionally, qualitative data can be converted into quantitative data for graphical display. For instance, users are able to place a numerical rating on the stated or perceived extent to which change has occurred among change agents (recalling that the Y-axis of graphs are derived from the Measure).
REACH IN is able to generate several types of reports of the data they have entered. For users, a standard report template exists for developing the evaluation reports required by CDC as part of each grantee’s cooperative agreement. This report follows the format provided by CDC and semi-automatically draws from the data entered by the user to collate into a document. This report is a comprehensive listing of the data entered into the system by the user and specified for CDC’s consumption.
Additionally, users are able to develop project reports following user-specified formats. That is, when developing a report, the user is able to identify which data elements to include or exclude in a report. For example, the user may wish to bring together in a report all the progress notes related to any Capacity Building effort within a specified time frame. Report results are saved in the system for future use.
Future customization possibilities include:
Activity planning dependency reports, based on the user-specified start and end dates. That is, certain Activities may not be able to be started or completed until certain other Activities are begun or finished. If data were entered into the system suggesting otherwise, the discrepancy report would identify the conflict. For example, a PSA would have to be developed before it could be aired. Similarly, a workshop’s curriculum would need to be outlined, developed, piloted, and revised before it could be fully implemented.
Narrative reports comprised of filtered or otherwise selected Progress Notes.
Combination of Indicators reports, allowing users to display multiple measures on one graph. Measures can only be compared if they share at least one variable. It must be the actual variable, not just something with the same name. The user can choose to graph rate, actual values or percent of target.
Reports depicting a Gantt chart view of all activities and sub-activities.
CDC reports are primarily designed to allow comparison across grantees, either of a specified set of grantees or to develop the aggregate of efforts. For example, CDC may wish to compare the approaches by two or more grantee organizations that share a common health priority area. Or, CDC may wish to quantify the number of Targeted Action Activities undertaken in a given month by all grantees. These comparative reports will only be available to CDC staff.
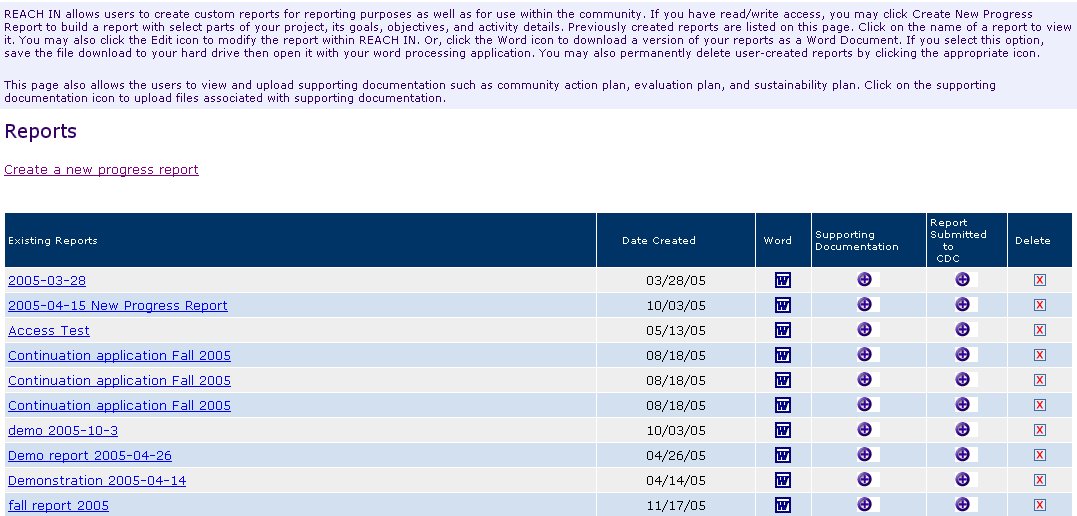
Exhibit 3-8-1. User Report List
The following is an example of what a user’s progress report might contain.
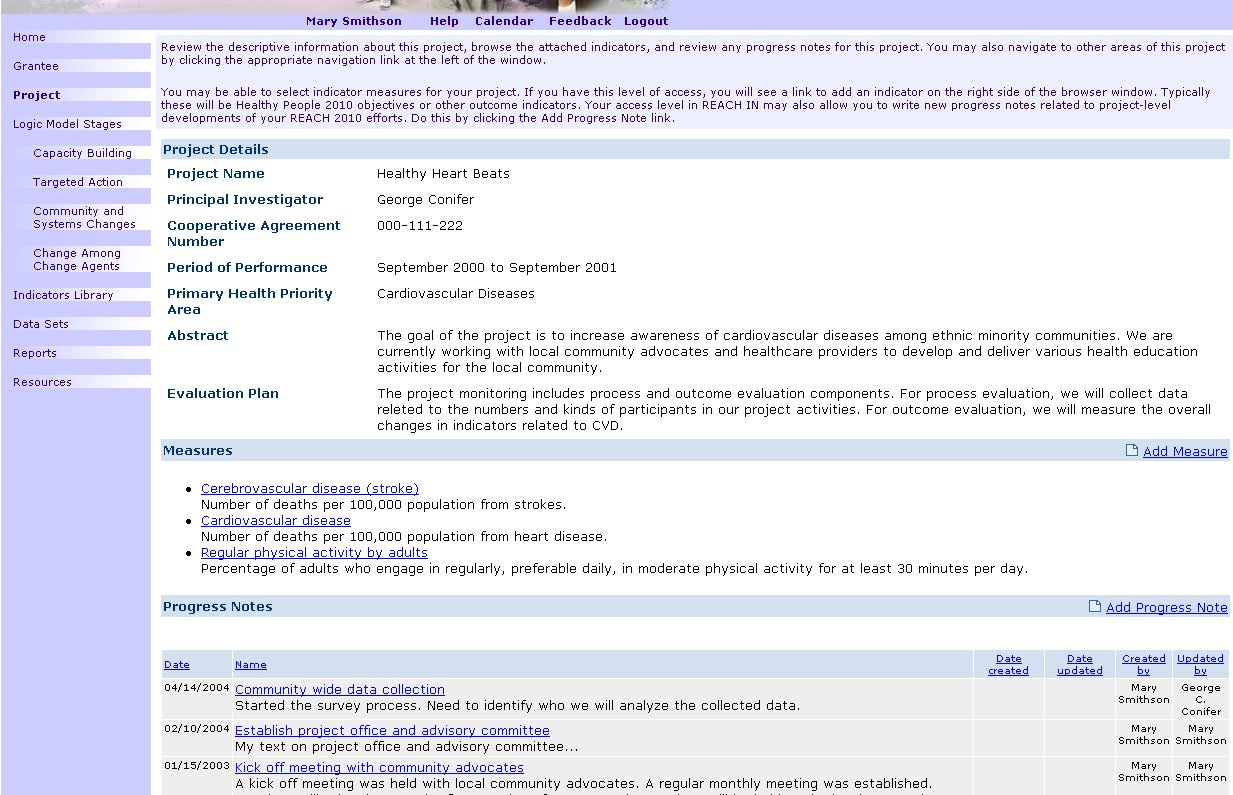
EXHIBIT 3-8-2. Sample Progress Report
Several resources are available on REACH IN for users, including
Calendar, a resource for users to post important events online. The calendar is specific to each REACH IN community.
File Library, a feature allowing users to upload and download nonexecutable files (e.g., .doc, .pdf, .gif) for sharing within the grantee community.
Search, a feature which allows users to easily locate a text string on the site. Searching will be of most name and description fields in the system.
Glossary, which defines key terms for users, encouraging full understanding and consistent use of specialized terms relevant to the REACH 2010 project.
4.1 Global and Local Navigation Systems
The following graphic presents a schematic view of the REACH IN web site (see Exhibit 4-1-1). Global navigation is accomplished through the links along the left side of the browser window. Additional administrative and other functional areas are accessible through links along the top of the browser window and below the banner. The following graphic presents the basic page layout and navigation system within REACH IN (see Exhibit 4-1-2).
Local navigation is accomplished a variety of ways, but mainly through hyperlinked item names. For example, a capacity building activity name brings up a display page with the details connected to the linked name. Icons control expanding and collapsing functionality.
Ex 4-1-1. Layout Design and Global Navigation
E x
4-1-2. Site Schematic Illustration
x
4-1-2. Site Schematic Illustration
The REACH IN system has two servers, an SQL database server and a web-services server. The web-services server handles security and access for users’ accessing the web pages. The database server stores user input and provided data to the web-services server.
To access the system, users a required to use an Internet-connected computer, preferably with a T1 connection, using Microsoft Internet Explorer 5.0 or higher, or Netscape 4.7 or higher, with Javascript enabled.
The current Web-based prototype system resides at www.reach2010.net.
42USC241
| File Type | application/msword |
| Author | HVD5F |
| Last Modified By | zfa4 |
| File Modified | 2006-12-04 |
| File Created | 2006-12-04 |
© 2026 OMB.report | Privacy Policy